Positive Rotational Internal Limiting Membrane Covering Technique for Large Idiopathic Macular Holes
Huiyu Xi, Yingying Song, Yewen Ni, Yumei Cao, Tianyu Zhu, Wei Fan, Haiyang Liu

TL;DR
A new surgical technique using a rotated internal limiting membrane flap successfully closes large macular holes and improves vision.
Contribution
A novel positive rotational internal limiting membrane covering technique for treating large idiopathic macular holes is introduced and evaluated.
Findings
All 13 patients showed successful closure of large idiopathic macular holes.
Visual acuity improved significantly after the procedure.
Postoperative improvements in ellipsoid zone and external limiting membrane defects were observed.
Abstract
This article aims to determine the efficacy of a modified technique by a positive rotational internal limiting membrane (ILM) covering for the treatment of large idiopathic macular holes (IMHs). A prospective analysis was conducted on a cohort of 13 patients with large IMH (> 400 μm). The ILM was dissected in approximately one diameter width of the optic disc from the inferior and temporal sides. Subsequently, a pedicled ILM flap connected to the optic disc was grasped and peeled from the superior edge of the residual ILM with a width of at least 2 papilla diameters (PDs). The pedicled ILM flap was then directly rotated to cover the IMH in a positive way. Some peeled‐off ILM samples were collected for scanning electron microscopy (SEM) examinations. During each follow‐up, best‐corrected visual acuity (BCVA), SD‐OCT scans, and M‐CHARTS were performed. The study successfully detected…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
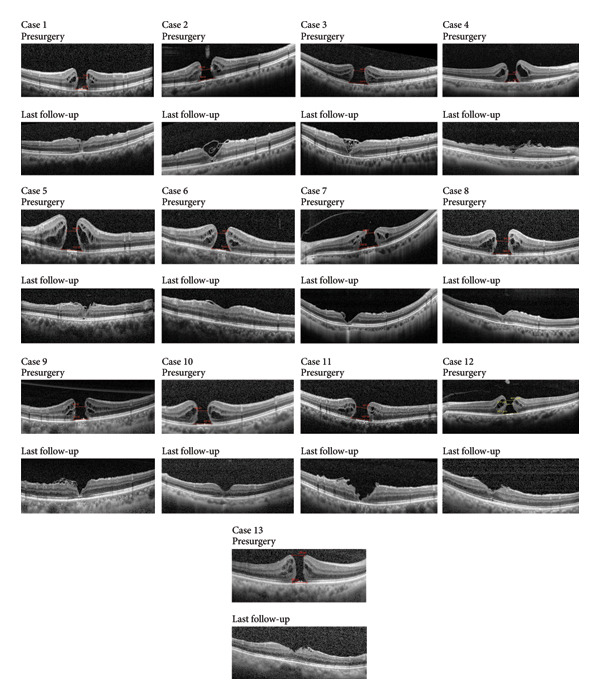 Figure 2
Figure 2| Case no. | Age | Sex | Eye | MLD (μm) | BD (μm) | Intraocular tamponade | Hole closure type | BCVA (logMAR) | Follow‐up, months | Complications | Duration of decreased vision, months | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | |||||||||||
| 1 | 64 | F | Left | 534 | 822 | C3F8 | V | 1.00 | 0.60 | 7 | None | 8 |
| 2 | 68 | F | Right | 588 | 950 | C3F8 | V | 1.00 | 0.70 | 26 | None | 1 |
| 3 | 71 | F | Right | 662 | 1246 | C3F8 | V | 1.30 | 0.52 | 24 | None | 1 |
| 4 | 66 | F | Right | 441 | 897 | C3F8 | U | 1.52 | 0.70 | 32 | None | 24 |
| 5 | 59 | F | Left | 545 | 1131 | C3F8 | U | 1.22 | 0.60 | 29 | None | 3 |
| 6 | 66 | M | Left | 442 | 1034 | C3F8 | U | 1.00 | 0.22 | 26 | None | 6 |
| 7 | 57 | F | Left | 450 | 1299 | C3F8 | V | 1.30 | 0.30 | 24 | None | 8 |
| 8 | 68 | F | Left | 587 | 929 | C3F8 | U | 1.22 | 0.60 | 13 | None | 24 |
| 9 | 60 | F | Left | 617 | 914 | C3F8 | V | 0.82 | 0.60 | 3 | None | 10 |
| 10 | 61 | F | Right | 499 | 937 | C3F8 | U | 1.30 | 0.92 | 15 | None | 2 |
| 11 | 61 | F | Left | 621 | 1057 | C3F8 | V | 1.22 | 0.89 | 15 | None | 1 |
| 12 | 66 | M | Left | 408 | 889 | C3F8 | U | 1.5 | 0.40 | 11 | None | 5 |
| 13 | 67 | F | Right | 425 | 800 | C3F8 | U | 1.0 | 0.52 | 6 | None | 6 |
| Overall | 64.15 ± 4.18 | F(11/13) | Left(8/13) | 524.54 ± 85.96 | 992.69 ± 153.92 | 13 | U/V = 7/6 | 1.18 ± 0.209 | 0.58 ± 0.202 | 17.77 ± 9.567 | 0 | 7.62 ± 7.848 |
| Item | Preoperation | 3 months postoperation |
|
|---|---|---|---|
| Vertical M‐score | 0.45 ± 0.307 | 0.14 ± 0.767 | 0.001 |
| Horizontal M‐score | 0.58 ± 0.358 | 0.20 ± 0.147 | < 0.001 |
| BCVA (logMAR) | 1.18 ± 0.209 | 0.58 ± 0.202 | < 0.001 |
| mf‐ERG R1 (8 cases) | 78.29 ± 32.697 | 94.88 ± 37.374 | 0.161 |
| Time point | ELM | EZ |
|---|---|---|
| Preoperation | 1031.00 ± 224.49 | 1381.69 ± 270.31 |
| 1 month postoperation | 386.54 ± 265.58 | 632.46 ± 264.69 |
|
| < 0.001 | < 0.001 |
| 3 months postoperation | 214.08 ± 266.05 | 371.38 ± 285.97 |
|
| < 0.001∗; 0.002∗∗ | < 0.001∗;< 0.001∗∗ |
- —Xuzhou Medical Key Talents Project
- —Xuzhou Key R & D Program
- —Natural Science Foundation of Jiangsu Province10.13039/501100004608
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRetinal and Macular Surgery · Intraocular Surgery and Lenses · Corneal Surgery and Treatments
1. Introduction
Pars plana vitrectomy (PPV) combined with internal limiting membrane (ILM) peeling and gas tamponade was first introduced as a treatment for MHs by Kelly and Wendel in 1991 [1]. It has been widely accepted as the standard surgery for idiopathic macular holes (IMHs) due to the high closure rate, especially for those with a size less than 400 μm. However, for IMHs larger than 400 μm, the closure rate is lower. The application of the ILM covering technique can improve the closure rate and lead to a better functional prognosis for large IMHs. Studies have demonstrated that the ILM flap can act as a scaffold for the proliferation of glial cells along with remaining Müller cells [2]. The inverted ILM flap technique, first reported by Michalewska, is one of the most widely studied surgical procedures [3]. However, it has been reported that the inverted ILM flap technique may not effectively contribute to the reconstruction of the outer retinal layers and vision restoration in cases of large IMH [4], as it provides a smooth surface for the IMH covering and results in fewer Müller cells [5]. Therefore, a modified technique involving a positive pedicled ILM flap that is created and rotated directly to cover the IMH, followed by the use of autologous blood clot (ABC) to fasten the flap, may be beneficial for reconstructing the microstructure of large IMHs and improving visual outcomes.
2. Methods
A prospective and consecutive study was conducted at Xuzhou First People’s Hospital from May 2022 to August 2023. Twelve patients with large IMHs (> 400 μm) underwent vitrectomy using a new technique. Presurgery, we recorded the best‐corrected visual acuity (BCVA) and basic eye conditions. Spectral domain optical coherence tomography (SD‐OCT) was used to verify and measure the IMHs. Metamorphopsia changes were evaluated using M‐CHARTS before and after surgery, specifically using the two‐line type due to central scotoma in IMHs. Detailed examinations, including BCVA, intraocular pressure (IOP), M‐CHART, slit‐lamp examination, fundus examination, and foveal microstructure using SD‐OCT, were conducted before and after surgery. Additionally, eight patients underwent multifocal electroretinogram (mf‐ERG). Patients with highly myopic and other ocular disorders, except mild‐to‐moderate cataracts, were excluded. The study adhered to the principles of the Declaration of Helsinki and was approved by the Ethics Committee of Xuzhou First People’s Hospital. The surgical procedure, detailed in a supporting video (see video [here] and Figure 1), involved a standard 23‐G PPV (Alcon, Constellation) under retrobulbar anesthesia by a single experienced surgeon (H.L.). All patients had cataracts and underwent phacoemulsification with intraocular lens implantation. The posterior vitreous was visualized with triamcinolone and removed with core vitrectomy. Indocyanine green (ICG, 1.25 mg/mL, Eisai, Inc., Shenyang, China) was injected into the vitreous cavity to stain the ILM around the IMH, which was then peeled off from the inferior and temporal sides in a long strip shape approximately one diameter width of the optic disc, ensuring complete removal of the ILM at the edge of the IMH. To prepare for future scanning electron microscopy (SEM) examinations, the peeled‐off ILMs were harvested and placed into 4% formaldehyde and then stored at 4°C overnight for fixation. Considering the gravity, we grasped and peeled a flap from the superior and the temporal edge of residual ILM near the vascular arch, with an area of at least 2 papilla diameters (PDs). The pedicled ILM flap was attached to the optic disc and rotated to cover the IMH directly in a positive way. ABC was obtained from the patient’s elbow vein using a 2‐mL syringe, and then, it was immediately applied to fasten the ILM flap, followed by the gas–fluid exchange. Finally, the vitreous cavity was filled with 10% C3F8 as tamponade. All patients were required to keep a prone position for 7–14 days [6].
Figure 1. Main process diagram. (a) The stained internal limiting membrane around the idiopathic macular hole was approximately peeled off. (b) Grasped and peeled a flap from the superior and the temporal edge of residual internal limiting membrane near the vascular arch, with an area of at least 2PD. (c) The internal limiting membrane flap is pedicled which attached to the macular hole. (d) Autologous blood clot was applied to fasten the internal limiting membrane flap, followed by the gas–fluid exchange.(a)(b)(c)(d)
Referring to the protocol of SEM, the fixation of the membranes was done for a duration of 2 h using 2% glutaraldehyde in a buffer solution containing 0.1 M sodium cacodylate. Subsequently, the specimens underwent dehydration through a series of ascending ethanol solutions for 2 h. Preservation of the terminal structure was achieved by critical point drying with carbon dioxide (CPD 30, BAL‐TEC AG, Balzers, Liechtenstein) and followed by gold sputtering (SCD 005, BAL‐TEC AG). Finally, examination of the membranes was conducted using a LEO 1450 VP SEM (Carl Zeiss AG, Oberkochen, Germany).
Statistical analysis was conducted using SPSS software (Version 26.0, IBM SPSS Statistics). Normality of the data was tested using the Shapiro–Wilk test. To compare the data before and after the operation, the paired sample t‐test was utilized for analyzing the difference, assuming normal distribution of the data. In cases where the data did not follow a normal distribution, the paired Wilcoxon signed‐rank test was employed for comparison.
3. Results
All patients began the postsurgery follow‐up at 1 month, which lasted for a minimum of 3 months. The status of IMH closure or remaining open was confirmed using SD‐OCT images obtained at the final follow‐up. Restoration of foveal closure after IMH closure was categorized into U‐shape, V‐shape, W‐shape, and flap‐closure outcomes. The positive ILM rotational covering technique was successfully performed on 13 patients, resulting in IMH closure in all cases (100%) after a single procedure. Additionally, all patients experienced a significant improvement in BCVA compared to their preoperative vision. The mean IMH diameter and base aperture were 524.54 ± 85.96 μm and 992.69 ± 153.92 μm, respectively, as detailed in Table 1. At the last postoperative follow‐up, we discovered 7 eyes with U‐shape closure and 6 eyes with V‐shape closure. The flap closure was not observed in this study. All cases of IMH closure are illustrated in Figure 2.
The preoperative and last follow‐up SD‐OCT images of 13 cases. All cases obtain macular hole closure.
The mean BCVA (logMAR) before surgery was 1.18 ± 0.209 and after surgery was 0.58 ± 0.202, showing a statistically significant difference (p < 0.001). The average follow‐up period was 17.77 ± 9.567 months. Macular foveal images were obtained using OCT 1 month after the operation due to C3F8 absorption. The horizontal and vertical deformations after operation were significantly improved compared with those before operation (p = 0.001, p < 0.001). The result of ERG analysis revealed that the response density in the postoperative period was improved, but the difference was not statistically significant (Table 2). The diameter of the defect of external limiting membrane (ELM) and ellipsoid zone (EZ) was significantly smaller at the 1‐month postoperative observation time (p < 0.001). And the defect size decreased further at the 3‐month follow‐up compared to the 1‐month follow‐up (ELM: p = 0.002; EZ: p < 0.001) (Table 3). No surgery‐related complications were reported during the follow‐up period.
Surface examinations using SEM revealed smooth vitreal surfaces and rough retinal surfaces with the residual Müller cell debris, as illustrated in Figure 3.
Figure 3. The vitreum (a) and retinal (b) surface of the internal limiting membrane in scanning electron microscopy.(a)(b)
4. Discussion
IMH is a well‐known retinal disease classified by Gass in 1995 [7]. PPV combined with ILM peeling and gas tamponade, initially proposed by Kelly, has now emerged as the standard technique for treating IMHs [1]. Nonetheless, when dealing with large or recurrent MHs, the efficacy of the ILM peeling approach can be limited. This may be attributed to the fact that ILM peeling only focuses on the anteroposterior traction toward the fovea and the tangential tension of the ILM, without fully stimulating gliosis in the macular hole area.
Therefore, the ILM flap covering technique, introduced by Michalewska, utilizes the ILM flap as a scaffold for cell proliferation to aid in IMH recovery [3]. Numerous studies have shown that this technique can improve closure rates, particularly in cases of large IMHs (> 400 μm) [8–10]. Since then, various improvements have been made in the ILM flap covering technique, all of which have shown positive outcomes [11–14]. Additionally, alternative approaches such as ILM insertion, amniotic membrane transplantation, lens capsule transplantation, and neural retinal transplantation have been explored for treating large IMHs, but these methods have shown lower therapeutic effectiveness when compared to the ILM flap covering technique [15–18]. Along with the further research about the histopathological characteristics of ILM through an electron microscope, we could observe the difference between the vitreal side and retinal side. The vitreal side is smooth, whereas the retinal side is undulated, and the residual Müller cell debris could be detected on the retinal side. This result is consistent with the results of previous studies [19, 20].
Thus, the cover of the ILM retinal side over the IMH would theoretically supply a better structure for IMH closure. Besides, in our previous study [14], the inverted ILM flap technique resulted in only one “U‐shape” IMH closure out of 13 cases, whereas this new positive ILM flap technique led to “U‐shape” closures in more cases (7 out of 13). The successful repair of IMHs can be classified by OCT into two types: closure without neurosensory retinal defect and closure with neurosensory retinal defect (W‐shape). Based on the contour of the macular fovea on OCT, closure without neurosensory retinal defect can also be categorized as normal foveal contour (U‐shape) and step foveal contour (V‐shape). Postoperative visual acuity was best with U‐shape closure, and W‐shape closure was associated with the worst visual outcomes [21, 22].
Several previous articles have discussed the use of the positive ILM flap technique for treating IMHs, all demonstrating high rates of IMH closure and improved visual acuity. Tian proposed a surgical approach involving ILM peeling and in situ covering around the IMH to maintain retinal integrity [23]. However, this method may not be suitable for patients with IMHs larger than 400 μm. In contrast, Hu developed a new technique involving a pedicled ILM flap for IMHs in a positive way, which was flattened using PFCL [24]. This method may present challenges with the PFCL residue. Additionally, silicon oil was applied in some cases to prevent displacement of ILM, which required a second operation to remove the silicon oil. Our procedure differs from Hu’s in that we select the optic disc as the anchor point for the ILM flap. This technique effectively alleviates the tension on the temporal ILM of the IMH, which is a key factor in IMH formation [25].
Therefore, a modified method we invented is to rotate the pedicled ILM flap in a positive way from the upper vascular arch to cover the IMH following the complete ILM peeling around the IMH. The procedure involved peeling the ILM around the IMH from the inferior and temporal sides in a long strip shape approximately one diameter width of the optic disc. Subsequently, a 2‐PD‐wide ILM flap attached to the optic disc was directly rotated to cover the IMH. ABC was used to facilitate the flap adherence and 10% C3F8 was injected to fill the eye. This technique allowed for the release of tractive forces and ensured the creation of a sufficiently large ILM flap to cover the IMH, regardless of the condition of the ILM in the macular. As a result, all patients achieved closure of their IMHs and experienced a significant improvement in BCVA. According to the images of OCT in the last follow‐up, all patients presented U‐ or V‐shape, with no W‐shape detected. It is a better result compared to our previous study about inverted flap technique [14]. In our study, we observed a significant reduction in the extent of damage to the ELM and EZ of patients at 1 and 3 months postsurgery compared to presurgery. And the defect size decreased further at the 3‐month follow‐up compared to the 1‐month follow‐up. Interestingly, the degree of restoration of EZ was found to be lower than that of ELM, and patients with an intact EZ at the final follow‐up also maintained an intact ELM layer. This indicates that ELM may be the initial structure to recover following surgery for IMHs, which aligns with prior research findings [26]. The use of two‐line type M‐CHARTS effectively quantified metamorphopsia in patients with IMHs pre‐ and postsurgery [27, 28]. Specifically, our analysis using M‐CHARTS revealed a significant improvement in visual distortion in both vertical and horizontal directions at 3 months after surgery. There was an increasing trend of mf‐ERG, but it was not statistically significant, which may be due to the small number of cases.
The results of visual acuity recovery in our study were compared with previous research on the ILM flap technique. Compared to the visual acuity recovery associated with the inverted flap technique in our prior study [14], we observed a notable degree of improvement with this method. Additionally, there was an enhancement over the other positive methods [25]. However, when compared to Tian’s study [29], our improvement in visual acuity did not reach the same level. This discrepancy may be attributed to the smaller MH diameter reported in Tian’s cases (367.0 ± 120.7 μm) compared to our findings (minimum linear diameter: 524.54 ± 85.96 μm). Additionally, the baseline vision of participants in Tian’s study was superior to that of our participants.
Nevertheless, while our study identified a greater number of U‐shaped closures, we cannot definitively conclude that this technique surpasses the previous inverted flap method. A randomized controlled trial will be beneficial for verifying this hypothesis. Furthermore, additional mf‐ERG results are still needed to demonstrate the changes in retinal sensitivity of the macula following surgery.
In conclusion, the ILM rotational covering surgery with positive flap could provide sufficient ILM flap to cover the IMH in a physiological way. This approach proves to be a valuable treatment for larger IMHs (> 400 μm). The results of this study suggested that this technique may be helpful for anatomical and functional recovery. However, further studies with larger sample sizes and longer follow‐ups are required to confirm the efficacy of this approach. Prospective randomized controlled trials are also crucial to establish the superiority of the positive ILM flap technique.
NomenclatureIMHIdiopathic macular holePDPapilla diameterSEMScanning electron microscopyBCVABest‐corrected visual acuityEZEllipsoid zoneELMExternal limiting membraneILMInternal limiting membraneERMEpiretinal membraneSD‐OCTSpectral domain optical coherence tomographyIOPIntraocular pressureERGMultifocal electroretinogramPPVPars plana vitrectomy
Ethics Statement
This study was approved by the Institutional Review Board of Xuzhou First People’s Hospital (Ethical approval number: xyyll[2021]‐XJSFX‐058). All methods were conducted in accordance with the tenets of the Declaration of Helsinki.
Consent
All data were obtained with written informed consent from participants for participation in the study.
Written informed consent was obtained from all study participants.
Disclosure
The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. All authors read and approved the final manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
Author Contributions
Haiyang Liu generalized the idea of the new technique, performed the surgery, and revised the manuscript. Huiyu Xi drafted the manuscript and interpreted the results. Yingying Song and Yewen Ni analyzed the patient data and performed the SEM examinations. Yumei Cao and Tianyu Zhu performed the OCT, mf‐ERG and M‐CHART examinations. Wei Fan edited the photos. Huiyu Xi, Yingying Song, and Yewen Ni contributed equally to this work and should be considered co‐first authors.
Funding
This study was supported by Xuzhou Medical Key Talents Project (no. XWRCHT20220048), Xuzhou Key R & D Program (no. KC22099), and Natural Science Foundation of Jiangsu Province (BK20241765).
Supporting Information
The video depicts the surgical procedure: firstly, the stained internal limiting membrane around the idiopathic macular hole was approximately peeled off. Secondly, a flap from superior and temporal edges of the residual internal limiting membrane near the vascular arch was grasped and peeled, with an area ≥ 2 PD. Subsequently, the internal limiting membrane flap is pedicled which attached to the macular hole. Finally, autologous blood clot was applied to fasten the internal limiting membrane flap, followed by the gas–fluid exchange.
Supporting information
Supporting Information Additional supporting information can be found online in the Supporting Information section.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kelly N. E. and Wendel R. T. , Vitreous Surgery for Idiopathic Macular Holes: Results of a Pilot Study, Archives of Ophthalmology. (1991) 109, no. 5, 654–659, 10.1001/archopht.1991.01080050068031, 2-s 2.0-0025828271.2025167 · doi ↗ · pubmed ↗
- 2Ittarat M. , Somkijrungroj T. , Chansangpetch S. , and Pongsachareonnont P. , Literature Review of Surgical Treatment in Idiopathic Full-Thickness Macular Hole, Clinical Ophthalmology. (2020) 14, 2171–2183, 10.2147/OPTH.S 262877.32801628 PMC 7398756 · doi ↗ · pubmed ↗
- 3Michalewska Z. , Michalewski J. , Dulczewska-Cichecka K. , and Nawrocki J. , Inverted Internal Limiting Membrane Flap Technique for Surgical Repair of Myopic Macular Holes, Retina. (2014) 34, no. 4, 664–669, 10.1097/IAE.0000000000000042, 2-s 2.0-84897573105.24263468 · doi ↗ · pubmed ↗
- 4Faria M. Y. , Proença H. , Ferreira N. G. , Sousa D. C. , Neto E. , and Marques-Neves C. , Inverted Internal Limiting Membrane Flap Techniques and Outer Retinal Layer Structures, Retina. (2020) 40, no. 7, 1299–1305, 10.1097/IAE.0000000000002607.31259810 · doi ↗ · pubmed ↗
- 5Hirata A. , Murata K. , Hayashi K. , and Nakamura K. I. , Three-Dimensional Analysis of Peeled Internal Limiting Membrane Using Focused Ion Beam/Scanning Electron Microscopy, Translational Vision Science & Technology. (2018) 7, no. 1, 10.1167/tvst.7.1.15, 2-s 2.0-85041843572.PMC 580232829423341 · doi ↗ · pubmed ↗
- 6Thompson J. T. , The Absorption of Mixtures of Air and Perfluoropropane After Pars Plana Vitrectomy, Archives of Ophthalmology. (1992) 110, no. 11, 1594–1597, 10.1001/archopht.1992.01080230094028, 2-s 2.0-0026442906.1444918 · doi ↗ · pubmed ↗
- 7Gass J. D. , Reappraisal of Biomicroscopic Classification of Stages of Development of a Macular Hole, American Journal of Ophthalmology. (1995) 119, no. 6, 752–759, 10.1016/s 0002-9394(14)72781-3, 2-s 2.0-0029059254.7785690 · doi ↗ · pubmed ↗
- 8Bonińska K. , Nawrocki J. , and Michalewska Z. , Mechanism of Flap Closure After the Inverted INTERNAL Limiting Membrane Flap Technique, Retina. (2018) 38, no. 11, 2184–2189, 10.1097/IAE.0000000000001861, 2-s 2.0-85055659739.28961670 · doi ↗ · pubmed ↗