Cannonball Metastases of the Lung: An Unusual Initial Manifestation of Endometrial Carcinoma
Midila Bapineni, Shivendra Tangutoori, Naga Vamsi Krishna Machineni, Kamlesh Sajnani, Maneesh Gaddam

TL;DR
A rare case of endometrial cancer presenting with unusual large lung metastases is reported, emphasizing the importance of recognizing this atypical symptom for timely treatment.
Contribution
This case report highlights the rare initial manifestation of endometrial carcinoma as cannonball pulmonary metastases, expanding diagnostic awareness.
Findings
Endometrial carcinoma presented with multiple large 'cannonball' lung metastases in a 60-year-old woman.
Chemotherapy with carboplatin and paclitaxel led to significant regression of metastases and symptom improvement.
Maintenance therapy with anastrozole achieved stable disease, demonstrating a treatment pathway for this rare presentation.
Abstract
Endometrial carcinoma is the most common gynecologic malignancy in developed countries and is typically diagnosed at an early stage, with distant metastases uncommon at presentation. Pulmonary involvement occurs in less than 5% of cases and usually manifests as small nodules or interstitial disease; the appearance of multiple, large, round ‘cannonball’ metastases is exceptionally rare. We report the case of a 60‐year‐old woman who presented with cough and dyspnea. Imaging revealed numerous bilateral pulmonary ‘cannonball’ nodules, mediastinal lymphadenopathy, hepatic lesions, and an enlarged uterus. Endometrial biopsy confirmed endometrioid adenocarcinoma, staged as FIGO IV‐B. The patient underwent chemotherapy with carboplatin and paclitaxel, resulting in significant regression of pulmonary and hepatic metastases and symptomatic improvement, followed by maintenance therapy with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
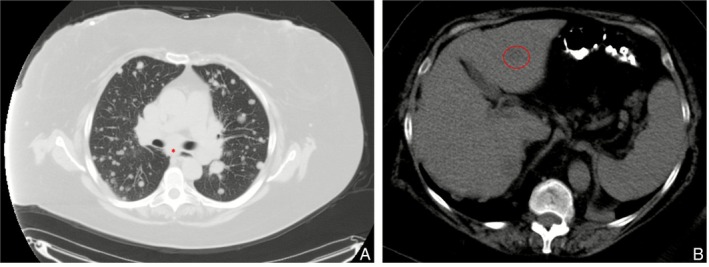 FIGURE 1
FIGURE 1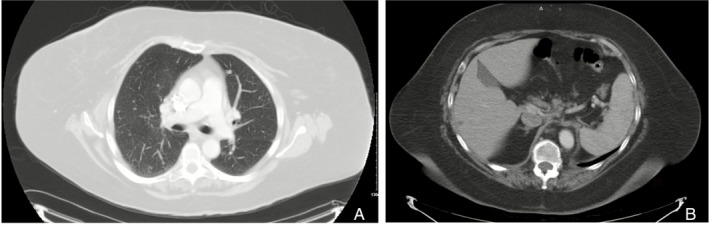 FIGURE 2
FIGURE 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEndometrial and Cervical Cancer Treatments · Cancer Diagnosis and Treatment · Ovarian cancer diagnosis and treatment
Introduction
1
Endometrial carcinoma is the most common gynecologic malignancy in developed countries and a leading cancer among women worldwide [1]. Most cases are detected early due to abnormal uterine bleeding, especially in postmenopausal women, and have favorable outcomes with five‐year survival exceeding 90%. In contrast, advanced or metastatic disease is less common and carries a markedly worse prognosis, with pulmonary metastases reported in only 2.3%–4.7% of patients [2, 3]. These metastases usually appear as small nodules or interstitial changes; large, well‐defined ‘cannonball’ lesions are exceedingly rare. The term ‘cannonball metastases’ describes multiple, round, sharply circumscribed pulmonary nodules resembling historical artillery fire and is classically associated with renal cell carcinoma, choriocarcinoma, and occasionally breast or colorectal carcinoma [4, 5]. Infectious or autoimmune conditions may mimic this radiographic pattern, but gynecologic primaries seldom do. We report a rare case of endometrial carcinoma that initially presented with respiratory symptoms, where progressive cough and dyspnea led to the discovery of widespread cannonball pulmonary metastases on imaging.
Case Report
2
A 60‐year‐old woman with no prior medical history and a lifetime non‐smoker presented to her primary physician with a persistent nonproductive cough. She was empirically treated with antibiotics for presumed bronchitis, but her symptoms persisted and gradually progressed to exertional dyspnea. She denied fever, chills, hemoptysis, chest pain, weight loss, or systemic complaints.
Chest radiograph was abnormal, prompting a computed tomography (CT) scan that demonstrated numerous, well‐circumscribed pulmonary nodules ranging from a few millimetres to 2 cm, distributed both peripherally and diffusely, along with mediastinal lymphadenopathy measuring up to 2.8 cm in the subcarinal region (Figure 1A). CT of the abdomen showed low‐attenuation hepatic lesions measuring 1.3 and 1.9 cm, as well as an enlarged uterus (6.4 cm) (Figure 1B), raising suspicion for metastatic disease.
(A) Multiple bilateral “cannonball” pulmonary nodules with enlarged subcarinal lymphadenopathy(). (B) Low‐attenuation lesion in the left hepatic lobe.*
At this stage, the differential diagnosis for multiple pulmonary nodules included metastatic malignancy, infections, inflammatory disorders, and vasculitides such as granulomatosis with polyangiitis. However, the clinical context strongly supported a metastatic aetiology. The patient lacked infectious symptoms, had no risk factors or features suggestive of tuberculosis or GPA, and the ancillary imaging findings were highly consistent with metastatic disease. Given these considerations, her respiratory symptoms were attributed to metastatic involvement, and additional laboratory evaluation was not pursued at that time.
Transvaginal ultrasound confirmed an enlarged uterus with thickened endometrium (0.93 cm). Endometrial biopsy revealed endometrioid adenocarcinoma with squamous differentiation. Molecular profiling demonstrated oestrogen receptor (90%) and progesterone receptor (75%) positivity, MMR proficiency, MSI stability, HER2 negativity, PTEN exon 5 mutation, PIK3R1 positivity, and POLE negativity.
At oncology consultation, her Eastern Cooperative Oncology Group (ECOG) performance status was 2 with a modified Medical Research Council (MMRC) grade 3 dyspnea. Apart from mild post‐biopsy vaginal bleeding, she denied pelvic pain or systemic symptoms. She was staged as cT1N0M1, corresponding to FIGO stage IV‐B endometrial carcinoma.
She began carboplatin–paclitaxel every 3 weeks. After three cycles, CT showed marked regression of pulmonary nodules, near‐resolution of mediastinal adenopathy (Figure 2A), and shrinkage of hepatic lesions (Figure 2B), with resolution of dyspnea. After six cycles, restaging confirmed a very good partial response. She was transitioned to maintenance anastrozole, with subsequent surveillance scans showing stable residual nodules and sustained clinical benefit.
(A) Regression of pulmonary nodules with near‐resolution of mediastinal adenopathy after three cycles of chemotherapy. (B) Near‐complete resolution of the hepatic lesion after chemotherapy.
Discussion
3
This case underscores an unusual presentation of endometrial carcinoma, with cannonball pulmonary metastases as the first clinical manifestation. Endometrial carcinoma is typically confined to the uterus at diagnosis, and postmenopausal bleeding remains the most common presenting symptom. Typical metastatic sites include local pelvic recurrence, pelvic and para‐aortic nodes, peritoneum, and lungs. Only 15%–20% of patients present with extrauterine spread, and fewer than 5% present with distant metastases at initial diagnosis [3]. Pulmonary involvement, when it occurs, is usually seen in recurrent disease rather than at initial presentation. Thus, widespread lung metastases in the form of large, discrete nodules represent an exceptional diagnostic scenario.
“Cannonball lesions” are radiographically defined as multiple, bilateral, well‐circumscribed nodules, often peripheral, ranging from millimetres to several centimetres in size. They generally indicate hematogenous dissemination and are most often linked to renal cell carcinoma or choriocarcinoma [5, 6]. Although infectious or inflammatory disorders such as tuberculosis, fungal infections, echinococcosis, or granulomatosis with polyangiitis may mimic this appearance, the clinical context and ancillary findings usually help differentiate these from metastatic malignancy [7, 8]. In endometrial carcinoma, venous invasion allows tumour emboli to reach the pulmonary vasculature [3]. The reasons some patients develop well‐circumscribed cannonball nodules rather than diffuse micronodular disease remain unclear, but tumour biology, angiogenesis, and host immune factors are likely contributors.
Molecular characterisation provides important therapeutic guidance. Our patient's tumour was ER/PR positive and MMR‐proficient. Hormonal responsiveness supports the use of agents such as anastrozole, while MMR proficiency excludes eligibility for checkpoint inhibitor immunotherapy currently approved in MMR‐deficient disease [9]. Additionally, PTEN and PIK3R1 alterations implicate PI3K/AKT/mTOR signalling, a pathway under investigation for targeted therapies [10].
The backbone of treatment for stage IV endometrial carcinoma remains systemic chemotherapy, most commonly carboplatin and paclitaxel [11]. Hormonal therapy may be considered in ER/PR‐positive disease either as maintenance or when chemotherapy is poorly tolerated [11]. Surgery has limited value in disseminated disease but can provide symptom control in selected patients. Emerging strategies include immunotherapy and targeted agents tailored to molecular subgroups, offering hope for improved outcomes in the future.
In this case, the patient achieved meaningful clinical and radiographic improvement with chemotherapy followed by hormonal maintenance, consistent with literature showing that systemic therapy can provide both palliation and durable disease control even in advanced presentations.
Author Contributions
All the authors contributed to the manuscript. Maneesh Gaddam and Midila Bapineni drafted the initial manuscript. All authors listed critically reviewed, edited the manuscript, and approved the version to be published.
Consent
The authors declare that written informed consent was obtained for the publication of this manuscript and accompanying images and attest that the form used to obtain consent from the patient complies with the Journal requirements as outlined in the author guidelines.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1C. de Haydu , J. D. Black , C. L. Schwab , D. P. English , and A. D. Santin , “An Update on the Current Pharmacotherapy for Endometrial Cancer,” Expert Opinion on Pharmacotherapy 17, no. 4 (2016): 489–499, 10.1517/14656566.2016.1127351.26629895 · doi ↗ · pubmed ↗
- 2R. L. Siegel , K. D. Miller , N. S. Wagle , and A. Jemal , “Cancer Statistics, 2023,” CA: a Cancer Journal for Clinicians 73, no. 1 (2023): 17–48, 10.3322/caac.21763.36633525 · doi ↗ · pubmed ↗
- 3D. Bouros , K. Papadakis , N. Siafakas , and A. F. Fuller , “Natural History of Patients With Pulmonary Metastases From Uterine Cancer,” Cancer 78, no. 3 (1996): 441–447, 10.1002/(SICI)1097-0142(19960801)78:3<>3.0.CO;2-Z.8697389 · doi ↗ · pubmed ↗
- 4I. Otsuka , I. Ono , H. Akamatsu , M. Sunamori , and T. Aso , “Pulmonary Metastasis From Endometrial Carcinoma,” International Journal of Gynecological Cancer 12, no. 2 (2002): 208–213, 10.1046/j.1525-1438.2002.01095.x.11975682 · doi ↗ · pubmed ↗
- 5N. Ammannagari and V. Polu , “Cannon Ball Pulmonary Metastases,” BMJ Case Reports 2013 (2013): bcr 2012008158, 10.1136/bcr-2012-008158.PMC 360438723302554 · doi ↗ · pubmed ↗
- 6R. Agarwal , J. Mukhopadhyay , D. Lahiri , A. Biswas , and P. Maity , “Cannon‐Ball Pulmonary Metastases as a Presenting Feature of Stomach Cancer,” Lung India 32, no. 3 (2015): 300–302, 10.4103/0970-2113.156264.25983428 PMC 4429404 · doi ↗ · pubmed ↗
- 7T. Franquet , N. L. Müller , A. Giménez , P. Guembe , J. de La Torre , and S. Bagué , “Spectrum of Pulmonary Aspergillosis: Histologic, Clinical, and Radiologic Findings,” Radiographics 21, no. 4 (2001): 825–837, 10.1148/radiographics.21.4.g 01jl 03825.11452056 · doi ↗ · pubmed ↗
- 8R. Kshatriya , V. Patel , S. Chaudhari , et al., “Cannon Ball Appearance on Radiology in a Middle‐Aged Diabetic Female,” Lung India 33, no. 5 (2016): 562–568, 10.4103/0970-2113.188988.27625459 PMC 5006345 · doi ↗ · pubmed ↗