Comparison of Adverse Reactions Between Remimazolam and Propofol in Hysteroscopic Surgery in Mainland China: A Meta‐Analysis and Systematic Review
Zirui Liu, Kexu Zhu, Zidong Zhao, Qi Zeng

TL;DR
This study compares remimazolam and propofol for hysteroscopic surgery anesthesia, finding remimazolam reduces certain adverse reactions.
Contribution
A meta-analysis showing remimazolam lowers risks of specific adverse reactions compared to propofol in hysteroscopic procedures.
Findings
Remimazolam significantly reduces respiratory depression compared to propofol.
Patients using remimazolam experience less dizziness and postoperative nausea.
No significant difference in anesthesia recovery time between the two drugs.
Abstract
The purpose of this meta‐analysis was to compare the adverse reactions of remimazolam and propofol in hysteroscopic anesthesia and to evaluate the efficacy of remimazolam in alleviating adverse reactions. We conducted a database search using China National Knowledge Infrastructure (CNKI), PubMed, and the Cochrane Library to identify randomized controlled trials (RCTs) comparing the use of remimazolam with propofol for hysteroscopy procedures. We extracted data on the occurrence of adverse reactions such as hypotension, respiratory depression, dizziness, nausea, and vomiting for meta‐analysis. Literature published until July 2024 was screened from each database, and the quality of the included studies was assessed using the bias risk assessment tool recommended by Cochrane. Data analysis was performed using RevMan 5.3 software, developed by the Cochrane Collaboration in the United…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
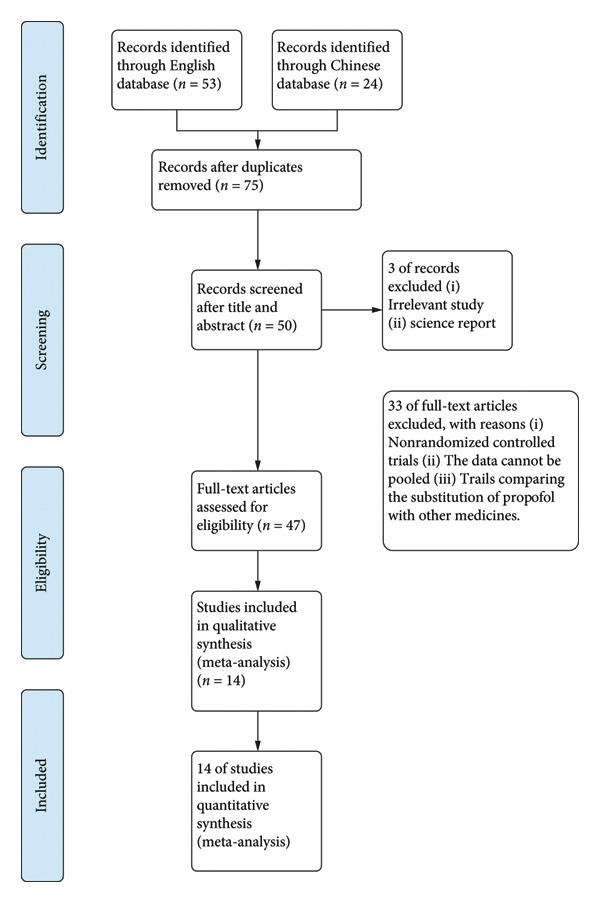 Figure 1
Figure 1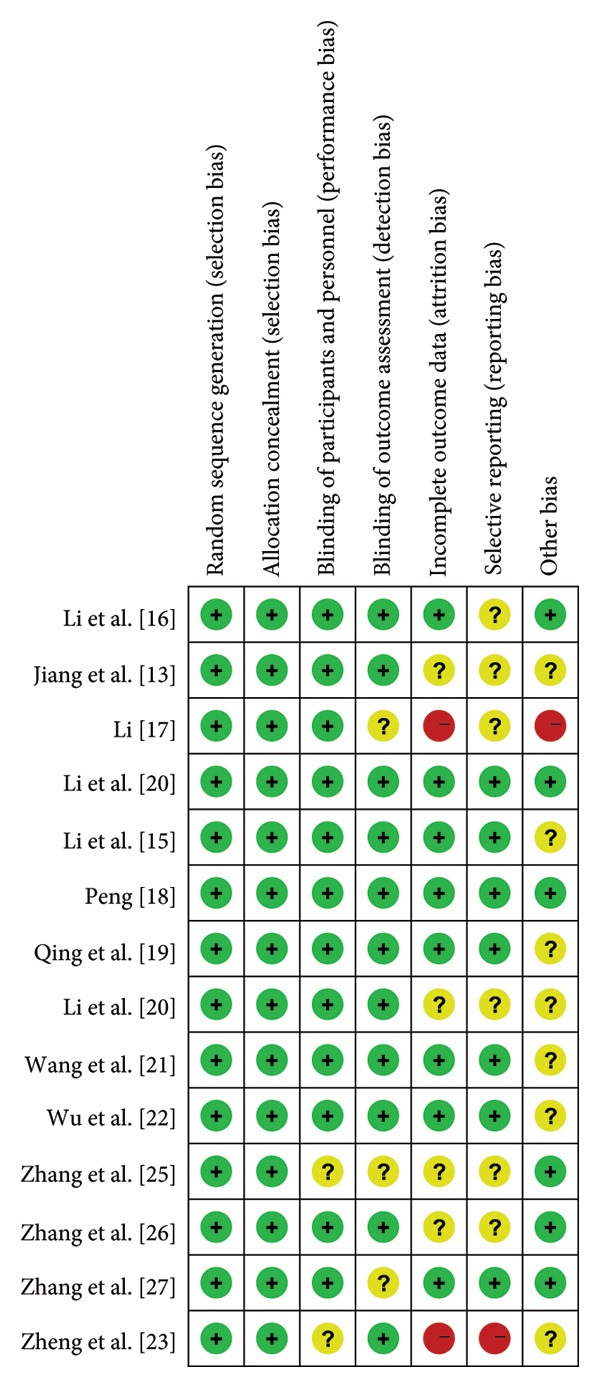 Figure 2
Figure 2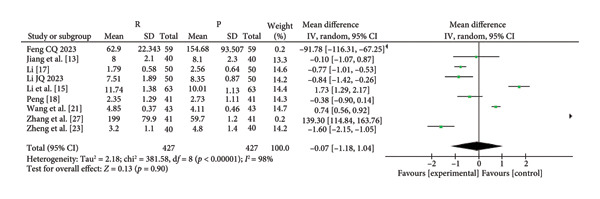 Figure 4
Figure 4| Study | Patients (T vs. C) | ASA | Intervention | Adverse reaction |
|---|---|---|---|---|
| Li [ | 50 vs. 50 | I‐II | Propofol 4.0 mg/kg 40.0 mg/min | Respiratory depression; hypotension; dizziness; PONV |
| Remit 0.1 mg/kg 40.0 mg/min | ||||
| Li et al. [ | 50 vs. 50 | I‐II | Propofol 1.5 mg/kg 2.0–5.0 mg/kg/h | Respiratory depression; dizziness |
| Remib 6.0 mg/kg/h | ||||
| Zhang et al. [ | 64 vs. 64 | I‐II | Propofol 1.5 mg/kg 4.0–10.0 mg/kg/h | Respiratory depression; hypotension; dizziness; PONV |
| Remit 0.2 mg/kg 0.4–1.0 mg/kg/h | ||||
| Zhang et al. [ | 41 vs. 41 | I‐II | Propofol 1.5–2.0 mg/kg 3.0–6.0 mg/kg/h | Respiratory depression; hypotension; dizziness |
| Remib 0.2 mg/kg 1 mg/kg/h | ||||
| Zhang et al. [ | 30 vs. 30 | I‐II | Propofol 2.0 mg/kg 5.0 mg/kg/h | Respiratory depression; PONV |
| Remit 0.25 mg/kg 0.48 mg/kg/h | ||||
| Zheng et al. [ | 40 vs. 40 | I‐II | Propofol 2.0 mg/kg 6.0 mg/kg/h | Respiratory depression; PONV |
| Remit 0.2 mg/kg 2.5 mg each time | ||||
| Wu et al. [ | 56 vs. 56 | I‐II | Propofol 2.0 mg/kg 4.0 mg/kg/h | Respiratory depression; hypotension; dizziness; PONV |
| Remib 0.4 mg/kg 1 mg/kg/h | ||||
| Wang et al. [ | 43 vs. 43 | I‐II | Propofol 2.0 mg/kg/h | Respiratory depression; dizziness; PONV |
| Remin 0.4 mg/kg 1 mg/kg/h | ||||
| Li et al. [ | 41 vs. 41 | I‐II | Propofol 2.0 mg/kg/h | Respiratory depression; dizziness; PONV |
| Remin 0.3 mg/kg 1 mg/kg/h | ||||
| Qing et al. [ | 40 vs. 40 | I‐II | Propofol 2.0 mg/kg 0.4 mg/kg each time | Dizziness |
| Remib 0.2 mg/kg 2.5 mg each time | ||||
| Peng [ | 41 vs. 41 | I‐II | Propofol 2.0 mg/kg 0.5 mg/kg each time | Respiratory depression; dizziness; PONV |
| Remin 0.2 mg/kg 2.5 mg each time | ||||
| Li et al. [ | 63 vs. 63 | I‐II | Propofol 0.5–1.5 mg/kg 3.0–5.0 mg/kg/h | Hypotension; PONV |
| Remib 0.05–0.15 mg/kg 0.3–0.5 mg/kg/h | ||||
| Jiang et al. [ | 40 vs. 40 | I‐II | Propofol 4.0 mg/kg/h | Respiratory depression; hypotension; PONV |
| Remib 1.0 mg/kg/h | ||||
| Li et al. [ | 59 vs. 59 | I‐II | Propofol 1.5–2.0 mg/kg 0.3–0.5 mg/kg each time | Hypotension; PONV |
| Remit 0.15–0.2 mg/kg 2.5 mg each time | ||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAnesthesia and Sedative Agents · Nausea and vomiting management · Gynecological conditions and treatments
1. Introduction
Hysteroscopy is among the most common minimally invasive diagnostic and therapeutic techniques for uterine diseases [1, 2]. With the advancement of assisted reproductive technology and minimally invasive techniques, as well as increased patient demands for comfortable medical procedures, outpatient painless hysteroscopy is becoming increasingly common [3, 4].
Propofol, combined with opioids, is commonly employed for sedation during hysteroscopic examinations [5, 6]. Propofol offers a rapid onset, convenient titration, and short half‐life [7]. However, propofol use is associated with pain on injection, postoperative dizziness, and respiratory depression [8, 9].
Remimazolam is a novel intravenous benzodiazepine. Like propofol, remimazolam has a rapid onset and short duration of action. Owing to its ester metabolism (similar to remifentanil), remimazolam does not accumulate in tissues and is metabolized independently of liver and kidney function. Remimazolam is widely used for both sedation as well as anesthesia induction and maintenance [10]. On July 2, 2020, the U.S. FDA approved the market release of remimazolam for sedation during medical procedures (lasting up to 30 min) in adult patients [11, 12].
Remimazolam was approved for use in China in 2019, where it is manufactured by two pharmaceutical companies. A substantial amount of clinical data and usage experience has been published since its introduction. Given that China is a multiethnic country, the extensive patient data obtained from its use holds certain representativeness, particularly for Japan and South Korea, whose populations predominantly identify as Asian.
This meta‐analysis compares the clinical and adverse effects of remimazolam and propofol in patients requiring sedation for hysteroscopy.
2. Research Methods and Materials
We conducted a systematic review and meta‐analysis based on the Cochrane Intervention Measures Handbook. We presented our findings using the preferred reporting items outlined in the Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA) guidelines. We registered this study with PROSPERO with the registration ID: CRD42023464718.
2.1. Search Strategy and Selection Criteria
To retrieve relevant literature databases online, we utilized several English resources, including PubMed and the Cochrane Library, as well as the Chinese database China National Knowledge Infrastructure (CNKI). Our search was conducted from the date of product approval through July 2024. In the English databases, we used the search query “(Remimazolam) AND (hysteroscopy)” for retrieval purposes, while in the Chinese database, we applied the search query “((Remimazolam) AND (propofol)) AND (hysteroscopy).”
2.2. Eligibility Criteria
The six predefined criteria for evidence selection were as follows: (1) randomized controlled trials (RCTs), (2) studies that involved adult patients older than 18 years who underwent medical procedures with procedural sedation using propofol or remimazolam, (3) studies that reported at least one comparative outcome of remimazolam and propofol, (4) the patient underwent hysteroscopy, (5) the sample size was at least 20, (6) article written in English or Chinese, and (7) patients from mainland China.
2.3. Exclusion Criteria
The studies were considered ineligible when any of the following criteria were met:
- (1)They were review articles, case reports, case series, retrospective data analysis, or nonrandomized prospective studies.
- (2)The data in the articles could not be pooled or were not relevant, thus rendering the study unsuitable for meta‐analysis.
- (3)The trials compared propofol with other sedatives.
- (4)Duplicate searches across different databases.
2.4. Data Extraction and Quality Evaluation
We extracted the data from eligible articles, including (1) the first author’s name, (2) publication year, (3) country, (4) American Society of Anesthesiology (ASA) score, (5) sample size, (6) procedure type, and (7) protocol of procedural sedation.
2.5. Assessment of Risk of Bias
To classify each article as low or high risk of bias or unclear risk of bias, we used the Cochrane Collaboration tool, which involved 7 items to evaluate the risk of bias.
2.6. Statistical Analysis
We used Review Manager V5.3 to perform the statistical analysis. Categorical variables were expressed as the relative risk (RR) with a 95% confidence interval (CI), while continuous variables were expressed as the standardized mean difference (SMD) with a 95% CI.
To address potential sensitivity and heterogeneity concerns, a model‐altering approach was implemented in this study. The I ^2^ statistic was utilized to assess heterogeneity, whereby an I ^2^ value exceeding 50% indicated high heterogeneity and led to the adoption of a random‐effects model. Conversely, if the I ^2^ value fell below 50%, it indicated lower heterogeneity, prompting the use of a fixed‐effects model. Publication bias was assessed using the Cochrane Collaboration risk of bias tool. Funnel plots were used to assess the goodness of fit.
2.7. Outcomes
Our primary objective was to compare the safety of remimazolam and propofol by analyzing the incidence of adverse events associated with their use. These adverse effects included hypotension, respiratory depression, dizziness, and postoperative nausea and vomiting. In addition, we evaluated the time to recovery from anesthesia as a secondary outcome to show the perioperative effects of the two anesthetics.
3. Results
3.1. Study Selection
Figure 1 illustrates the detailed flowchart of article selection. We retrieved 53 articles from the English database. We retrieved 24 articles from the Chinese database. Two of the Chinese articles were excluded due to duplicate searches. We excluded 25 articles describing animal experiments. We excluded 33 of the remaining papers as they did not meet the inclusion criteria for analysis.
PRISMA flowchart diagram. We initially extracted 75 potential references. Screening the titles and abstracts yielded 47 full‐text articles, the eligibility of which was assessed. Eventually, 14 studies were included for qualitative and quantitative syntheses. PRISMA = Preferred reporting items for systematic reviews and meta‐analyses.
3.2. Study Characteristics
In the end, we included 14 RCTs involving 633 subjects in the meta‐analysis, and the details are demonstrated in Table 1 [13–27]. The publication year of the included studies ranged from 2021 to 2024. All enrolled patients met the screening criteria.
3.3. Risk of Bias in the Included Studies
We categorized seven articles as having an “ambiguous risk of bias” because they did not clearly state participant blinding and the utilization of blind assessment methods for evaluating results (Figure 2). These seven articles included RCTs with comprehensive data on relevant symptoms and originated from significant hospitals across China; we evaluated the potential for incomplete or selective publication of data, as well as the risks associated with withdrawal and reporting biases. For those articles that have a high risk of bias when evaluated using RevMan software, as well as those that do not meet the evaluation criteria of this study in terms of experimental design, they were not included in this meta‐analysis. This evaluation took into account the influence of the hospitals involved and the quality of the journals in which the RCTs were published (refer to Figure 2).
Risk of bias graph: review authors’ judgments about each risk of bias item presented as percentages across all included studies. + = Low risk; ? = unclear; − = High risk.
3.4. Safety and Efficacy of Remimazolam Versus Propofol
The pooled results demonstrated that patients given remimazolam for procedural sedation had a lower risk of hypotension (RR: 5.25; 95% CI: [2.63, 10.48]; I ^2^ = 0%; p < 0.00001), respiratory depression (RR: 0.19 95% CI: [0.11, 0.33]; I ^2^ = 0%; p < 0.00001), dizziness (RR: 0.10; 95% CI: [0.04, 0.31]; I ^2^ = 0%; p < 0.0001), and postoperative nausea and vomiting (RR: 0.60; 95% CI: [0.15, 2.46]; I ^2^ = 0%; p = 0.48) (Figure 3). The characteristics of the included studies in the meta‐analysis are listed in Table 1. Among the five indicators of adverse reactions, only nausea and vomiting had no significant statistical significance (p slightly greater than 0.05). No obvious differences were observed in anesthesia recovery time (MD: −0.07; 95% CI: [−0.18–1.04]; I ^2^ = 98%; p = 0.90; Figure 4) between the remimazolam and propofol groups and the procedure duration. The I ^2^ value for the anesthesia recovery time reached 98%, indicating a significant heterogeneity in this measure. The aforementioned adverse reaction results exhibited no considerable heterogeneity, and the included RCTs displayed no significant disparities concerning age, gender, ASA, and other collected data. Moreover, there was no evidence suggesting a significant distinction in clinical outcomes between these two drugs. We tried to exclude some included references to test sensitivity, but the statistical significance did not change after the exclusion of some references, so the sensitivity was considered low.
Figure 3. Specific forest map of adverse reactions of remimazolam and propofol. (a) Hypotension. (b) Respiratory depression. (c) Dizziness. (d) Postoperative nausea and vomiting.(a)(b)(c)(d)
Forest map of remimazolam and propofol anesthesia recovery time.
3.5. Publication Bias
To assess publication bias, the Cochrane Collaboration risk of bias tool was used, and the funnel plot was also used to assess publication bias based on the primary outcome. The two funnel plots for the respiratory depression and hypotension indexes in this study were visually asymmetrical around the midline, indicating the presence of publication bias in these studies. The funnel plots of dizziness and postoperative nausea and vomiting were visually symmetrical to the midline, so publication bias was not considered (Figure 5).
Figure 5. The results of the funnel plot. (a) Hypotension. (b) Respiratory depression. (c) Dizziness. (d) Postoperative nausea and vomiting.(a)(b)(c)(d)
4. Discussion
When utilized for anesthesia during hysteroscopy, remimazolam demonstrates a lower incidence of adverse reactions compared to propofol. It effectively mitigates postanesthetic complications, including hypotension, respiratory depression, dizziness, and postoperative nausea and vomiting, making it a viable choice for hysteroscopy procedures. Consistent with previous literature [28], we found no significant disparity in the awakening time between remimazolam and propofol. These data suggest that remimazolam is a better option for sedation in patients undergoing hysteroscopy, and likely for other endoscopic procedures as well.
Although injection pain during anesthesia is not considered a major complication, it can cause discomfort and anxiety in patients. Women who undergo hysteroscopy, in particular, often express concern about potential pain and discomfort during the procedure. A large body of literature and clinical practices have confirmed that propofol is significantly associated with injection pain, while remimazolam is an ester benzodiazepine containing different components, which can theoretically reduce injection pain [29–32]. Our research findings substantiate the idea that remimazolam significantly reduces injection pain compared to propofol, providing patients with an enhanced experience and aligning with the principles of painless surgery.
The I ^2^ value for the anesthesia recovery time reached 98%, indicating a significant heterogeneity in this measure. This could be attributed to the different types of intravenous anesthetics used during surgery, as well as variations in the dosages maintained for each anesthetic during the procedure, resulting in the observed heterogeneity. In addition, individual differences among patients and variations in their ability to metabolize anesthetics may also contribute to the heterogeneity. However, since the patients included in this study did not exhibit significant differences in terms of age and gender, it is believed that the possibility of individual differences causing the observed heterogeneity is relatively low. Moreover, the varying methods of drug combinations used in anesthesia presented challenges in merging identical data.
Remimazolam carries a higher economic burden in comparison to the currently utilized anesthetic drugs for hysteroscopy. This may impose financial constraints on Chinese patients. The clinician should discuss the cost of remimazolam compared to propofol with patients to determine whether the advantages associated with remimazolam justify the additional cost.
The 14 RCTs included in our analysis were conducted across Mainland China. As a multiethnic country in Asia, this study, to some extent, reflects the influence of racial factors on treatment outcomes among Asian patients, thereby holding a certain level of representativeness and practical significance. However, in broader regions across other continents, more specific evaluations are needed based on their unique clinical practices.
5. Conclusion and Limitation
Since remifentanil has only been available in China for 6 years, there are only a few RCTs that meet our criteria. Second, our primary focus was to compare adverse reactions associated with remimazolam and propofol.
In conclusion, remimazolam is associated with a similar onset and offset to propofol when used for hysteroscopy sedation; however, it is associated with fewer adverse effects.
Ethics Statement
No ethical approval was required for the present study since the data were solely collected from CNKI, PubMed, and Cochrane Library databases.
Conflicts of Interest
The authors declare no conflicts of interest.
Author Contributions
Zirui Liu: conceptualization, validation, data extraction and curation, methodology and software search, initial drafting, figure generation, article revisions, and project management. Kexu Zhu: initial drafting, writing of comments, and editing. Zidong Zhao: supervision, investigation, and data curation. Qi Zeng: content guidance and English language editing.
Funding
No funding was received for this study.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Okohue J. E. , Overview of Hysteroscopy, West African Journal of Medicine. (2020) 37, no. 2, 178–182.32150637 · pubmed ↗
- 2Cela V. , Litta P. , Franchini M. et al., Fertility-Enhancing Hysteroscopic Surgery, Minerva Ginecologica. (2016) 68, no. 2, 167–174.26928416 · pubmed ↗
- 3Bettocchi S. , Achilarre M. T. , Ceci O. , and Luigi S. , Fertility-Enhancing Hysteroscopic Surgery, Seminars in Reproductive Medicine. (2011) 29, no. 2, 75–82, 10.1055/s-0031-1272469, 2-s 2.0-79953197597.21437821 · doi ↗ · pubmed ↗
- 4Murdoch J. A. and Gan T. J. , Anesthesia for Hysteroscopy, Anesthesiology Clinics of North America. (2001) 19, no. 1, 125–140, 10.1016/s 0889-8537(05)70215-7, 2-s 2.0-0035123772.11244913 · doi ↗ · pubmed ↗
- 5Knigge S. and Hahnenkamp K. , Nonoperating Room Anesthesia for Endoscopic Procedures, Current Opinion in Anaesthesiology. (2017) 30, no. 6, 652–657, 10.1097/aco.0000000000000518, 2-s 2.0-85033779785.28938299 · doi ↗ · pubmed ↗
- 6Cho Y. J. , Role of Anesthesia in Endoscopic Operations, Gastrointestinal Endoscopy Clinics of North America. (2021) 31, no. 4, 759–772, 10.1016/j.giec.2021.05.011.34538414 · doi ↗ · pubmed ↗
- 7Ferrier D. C. , Kiely J. , and Luxton R. , Propofol Detection for Monitoring of Intravenous Anaesthesia: A Review, Journal of Clinical Monitoring and Computing. (2022) 36, no. 2, 315–323, 10.1007/s 10877-021-00738-5.34213720 PMC 9123036 · doi ↗ · pubmed ↗
- 8Nishizawa T. and Suzuki H. , Propofol for Gastrointestinal Endoscopy, United European Gastroenterology Journal. (2018) 6, no. 6, 801–805, 10.1177/2050640618767594, 2-s 2.0-85044570574.30023057 PMC 6047291 · doi ↗ · pubmed ↗