Distribution and Clinical Characteristics of MIH in Schoolchildren From the Central Peruvian Jungle: A Cross‑Sectional Study
Mayra Belen Barahona-Hernandez, Roxana Patricia López-Ramos, Julio César Sánchez-Sotomayor, Karin Harumi Uchima-Koecklin, Daniel José Blanco-Victorio, Gilmer Torres-Ramos

TL;DR
This study found that 18.8% of schoolchildren in Peru's Central Jungle region have a tooth enamel defect called MIH, mainly affecting molars and showing specific patterns and severity.
Contribution
The study provides new data on MIH prevalence and clinical characteristics in a previously understudied jungle region of Peru.
Findings
MIH prevalence was 18.8% in 6–12-year-old children from the Central Jungle region of Peru.
First permanent molars were more affected than incisors, with molars showing greater severity and higher rates of post-eruptive breakdown.
Pattern I was most common (78.7%), while patterns II/III showed male predominance and more severe lesions.
Abstract
Molar incisor hypomineralisation (MIH) is a developmental enamel defect that predominantly affects first permanent molars and frequently involves incisors. However, evidence on MIH prevalence and clinical presentation in jungle regions is limited. To determine the distribution and clinical patterns of MIH among schoolchildren in the Central Jungle region of Peru. This cross‐sectional study included 1500 schoolchildren aged 6–12 years from two public schools in Peru’s Central Jungle region, recruited through stratified random sampling. Two calibrated examiners diagnosed MIH using European Academy of Paediatric Dentistry (EAPD) criteria (inter‐examiner κ = [0.87]; intra‐examiner κ = [0.89]). Categorical variables were analysed using Pearson’s chi‐squared and Fisher’s exact tests (α = 0.05, 95% CI). MIH prevalence was 18.8% (95% CI: [17.0–20.0]). First permanent molars were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
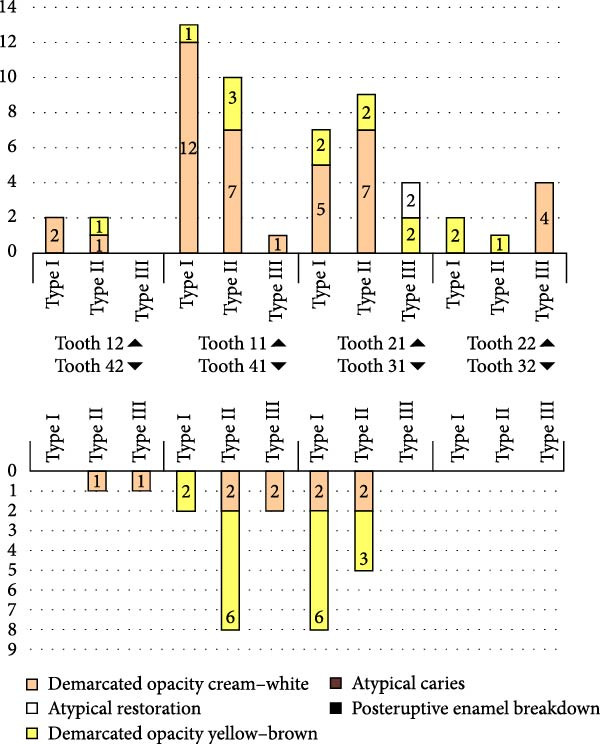 Figure 1
Figure 1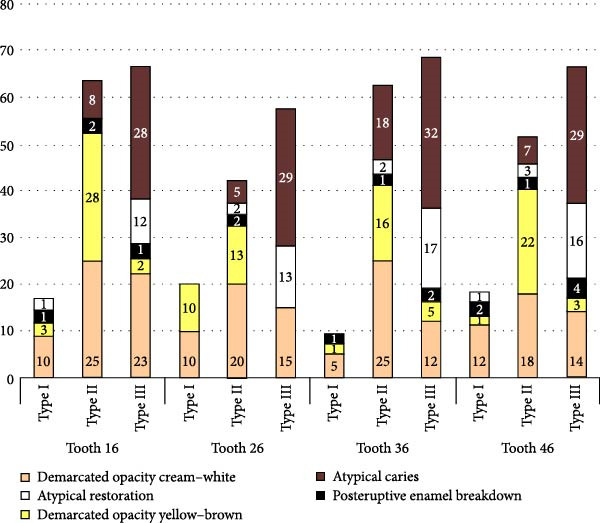 Figure 2
Figure 2| Category | Definition |
|---|---|
| Distribution pattern [ | |
| Pattern I | Molars only |
| Pattern II | Molars and ≥1 affected incisor |
| Pattern III | Upper and lower molars and incisors affected |
| Clinical status [ | |
| Demarcated opacity | White–cream or yellow–brown demarcated opacity |
| Post‐eruptive breakdown | Loss of enamel structure after tooth eruption |
| Atypical restoration | Restoration not consistent with caries pattern |
| Atypical caries | Caries in unusual locations associated with MIH |
| Extraction due to MIH | Tooth extracted because of MIH severity |
| Not categorized | Unable to classify due to insufficient information |
| Lesion extension [ | |
| Type I | <1/3 of tooth surface affected |
| Type II | ≥1/3 but <2/3 of tooth surface affected |
| Type III | ≥2/3 of tooth surface affected |
| Oral condition |
| CI (95%) |
|---|---|---|
| Without MIH | 1218 (81.2) | |
| MIH | 282 (18.8) | 17.0%–20.0% |
| Total | 1500 (100.0) |
| Teeth affected by MIH | Upper arch |
| Lower arch |
| ||||
|---|---|---|---|---|---|---|---|---|
|
Right hermiarcade
|
Left hermiarcade
|
Total
|
Right hermiarcade
|
Left hermiarcade
|
Total
| |||
| Central incisor | 24 (7.1) | 20 (5.9) | 44 (13.1) | 0.016 ∗ | 12 (3.8) | 13 (4.2) | 25 (7.9) | 1.000 ∗ |
| Lateral incisor | 0 (0.0) | 7 (2.1) | 7 (2.1) | 2 (0.6) | 2 (0.6) | 4 (1.3) | ||
| First molar | 152 (45.3) | 133 (39.6) | 285 (84.8) | 143 (45.1) | 145 (45.7) | 288 (90.9) | ||
|
Total
| 176 (52.4) | 160 (47.6) | 336 (100.0) | 157 (49.5) | 160 (50.5) | 317 (100.0%) | ||
| Proportion | 0.198 | 0.187 | 0.200 ∗∗ | |||||
| Sex | Pattern |
| ||
|---|---|---|---|---|
| Pattern I | Pattern II/Pattern III | Total | ||
| Male | 105 (37.2) | 40 (14.2) | 145 (51.4) | 0.008 |
| Female | 117 (41.5) | 20 (7.1) | 137 (48.5) | |
|
Total
| 222 (78.7) | 60 (21.3) | 282 (100.0%) | |
| Teeth affected by MIH | Incisors | Molars |
|
|---|---|---|---|
| Clinical status |
|
| |
| Demarcated white–cream opacity | 49 (7.4) | 188 (28.5) | 0.001 ∗ |
| Demarcated yellow–brown opacity | 28 (4.3) | 108 (16.9) | |
| Loss of structure | 4 (0.6) | 16 (2.4) | |
| Atypical restoration | 2 (0.3) | 66 (10.0) | |
| Atypical caries | 0 (0.0) | 159 (24.1) | |
| Extracted due to MIH | 0 (0.0) | 10 (1.5) | |
| Not categorised | 0 (0.0) | 29 (4.4) | |
| Total | 83 (12.6) | 576 (87.4) |
| Affected teeth | Upper molars | Lower molars | Upper incisors | Lower incisors | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Extension |
| % |
| % |
|
| % |
| % |
| |
| Type I | 35 | 12.3 | 24 | 8.8 | 0.001 | 24 | 43.6 | 12 | 41.4 | 0.645 | |
| Type II | 117 | 41.1 | 120 | 41.7 | 20 | 39.2 | 15 | 51.7 | |||
| Type III | 133 | 46.7 | 144 | 49.5 | 7 | 12.8 | 2 | 6.9 | |||
| Total | 285 | 100.0 | 288 | 100.0 | 51 | 100.0 | 29 | 100.0 | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone and Dental Protein Studies · dental development and anomalies · Forensic Anthropology and Bioarchaeology Studies
1. Introduction
Molar‐incisor hypomineralisation (MIH), introduced by Weerheijm in 2001 [1], describes a systemic condition involving asymmetrical involvement of one or more permanent first molars, with or without affected incisors [1, 2]. Clinical manifestations range from distinct white–yellow or yellow–brown opacities to severe hypomineralised enamel prone to post‐eruptive breakdown [3, 4]. Affected teeth exhibit hypersensitivity to thermal and mechanical stimuli, impairing masticatory function and oral hygiene compliance, thereby elevating caries risk [5–9]. Incisor involvement additionally imposes aesthetic and psychosocial burdens [10].
MIH aetiology remains multifactorial, encompassing pharmacological exposures (antibiotics, anticonvulsants), childhood illnesses, perinatal hypoxia, and hypomineralised second primary molars [4, 11, 12]. Genetic predisposition and epigenetic mechanisms may further contribute to pathogenesis [13, 14]. Global MIH prevalence is estimated at 15.5%, with regional variation: North America 23.9%, Europe 14.3%–14.4%, Africa 10.9%–14.5% and South America 17.1% [15]. In Peru, most research concentrates on coastal and Andean populations (Lima 10% [16]; Puno 19.8% [17]), leaving jungle regions—which differ substantially in environmental exposures, healthcare access, and sociodemographic characteristics [18]—understudied despite representing considerable national territory.
This study aimed to determine MIH distribution and clinical patterns among schoolchildren aged 6–12 years in Peru’s Central Jungle using European Academy of Paediatric Dentistry (EAPD) criteria [1], thereby informing targeted public health interventions (school‐based screening, preventive strategies and capacity‐building for primary‐care teams) in underserved communities.
2. Materials and Methods
2.1. Ethics Approval and Study Design
This cross‐sectional study received approval from the Institutional Research Ethics Committee of Peru (Registration number: CIEI‐2020‐19). Written informed consent was obtained from parents or caregivers, and assent was secured from all participating children prior to enrollment.
2.2. Study Setting
The study was conducted in Pichanaqui district, Central Jungle of Junín Region, Peru—a predominantly agricultural area with over 39,000 inhabitants characterised by coffee production and a mix of urban and rural zones [18]. This location was selected for its representativeness of underserved rural communities in highland‐lowland transition zones, where limited access to specialised paediatric dental care and environmental factors (variable water quality, nutritional challenges) may influence the prevalence of developmental enamel defects like MIH [17].
2.3. Sampling Strategy and Sample Size
Two public schools were randomly selected from the complete roster of six public institutions in the Pichanaqui district using random number generation in Microsoft Excel 2019 (Microsoft Corporation, Redmond, WA, USA). Within these schools, participants were recruited via simple random sampling from enrollment lists.
Sample size was calculated using Epidat software version 4.2 (Dirección Xeral de Saúde Pública, Xunta de Galicia, 2016) based on an anticipated MIH prevalence of 19.8% [17], 2.5% precision, 80% statistical power, and 95% confidence level. Accounting for a 20% non‐response rate, the minimum required sample was 977 participants; this was inflated to 1500 to enhance precision and generalizability.
2.4. Selection Criteria
Inclusion criteria: children aged 6–12 years [19, 20] in mixed dentition phase with all four first permanent molars and permanent incisors erupted to at least one‐third of crown height [21].
Exclusion criteria: children with severe systemic illnesses, incomplete records, teeth with extensive restorations obscuring enamel surfaces or confounding enamel conditions (amelogenesis imperfecta, severe dental fluorosis or hypoplasia unrelated to MIH) [22–24].
2.5. Examiner Training and Calibration
Two paediatric dentistry examiners underwent structured training provided by a senior paediatric dentist with over 20 years of experience (originally trained in Brazil). Training comprised two sessions: (1) practical instruction using standardised images illustrating the spectrum of MIH presentations and other developmental enamel defects; (2) independent assessment of 30 digital images classified according to EAPD criteria.
Reliability was assessed using Cohen’s kappa coefficient: inter‐examiner agreement κ = 0.87; intra‐examiner reliability (reassessed after a 10‐day interval to minimise recall bias) κ = 0.89—both indicating substantial agreement. Disagreements during calibration were resolved through consensus discussion with the senior trainer. Examiners remained blinded to participants’ demographic and socioeconomic data throughout assessments.
2.6. Clinical Examination
Examinations were conducted in school dental offices equipped with dental units and LED lighting. All participants received prophylaxis prior to evaluation. Teeth were assessed in a wet state using an oral mirror and periodontal probe, following EAPD guidelines [1].
2.7. Diagnostic Criteria
MIH was diagnosed according to EAPD criteria [1] (Table 1).
2.8. Statistical Analysis
Data was recorded in Microsoft Excel 2019 and analysed using Stata version 16.0 (StataCorp LLC, College Station, TX, USA). Qualitative variables were described using absolute and relative frequencies. Normality assumptions were assessed prior to analysis.
Inferential comparisons employed chi‐squared tests for categorical variables and Fisher’s exact test when expected cell counts were <5. The difference of proportions test compared to the overall proportions of affected teeth between right and left hemiarcades based on total counts per arch. All tests were two‐tailed with significance set at p < 0.05; 95% confidence intervals are reported. Participants with missing data were excluded from analysis.
3. Results
The prevalence of MIH among schoolchildren was 18.8% (95% CI: 17.0%–20.0%). This narrow confidence interval indicates a precise estimate of MIH prevalence in this population (Table 2).
3.1. MIH Distribution
Table 3 shows that MIH predominantly affects the first permanent molars. In the upper arch, 285 of the 336 affected teeth were first molars (84.8%), and in the lower arch, 288 of the 317 affected teeth were first molars (90.9%, Table 3). Incisor involvement was considerably less common: central incisors accounted for 44/336 (13.1%) of affected teeth in the upper arch and 25/317 (7.9%) in the lower arch, whereas lateral incisors were uncommon (upper 7/336, 2.1%; lower 4/317, 1.3%). The distribution between the right and left hemi‑arcades was broadly symmetrical. In the upper arch, 176/336 (52.4%) affected teeth were on the right, 160/336 (47.6%) were on the left (no difference in proportions, p = 0.198), and in the lower arch, 157/317 (49.5%) were on the right, and 160/317 (50.5%) were on the left (no difference in proportions, p = 0.187). The overall comparison between the right and left hemi‑arcades was not statistically significant (p = 0.200). The only statistically significant lateral asymmetry observed was for upper lateral incisors: all seven affected upper lateral incisors were on the left side (p = 0.016). No significant difference was found for the lower lateral incisors (p = 1.000).
3.2. MIH Pattern
Overall, Pattern I predominated, affecting 222 of 282 children (78.7%), whereas Pattern II/III were present in 60 children (21.3%). By sex, 105/145 males (72.4%) and 117/137 females (85.4%) exhibited Pattern I. Conversely, patterns II/III occurred in 40/145 males (27.6%) compared with 20/137 females (14.6%). The association between sex and the MIH pattern distribution was statistically significant (p = 0.008). Specifically, males were more likely than females to exhibit patterns II/III, with 40 males (14.2%) compared to 20 females (7.1%) affected, as detailed in Table 4.
3.3. Clinical Characteristics
The clinical pattern of MIH differed significantly between incisors and molars (p = 0.001). Although demarcated opacities were common in both groups, molars more frequently presented white–cream (188/576; 28.5%) and yellow–brown opacities (108/576; 16.9%) and were disproportionately affected by more severe outcomes: loss of structure (16/576; 2.4%), atypical restorations (66/576; 10.0%), atypical caries (159/576; 24.1%) and extractions attributed to MIH (10/576; 1.5%). In contrast, incisors presented mainly as demarcated opacities (49/83 white–cream, 28/83 yellow–brown), with very few restorations or carious lesions recorded. (Table 5).
3.4. Extension of Lesions
The extent of MIH differed by tooth type: molars most frequently presented with extensive lesions (Type III: upper 133/285, 46.7%; lower 144/288, 49.5%) and showed a significantly different distribution between arches (p = 0.001), whereas incisors predominantly presented less extensive defects (Type I) with no significant arch‑related difference (p = 0.645) (Table 6).
3.5. Distribution of Lesion Extent and Clinical Features of MIH by Tooth (Incisors and First Molars)
Figure 1 illustrates the distribution of lesion extent (Types I–III) and clinical features of MIH across incisor types. Upper central incisors (teeth 11 and 21) showed the highest frequency of involvement, mainly with Type I and II defects. Demarcated opacities, particularly cream–white, were the predominant clinical feature, whereas post‑eruptive enamel breakdown, atypical restorations and atypical caries were rare. Consistent with Table 6, no statistically significant difference in lesion extent was observed between upper and lower incisors (χ ^2^(2) = 0.89, p = 0.645).
Distribution of lesion extent (Types I–III) and clinical features of MIH by incisor type. No significant difference in lesion extent was observed between upper and lower incisors (χ²(2) = 0.89, p = 0.645).
Figure 2 shows the distribution of lesion extent and clinical characteristics in upper (teeth 16 and 26) and lower (teeth 36 and 46) first permanent molars. Demarcated opacities (cream–white and yellow–brown) were frequent in all molars but were especially common in Type II and Type III lesions. Post‑eruptive enamel breakdown and atypical caries concentrated in the most severely affected teeth, particularly teeth 26, 36 and 46, whereas atypical restorations were less frequent. In agreement with Table 6, the extent of MIH differed significantly between upper and lower molars (χ ^2^(2) = 14.46, p = 0.001), with lower molars showing a higher proportion of extensive defects (Type III).
Distribution of lesion extent (Types I–III) and clinical features of MIH in upper and lower first permanent molars. Lesion extent differed significantly between upper and lower molars, with more extensive defects (Type III) in the lower arch (χ²(2) = 14.46, p = 0.001).
4. Discussion
This cross‐sectional study established an 18.8% MIH prevalence among children aged 6–12 years in Central Jungle, Peru—consistent with global estimates (one in six to seven children affected) [15, 26–28] and Latin American reports from Peru (15.9%–20.2%) [16, 17]. Notable sex‐related differences emerged: patterns II/III predominated in males, whereas pattern I was more common in females. These findings contrast with studies reporting no sex predilection [22, 29, 30], but align with research linking MIH severity variations to biological variability or differential environmental exposures during amelogenesis [11, 12]. First permanent molars were predominantly affected, exhibiting extensive lesions, post‐eruptive breakdown, atypical caries and restorations, while incisors presented primarily mild demarcated opacities. A symmetrical distribution across hemiarcades was observed, except for upper lateral incisors (p = 0.016), though absolute numbers remained small. These patterns reflect MIH’s heterogeneous nature across tooth types [31, 32], likely influenced by multifactorial genetic and systemic aetiologies [12, 14].
The observed molar involvement (84.8% upper; 90.9% lower) aligns with established literature documenting preferential first molar affectation [1, 22, 33]. Molars predominantly exhibited moderate‐to‐severe defects (Types II/III) characterised by yellow–brown opacities, enamel breakdown, and atypical restorations, whereas incisors displayed mainly Type I lesions (cream‐white opacities) [3, 34]. The high proportion of atypical caries in hypomineralised molars corroborates evidence that defective enamel facilitates rapid breakdown, increased plaque accumulation and dentine exposure [5, 28, 35], complicating restorative management and heightening extraction risk [36]. Hypersensitivity may further reduce oral hygiene tolerance, compounding caries development [6, 8].
MIH represents a significant public health concern in the region, given its association with increased caries susceptibility, hypersensitivity and diminished quality of life [8–10, 31]. The study’s focus on Pichanaqui—a district representing underserved Amazonian communities with limited specialised dental care and potential environmental risk factors (variable water quality and nutritional challenges)—addresses critical gaps in understanding MIH prevalence in ecologically and socioeconomically diverse highland‐lowland transition zones [18]. Early diagnosis is imperative: adoption of standardised diagnostic criteria (e.g., EAPD guidelines) and comprehensive training protocols enhances reporting consistency and facilitate case identification [1, 37, 38]. Preventive strategies—including remineralisation therapies, desensitising agents and minimally invasive interventions—should be promptly implemented to mitigate enamel breakdown risk [38, 39].
For clinicians, integrating routine screening protocols with sealant application and desensitising agents can prevent caries progression in molars. Researchers should investigate hypomineralisation in second primary molars as early MIH predictors [40, 41], explore correlations between MIH and the DMFT index, and evaluate interventions such as fluoride, CPP‐ACP and biomimetic hydroxyapatite supplementation [42–44]. Policymakers must prioritise community‐based oral health programmes in rural areas—including mobile dental units, training for local health workers and referral systems for complex cases—to address regional MIH burden effectively. Raising awareness among parents, teachers and clinicians remains essential for early detection and intervention.
The cross‐sectional design precludes causal inference, and findings may have limited generalisability beyond the specific regional population studied. Nonetheless, the robust sample size (n = 1500) and rigorous clinical examinations enabled comprehensive MIH characterisation, enhancing reliability and international comparability. Future longitudinal studies incorporating age stratification and environmental exposure assessments would strengthen causal understanding and inform targeted interventions in similar underserved settings.
5. Conclusions
MIH prevalence among schoolchildren in Peru’s Central Jungle was 18.8%, predominantly affecting first permanent molars (84.8% upper; 90.9% lower) with less frequent incisor involvement. Pattern I distribution was most common (78.7%), while patterns II/III (21.3%) showed significant male predominance. Molars exhibited greater clinical severity with white–cream opacities, Type III lesions and higher rates of post‐eruptive breakdown and atypical caries, whereas incisors presented mainly mild demarcated opacities. These findings underscore MIH as a significant public health concern in underserved Amazonian communities, warranting enhanced surveillance and targeted preventive strategies in similar highland‐lowland transition zones.
Consent
Informed consent was obtained from all study participants.
Disclosure
All the authors have read and approved the final manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
Author Contributions
Mayra Belen Barahona‐Hernandez, Gilmer Torres‐Ramos and Daniel José Blanco‐Victorio conceived the ideas. Mayra Belen Barahona‐Hernandez and Julio César Sánchez‐Sotomayor and collected the data. Daniel José Blanco‐Victorio, Roxana Patricia López‐Ramos, Karin Harumi Uchima‐Koecklin and Gilmer Torres‐Ramos analysed the data. Mayra Belen Barahona‐Hernandez, Daniel José Blanco‐Victorio and Roxana Patricia López‐Ramos involved in reviewing and editing the manuscript.
Funding
This study was not funded.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ghanim A. , Silva M. J. , and Elfrink M. E. C. , et al.Molar Incisor Hypomineralisation (MIH) Training Manual for Clinical Field Surveys and Practice, European Archives of Paediatric Dentistry. (2017) 18, no. 4, 225–242, 10.1007/s 40368-017-0293-9, 2-s 2.0-85027412224.28721667 · doi ↗ · pubmed ↗
- 2Hanh T. T. M. , Thanh P. K. , and Ngoc V. T. N. , et al.Molar Incisor Hypomineralization in Children: Prevalence and Risk Factors From a Cross-Sectional Study in Dong Thap, Vietnam, Cureus. (2025) 17, no. 5, 10.7759/cureus.85104.PMC 1220656440589688 · doi ↗ · pubmed ↗
- 3Cabral R. N. , Nyvad B. , Soviero V. L. , Freitas E. , and Leal S. C. , Reliability and Validity of a New Classification of MIH Based on Severity, Clinical Oral Investigations. (2020) 24, no. 2, 727–734, 10.1007/s 00784-019-02955-4, 2-s 2.0-85066325733.31129878 · doi ↗ · pubmed ↗
- 4Alrehaili R. , Khalil A. , and Mergami J. , et al.Current Knowledge of the Etiology and Management of Molar Incisor Hypomineralisation in Children: A Narrative Review, Cureus. (2024) 16, no. 11, 10.7759/cureus.74770.PMC 1168282739735046 · doi ↗ · pubmed ↗
- 5Duarte M. B. S. , Carvalho V. R. , Hilgert L. A. , Ribeiro A. P. D. , Leal S. C. , and Takeshita E. M. , Is There an Association Between Dental Caries, Fluorosis, and Molar-Incisor Hypomineralisation?, Journal of Applied Oral Science. (2021) 29, 10.1590/1678-7757-2020-0890.PMC 828925434287466 · doi ↗ · pubmed ↗
- 6Linner T. , Khazaei Y. , Bücher K. , Pfisterer J. , Hickel R. , and Kühnisch J. , Hypersensitivity in Teeth Affected by Molar-Incisor Hypomineralisation (MIH), Scientific Reports. (2021) 11, no. 1, 10.1038/s 41598-021-95875-x, 17922.34504122 PMC 8429747 · doi ↗ · pubmed ↗
- 7da Costa Rosa T. , Spinelli L. R. , da Silva F. M. F. , de Castro Costa M. , and de Almeida Neves A. , Perceptions, Attitudes, and Clinical Experiences of Brazilian Dental Practitioners Towards Molar Incisor Hypomineralisation: A Cross-Sectional Study, European Archives of Paediatric Dentistry. (2024) 25, no. 6, 855–868, 10.1007/s 40368-024-00945-z.39266901 · doi ↗ · pubmed ↗
- 8Ebel M. , Bekes K. , Klode C. , and Hirsch C. , The Severity and Degree of Hypomineralisation in Teeth and its Influence on Oral Hygiene and Caries Prevalence in Children, International Journal of Paediatric Dentistry. (2018) 28, no. 6, 648–657, 10.1111/ipd.12425, 2-s 2.0-85053687414.30246468 · doi ↗ · pubmed ↗