A Rare Case of RNRVAS Termination and Re‐Initiation Visualized on a 12‐Lead ECG
Tomoyoshi Morioku, Yasuyuki Egami, Yasuharu Matsunaga‐Lee, Masamichi Yano, Masami Nishino

TL;DR
A rare heart rhythm pattern called RNRVAS was observed and captured on an ECG, showing how pacemaker settings and heart conditions can influence it.
Contribution
The paper presents a unique visualization of RNRVAS termination and re-initiation using a standard 12-lead ECG.
Findings
RNRVAS termination and re-initiation were clearly captured on a 12-lead ECG.
Pacemaker algorithms and abnormal atrial refractoriness play roles in triggering or terminating RNRVAS.
Abstract
This case illustrates both termination and re‐initiation of repetitive non‐reentrant ventriculoatrial synchrony (RNRVAS) visualized on a standard 12‐lead ECG. It highlights how pacemaker algorithms such as VIP and PVC response, together with abnormal atrial refractoriness, can trigger or terminate RNRVAS.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
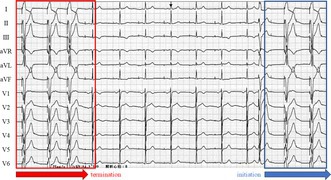 Figure 1
Figure 1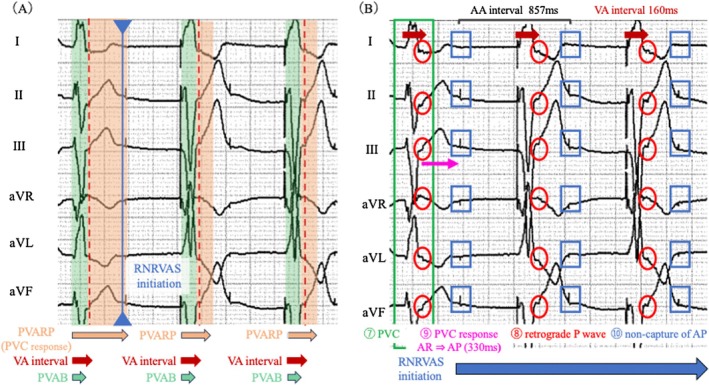 Figure 2
Figure 2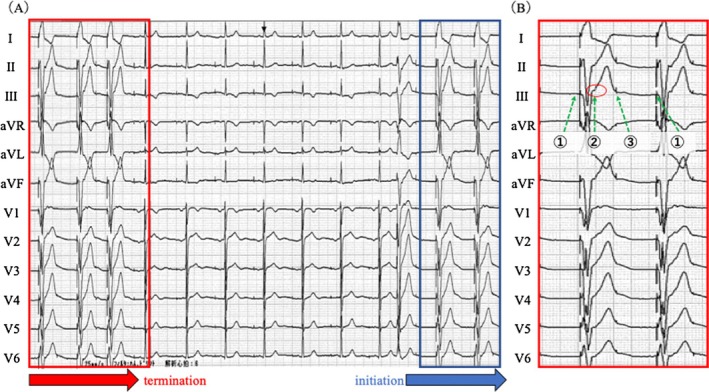 Figure 3
Figure 3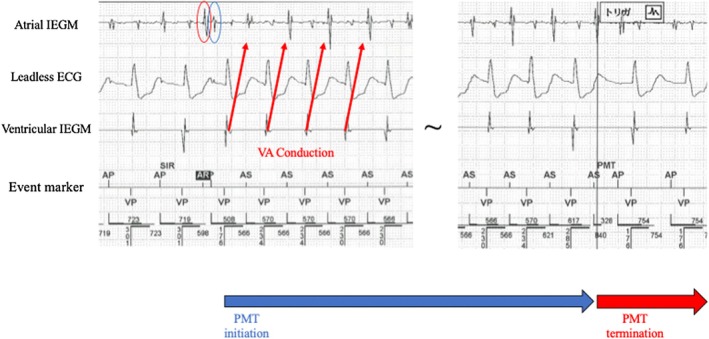 Figure 4
Figure 4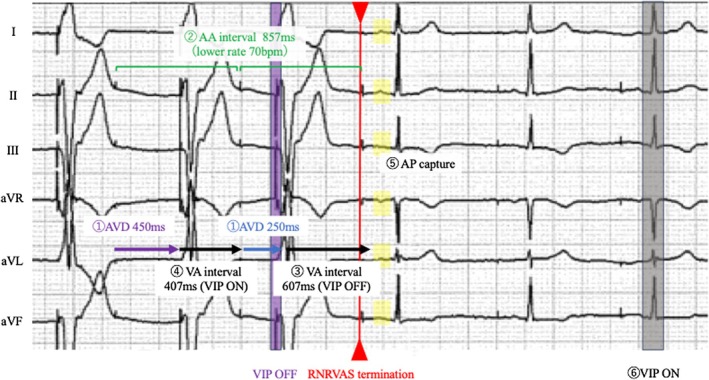 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac pacing and defibrillation studies · Cardiac Arrhythmias and Treatments · Cardiac electrophysiology and arrhythmias
The diagnosis of pacemaker malfunction typically relies on telemetry interrogation. However, careful analysis of a 12‐lead electrocardiogram (ECG), combined with knowledge of pacemaker algorithms, enables accurate diagnosis without interrogation. A 76‐year‐old woman with sick sinus syndrome underwent dual‐chamber pacemaker implantation (Zephyr XL DR 5826, Abbott) six years earlier for symptomatic bradycardia. The pacemaker was programmed in DDD mode with the following settings: lower rate, 70 bpm; maximum tracking rate, 105 bpm; atrioventricular delay (AVD): paced/sensed, 250/225 ms; post‐ventricular atrial refractory period (PVARP), 275 ms; post‐ventricular atrial blanking (PVAB), 150 ms; ventricular intrinsic preference (VIP), ON with a 200‐ms AVD extension to encourage intrinsic conduction; and PVC response, ON.
She remained asymptomatic and continued follow‐up. During a routine visit, a 12‐lead ECG was recorded at rest (Figure 1). The ECG (25 mm/s, 10 mm/mV) revealed abrupt cessation and re‐initiation of ventricular pacing (VP), demonstrating repetitive non‐reentrant ventriculoatrial synchrony (RNRVAS), a rare pacemaker‐mediated arrhythmia (Figure 1B). VP stimulus (①) was followed by a retrograde atrial activation (② red circle), and the subsequent atrial pacing (AP) (③) occurred during the atrial refractory period, resulting in non‐capture. This sequence (VP → retrograde P wave → non‐capture of AP) repeated in a loop, fulfilling the diagnostic criteria for RNRVAS [1]. The ventriculoatrial (VA) conduction time (for both premature ventricular contraction [PVC] and VP) measured on the 12‐lead ECG was 160 ms. VA conduction was confirmed on the intracardiac electrogram during a pacemaker‐mediated tachycardia (PMT) event, where VP was followed by atrial sensing (AS). The VA conduction time was approximately 340 ms, exceeding the PVARP (275 ms) and resulting in AS recognition and PMT initiation (Figure 2). RNRVAS persisted until the first intrinsic ventricular beat, then terminated with VIP OFF. The VIP algorithm promotes intrinsic conduction by extending the AVD and switches between ON and OFF every 30 s with three cycles. VIP turns OFF when VP occurs for three consecutive beats during the extended AVD and turns ON when three consecutive VS events are detected either during the extended AVD or within the normal AVD. In this case, the sequence of VIP OFF and ON was as follows (Figure 3):
① Three consecutive VP events occurred during extended AVD of 450 ms.
② VIP turned OFF, and the AVD returned to its baseline value of 250 ms.
③ The VA interval was extended to 607 ms (857–250 = 607).
④ In the previous beat, when VIP was active, the VA interval was 407 ms (857–450 = 407).
⑤ This extended VA interval (③) allowed the AP stimulus to capture the atrium (highlighted in yellow) beyond the physiologic refractory period caused by the preceding retrograde conduction, resulting in RNRVAS termination. Thus, the transition from VIP ON to OFF status restored the baseline AVD, prolonged the VA interval, and interrupted the RNRVAS loop.
⑥ Subsequently, VIP was reactivated after three consecutive VS detections within the normal AVD.
At the time of RNRVAS initiation triggered by the PVC, the PVAB was 150 ms, the PVARP under PVC response was 480 ms, and the normal PVARP was 275 ms (Figure 4). As shown in Figure 4, a PVC (⑦ green box) was followed by a retrograde P wave (⑧ red circle). After the PVC, the pacemaker activated the PVC response algorithm designed to prevent PMT. The PVC response algorithm functions as follows: If a retrograde atrial event is sensed within the PVARP (extended to 480 ms), the device delivers an AP stimulus 330 ms after the atrial refractory (AR) event to restore atrioventricular synchrony and resume normal operation. Otherwise, if no atrial event is sensed within the PVARP, the device delivers AP after the programmed VA interval (Figure S1). In this case, the algorithm operated according to the first condition, delivering an AP stimulus 330 ms after AR detection (⑨ magenta arrows). However, because the atrium was still within its physiological refractory period, the AP resulted in non‐capture of AP (⑩ blue boxes). In this case, approximately 150 ms elapsed from the captured AP to the end of the atrial wave, suggesting abnormally prolonged atrial activation and refractory period likely leading to AP without atrial capture. Prolonged VA conduction, drug‐induced atrial refractoriness [2], and delayed atrial activation may contribute to RNRVAS development. This suggests that algorithms designed to prevent PMT may paradoxically trigger RNRVAS, highlighting the importance of understanding programming and atrial refractoriness.
This case represents a rare instance in which both termination and re‐initiation of RNRVAS were clearly documented on a standard 12‐lead ECG. Unlike reports using intracardiac electrograms or Holter monitoring [3], this case demonstrates the full RNRVAS sequence on surface ECG. To distinguish RNRVAS from other pacemaker‐mediated rhythms, understanding pacing dynamics and rate characteristics is essential. Among these, PMT is most representative. RNRVAS occurs near the lower pacing rate, whereas PMT appears at the upper tracking rate, where retrograde P waves are tracked as atrial sensing. Recognizing these differences allows differentiation using a 12‐lead ECG.
In this case, both pacing algorithms (VIP and PVC response) and the abnormally prolonged atrial activation with its refractory period may have contributed to RNRVAS termination and recurrence. Although triggered by a PVC, RNRVAS might also occur during ventricular pacing with an AVD plus VIP extension under atrioventricular block. Other manufacturers' platforms rely on post‐PVC PVARP extension without early atrial pacing, making this specific mechanism of RNRVAS less likely. These manufacturers‐specific differences underscore the need to tailor programming to the device and patient physiology. In addition, lowering the lower pacing rate from 70 to 60 bpm to avoid atrial pacing during the refractory period caused by retrograde conduction delayed the timing of atrial pacing, restored atrial capture, and markedly reduced RNRVAS episodes. In this case, RNRVAS was asymptomatic and incidentally detected. However, previous reports have shown that atrial pacing during the relative refractory period, also known as the vulnerable period, during RNRVAS can induce atrial arrhythmias [2], and that atrioventricular dyssynchrony may worsen heart failure [4]. Therefore, even asymptomatic RNRVAS warrants consideration of device reprogramming to prevent future arrhythmias or heart failure.
Funding
The authors have nothing to report.
Ethics Statement
The authors have nothing to report.
Consent
The patient provided written informed consent for the ablation procedures and agreed to the publication of his case details and images in this report.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Figure S1: joa370270‐sup‐0001‐FigureS1.zip.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1S. S. Barold and P. A. Levine , “Pacemaker Repetitive Nonreentrant Ventriculoatrial Synchronous Rhythm. A Review,” Journal of Interventional Cardiac Electrophysiology 5, no. 1 (2001): 45–58.11248774 10.1023/a:1009853723766 · doi ↗ · pubmed ↗
- 2L. Garber , E. Shulman , A. Kushnir , T. Saraon , D. S. Park , and L. A. Chinitz , “Repetitive Nonreentrant Ventriculoatrial Synchrony Inducing Atrial Fibrillation in Setting of Dofetilide,” Heart Rhythm Case Reports 8, no. 5 (2022): 320–324.35607350 10.1016/j.hrcr.2022.01.015PMC 9123322 · doi ↗ · pubmed ↗
- 3S. S. Barold , R. X. Stroobandt , and F. Van Heuverswyn , “Pacemaker Repetitive Nonreentrant Ventriculoatrial Synchrony. Why Did Automatic Mode Switching Occur?,” Journal of Electrocardiology 45, no. 4 (2012): 420–425.22560600 10.1016/j.jelectrocard.2012.04.003 · doi ↗ · pubmed ↗
- 4S. Andric , D. Tesic , D. Somer , et al., “Ventriculoatrial Synchrony Induced Heart Failure,” Acta Clinica Belgica 73, no. 6 (2018): 439–443.29466924 10.1080/17843286.2018.1443002 · doi ↗ · pubmed ↗