Health care use as an aspect of immigrant integration? An analysis of health care cost convergence among new immigrants and natives in Finland
Maria Vaalavuo, Tuukka Holster, Natalia Skogberg, Heidi Kuusinen

TL;DR
The study finds that immigrants in Finland use less healthcare than natives, and this gap doesn't close over time, even for more integrated immigrants.
Contribution
The paper introduces a novel analysis of healthcare cost convergence and integration factors among immigrants in Finland using longitudinal register data.
Findings
Immigrant healthcare costs remain lower than natives' and do not converge over seven years.
More integrated immigrants show narrower gaps, but convergence is still modest.
Healthcare costs vary significantly between immigrant groups and other factors.
Abstract
•Health care use and costs of recent immigrants remain lower compared to native Finnish population over time.•Accounting for other measures of integration narrows the gap between immigrants and natives, but convergence over time remains modest among more integrated immigrants too.•Significant differences in health care costs exist between immigrant groups.•In addition to better health, the results can indicate unmet health care needs among immigrants.•In the context of increasing immigration, improving access to health care among immigrants is important for ensuring health equity. Health care use and costs of recent immigrants remain lower compared to native Finnish population over time. Accounting for other measures of integration narrows the gap between immigrants and natives, but convergence over time remains modest among more integrated immigrants too. Significant differences in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
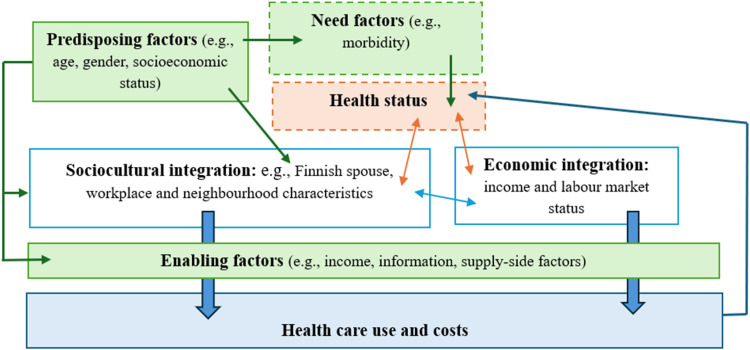 Figure 1
Figure 1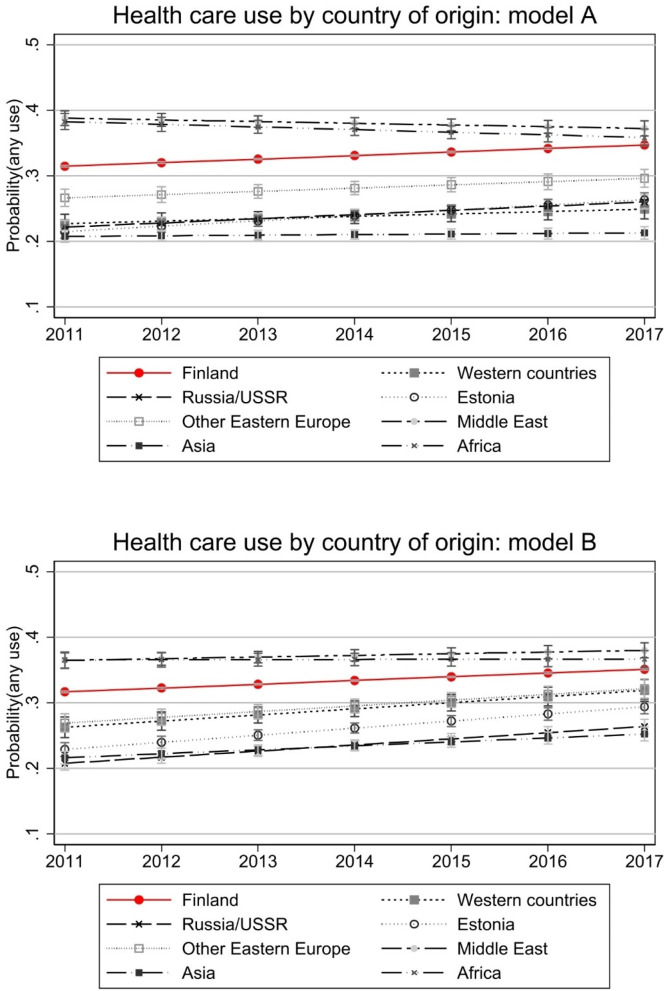 Figure 2
Figure 2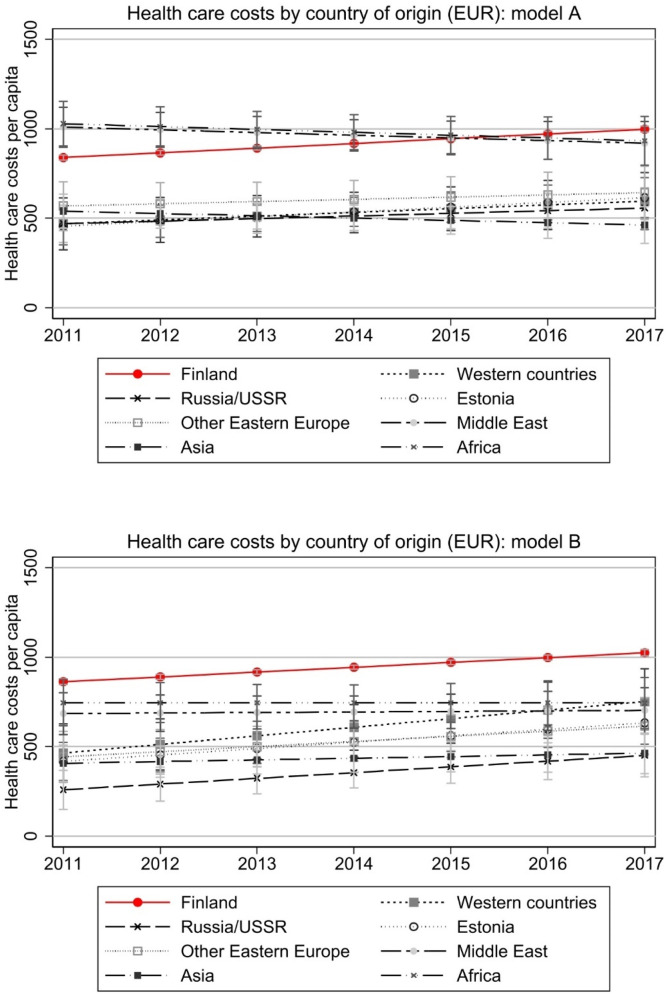 Figure 3
Figure 3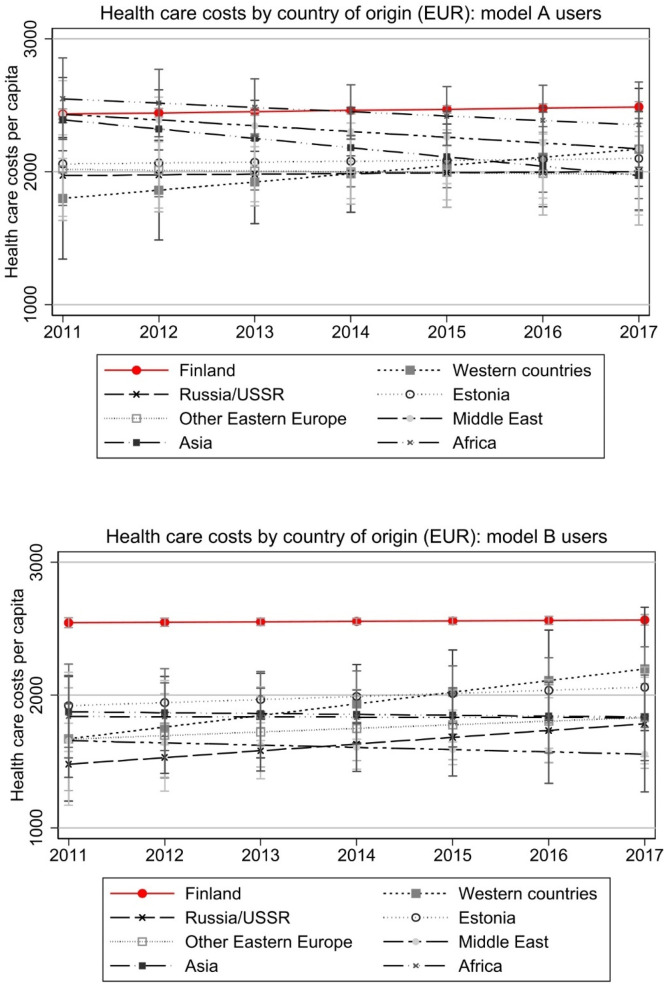 Figure 4
Figure 4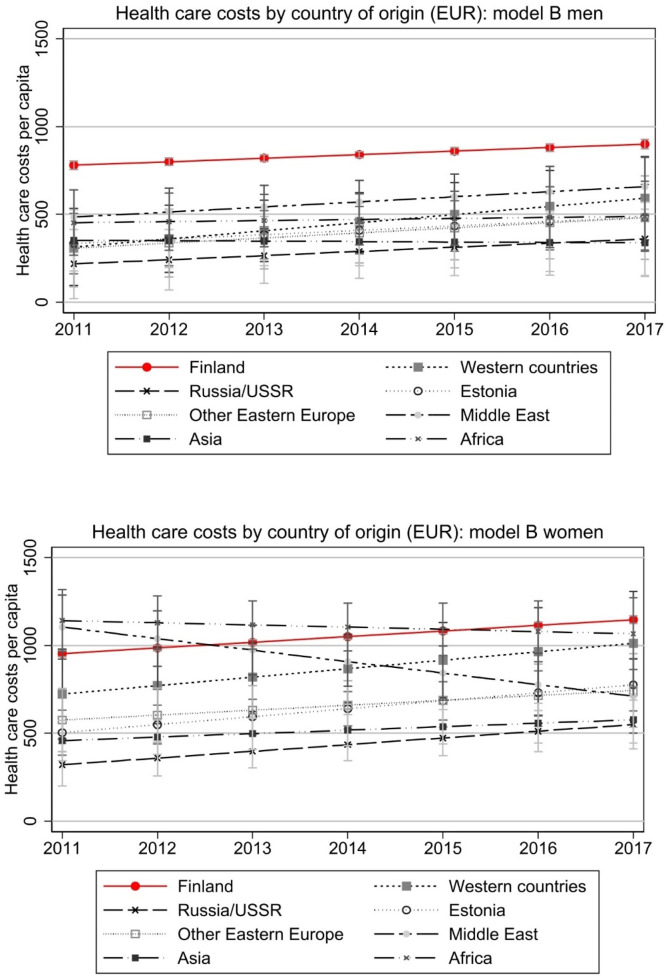 Figure 5
Figure 5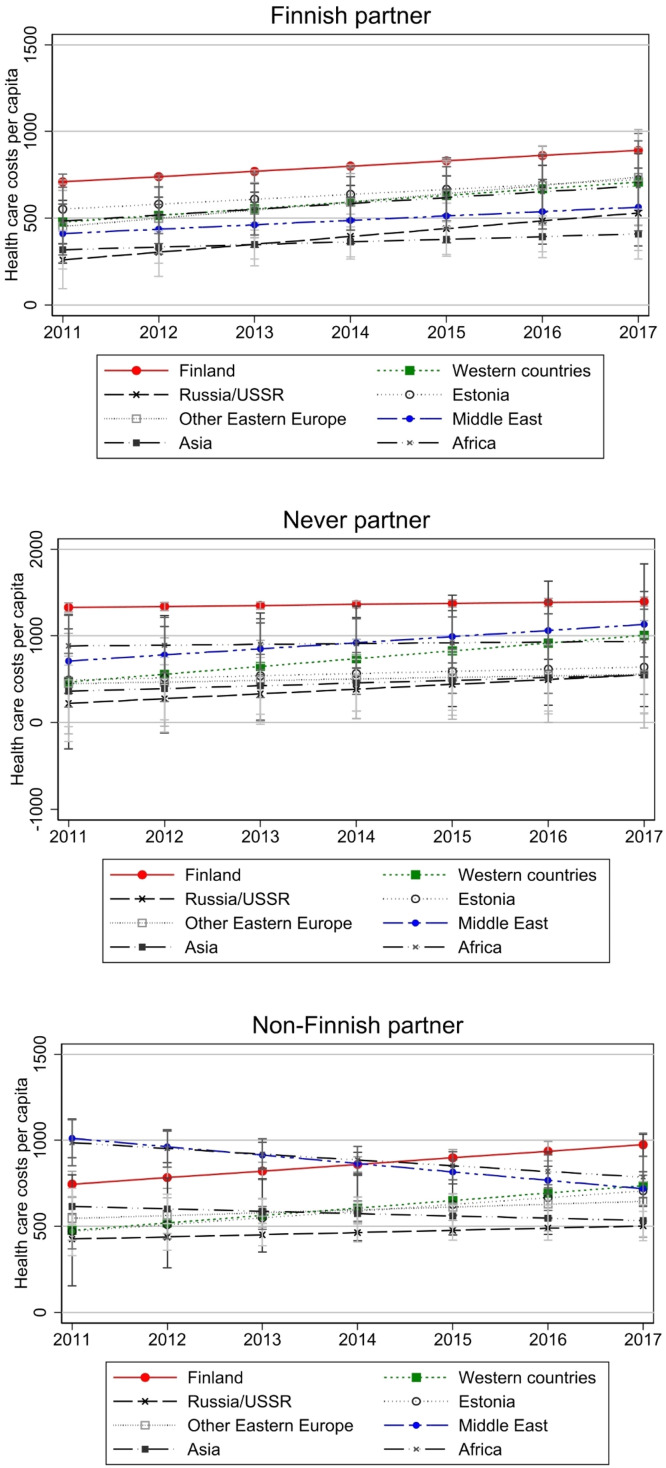 Figure 6
Figure 6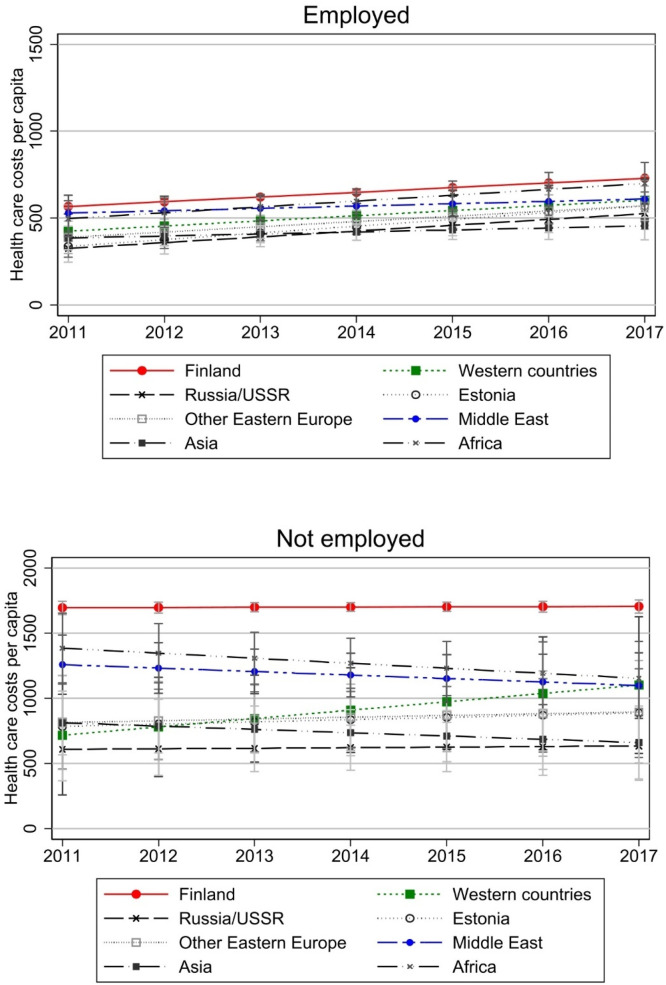 Figure 7
Figure 7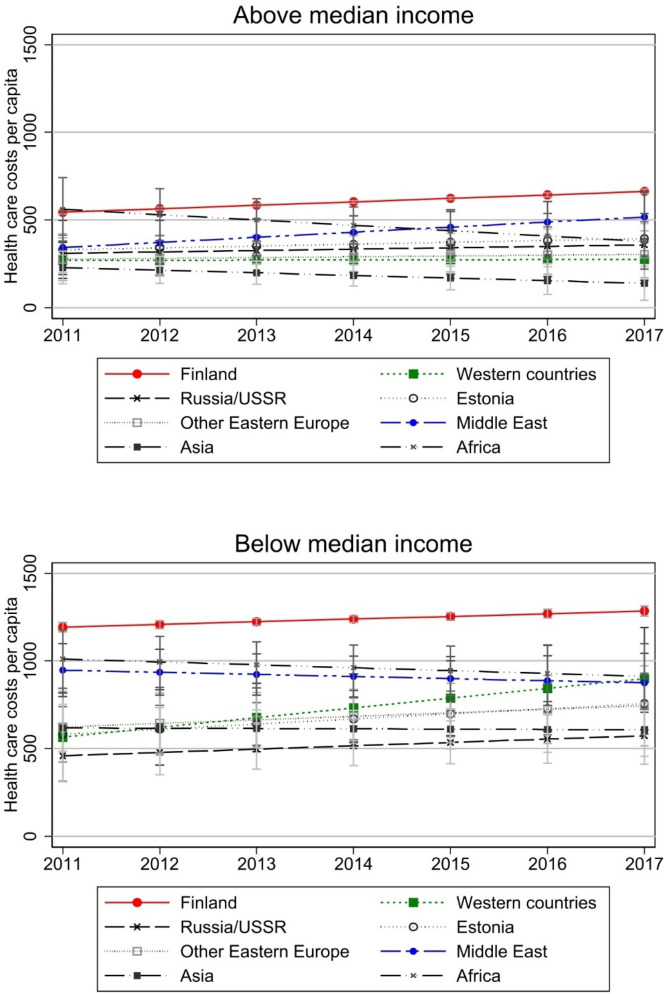 Figure 8
Figure 8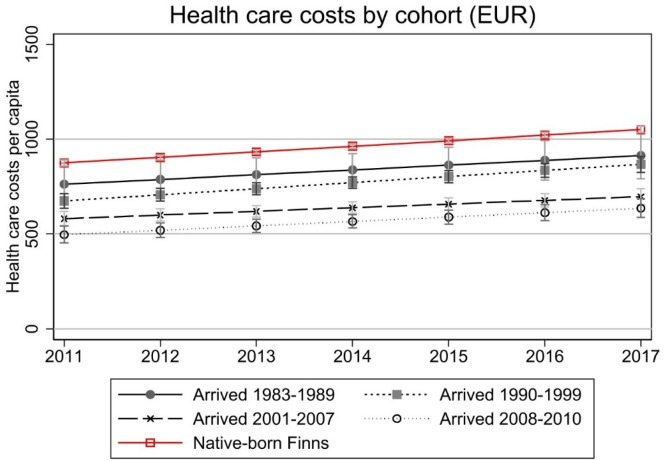 Figure 9
Figure 9Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMigration, Health and Trauma · Healthcare Systems and Reforms · Racial and Ethnic Identity Research
Introduction
1
Alongside an aging population, one of the most prominent factors affecting the population structure in European welfare states is immigration. Although net migration into Finland, a Nordic welfare state, is a relatively new phenomenon, the number of immigrants has steadily grown since the 1990′s. Today 9.6 per cent of the Finnish population has been born abroad (Statistics Finland, 2023). In the context of increasing diversity, understanding differences in the determinants of health care use and improving access to health care among immigrants is important for ensuring health equity. In Finland, the Health Care Act (1326/2010) aims to reduce health inequalities between population groups and to ensure equal access, quality, and patient safety. Still, significant disparities have been observed in both health outcomes and health care use based on socioeconomic status and other factors (e.g., van Doorslaer et al., 1997; Huijts et al., 2010; Vaalavuo, 2020).
Immigrants in Finland are a heterogenous group, showing both health advantages and disadvantages in health compared with the general Finnish population. On average, immigrants in Finland have a lower prevalence of self-reported long-term illnesses (Laatikainen et al., 2020). Other studies have found that the prevalence of psychological distress and diabetes is generally higher among immigrants compared to the general population (Skogberg et al., 2018; Robertsson et al., 2023). It is also important to note that pronounced differences in health tend to emerge when data is disaggregated by region of origin, with particularly immigrants of Middle Eastern and African origin overrepresented among those with greater health problems (Rask et al., 2016; Skogberg et al., 2016, 2018; Robertsson et al., 2023).
Existing studies have found that immigrants generally have lower health care use and costs compared to the majority population (e.g., Wilson et al., 2020; Çilenti et al., 2021; Kieseppä et al., 2020; Xu et al., 2021; Barlow et al., 2022). While some studies propose this may be due to inequality in access to health care (supply-related factors), other studies suggest it is due to lower overall need for these services (demand-related factors). The latter explanation draws from the literature on the “healthy immigrant effect” (HIE) that posits that immigrants tend to be healthier than individuals from both the receiving country and the country of origin as selection occurs, with those who are healthier being more likely to migrate and to stay in the destination country (e.g., McDonald and Kennedy, 2004; Kennedy et al., 2015; Holz, 2022; Hagos and Hamilton, 2024). The health effect is especially observed in the immediate years after migration, while “acculturation” is argued to result in smaller native-immigrant health differences in the longer term (Hagos and Hamilton, 2024). In fact, the “weathering” hypothesis argues that immigrants experience a more rapid health decline with age (Loi et al., 2025). However, a recent study from Finland argues that the HIE continues until old age with evidence on migrant mortality advantage across various causes of death (Kemppainen et al., 2024).
The HIE theory has also been contested as it oversimplifies an intricate, complex, and multidimensional phenomenon (e.g., Vang et al., 2016; Helgesson et al., 2019; Elshahat et al., 2022). It seems unlikely that health is the only factor causing differences in health care use. The country of origin, the conditions in the country of origin as well as in the country of destination, the reason for migration, and the process of immigration and integration all contribute to immigrants’ health and health care use in addition to the typical factors affecting health care use and social determinants of health. Previous research has also highlighted multiple barriers in immigrants’ access to health services, such as language, unsatisfactory experiences, inadequate knowledge about available services and perceptions about where and when to seek care (Akhtar et al., 2022; Pandey et al., 2022; Arsenijevic and Seibel, 2024). Consequently, achieving equal access and use of services as well as equal outcomes of health care use may require a high level of sociocultural integration from immigrants, as navigating the health care system can prove to be difficult even among the natives. Various forms of social, cultural, and economic capital are necessary to understand how the health care system works, and what services are available (Willis et al., 2016; Straiton and Myhre, 2017).
Our study combines research interests and wider societal concerns about health care costs, immigration integration, and health inequality. The aim is to study how health care use and costs differ among immigrants and native population in Finland. Using rich register data and following health care costs in public specialized health care from 2011 to 2017, we ask:
- 1)How do average health care costs per capita in public specialized health care sector differ between newly arrived immigrant groups and natives in Finland?
- 2)Do costs among the immigrants converge to the level of natives over the 7-year observation period?
- 3)How do the individual health care cost trajectories vary between different immigrant groups and over time?
- 4)Does integration in other areas foster convergence of health care costs between immigrants and natives?
It is important to look at the health care use and costs among immigrants. In this study, we approach the convergence of health care costs between immigrants and natives as a potential indicator of integration within the health care system. First, it may reflect integration in the service system of the country of migration, which we regard to be an important aspect of integration. However, we acknowledge that convergence in costs is a complex indicator, which does not necessarily indicate successful integration. It may reflect changes in health status (e.g., health deterioration or “weathering”), growing familiarity with the health care system, or improved access to services. Therefore, we interpret cost convergence cautiously and discuss it alongside alternative explanations such as acculturation processes, differences in unmet health care needs, and varying health trajectories after migration. We also study cost convergence in relation to other dimensions of integration. Second, it enhances our understanding of how equitable the health care system is. While accounting for care needs is beyond the scope of this study and not possible with the data used here, we acknowledge these as alternative interpretations. Third, better understanding of health care use and its trajectory among the immigrant population may serve as an important tool in developing further the models used to predict the future health expenditures at the population level. Fourth, if an increasing proportion of the population will consist of immigrants, understanding their service use is necessary for developing a culturally competent and accessible system.
We compare use of health care of immigrants to natives in Finland using data for the years 2008–2017 and a rich set of Finnish register data. Our data includes the full population of Finland and for almost every individual, information on the country of origin and the date when the person moved to Finland (or more precisely acquired a home municipality in Finland). The data also includes comprehensive individual-level information on health care utilization, demographics, and socioeconomic background. Information on socioeconomic background includes income, labour market status, marital status, and family members. We are then able to build on the previous literature by having much more detailed information on health care use over time and rich set of background variables, for the entire immigrant cohort that arrived in Finland between 2008–2010.
Our most important contribution to the literature is that we follow health care use of immigrants for several years after moving to Finland to see if it converges to that of natives. Comparing mean health care use of immigrants to the native-born answers if, on average, immigrants use services as much as the native population. While analysing average differences is important, for many policy questions it is more relevant to know whether differences between immigrants and natives tend to persist: it could be that differences in mean health care use are driven by lower use one or two years after the move, after which immigrants’ cost levels converge to those of the natives. Such short-term differences would seem less likely to warrant further research or to require interventions to increase access to health care. We use growth curve models to analyse changes in health care use over time. Growth curves allow us to flexibly characterize the development of health care use after migration to Finland and to compare the curves between immigrants and native-born Finns.
We also analyse how the trajectory of health care use depends on integration in other areas. “Integration in other areas” refers to proxies of local social capital, namely having a Finnish spouse, a workplace with dominantly native-born co-workers and neighbourhood’s ethnic composition, and socioeconomic status (employment and income status). These can be expected to provide the forms of social, cultural, and economic capital that are needed to navigate the health care system. Finally, we extend the analyses to immigrant cohorts that have arrived in Finland earlier to see whether there is a pattern of convergence when immigrants have lived in Finland for much longer.
Literature and theoretical background
2
Health care use by immigrants and demand and supply of health care
2.1
Health and health care use are affected by various sociocultural, socioeconomic, and demographic factors both in the immigrant and native populations. Andersen’s conceptual framework conceives the use of health care as a function of predisposing, enabling, and need factors (Andersen and Newman, 1973). The predisposing factors include sociodemographic variables, such as age and gender, educational level, and income, that are associated with health care needs and morbidity. Need factors include health status and how it is perceived by the individual and medical professionals. Enabling factors include not only economic resources that allow access to services but also information on the available services and other factors associated with accessibility and availability of services. Enabling factors then include factors that in the economics literature would be called supply-factors, such as the number of local service providers and the distance to them. Enabling factors also include some demand-factors, such as income, but most demand-factors would be predisposing and need variables. Immigrants may use less health care for reasons related to both supply and demand of services.
The healthy immigrant effect (HIE) is a widely studied phenomenon in the literature on immigrant health. According to the healthy immigrant effect, lower health care use by immigrants is driven by selection: those in better health tend to have a higher propensity to migrate and stay in the destination country. If this is the case, some, or all of the observed difference in average health care use is the result of differences in health. However, the evidence is mixed. The theory suggests that immigrants tend to have better health outcomes compared to the native population, particularly in the early period after their arrival in a new country. This effect has been supported by evidence from various countries (e.g., Kennedy et al., 2015; Helgesson et al., 2019; Holz, 2022; Ichou and Wallace, 2019). A recent study by Kemppainen et al. (2024) argued that immigrants in Finland have a mortality advantage also among those aged 70 years and older, but the study did not follow individuals over time to see whether there is any convergence or what is often called “acculturation” in terms of health (Hagos and Hamilton, 2024).
While evidence in support of the theory is abundant, some studies have found contrasting results, indicating that immigrants’ health may be poorer than that of the native population, particularly in European contexts (see e.g., Iglesias et al., 2003; Solé-Auró and Crimmins, 2008). Additionally, the validity of the HIE may vary depending on the origin of the immigrants. For instance, Helgesson et al. (2019) observed evidence of the HIE among Western immigrants but not among non-Western immigrants. Conversely, Kennedy et al. (2015) found that the HIE is stronger for immigrants from developing countries than for those from developed countries. It is questionable to what extent HIE can explain health care use for the heterogeneous immigrant group as a whole; therefore, a more intricate analysis is necessary both for testing the hypothesis as well as for any solid policy implications (see also Domínguez-Rodríguez and González-Rábago, 2024).
Other potential demand-side factors affecting health care use include economic resources that vary greatly between immigrants and natives also long after arrival to the host country (see Vaalavuo and Rask, 2024, on earnings trajectories of immigrants in Finland). Income may affect service use especially if there are high monetary costs for accessing care; this is not really the case in Finland where user fees in public health care were moderate in the study period, while unmet needs due to economic burden have also been reported (e.g., Aaltonen and Vaalavuo, 2024). Preferences of care intensity refer to the attitudes and information concerning the benefits and inconveniences of health care interventions. Information may also include the simple knowledge of what kind of services are available and what individuals are entitled to receive. Knowledge on the service system, health literacy, experiences of racism and discrimination, and trust in the health care system and professionals could be especially important demand-side factors for individuals with a foreign background, while also stigma related to service use could also explain differences in health care use among some immigrant groups and natives. While a number of studies report an association between experiences or anticipation of discrimination with seeking or foregoing health services (Rivenbark and Ichou, 2020), some studies have, in contrast, found an increase in health service use or no associations (Gazard et al., 2018; Dehkordy et al., 2016).
Data on preferences, health literacy, discrimination, or knowledge is not available in registers, but variables like having a Finnish spouse or living in a neighbourhood / working in a workplace with a majority of natives can be used as proxies for the information set of the individual. In general, we expect that integration in other aspects is related to health care use of immigrants being more similar to the native levels – a hypothesis that we test in this article.
Fig. 1 illustrates the conceptual framework of our study, focusing on the potential factors affecting health care use and costs among immigrants and linking the above-mentioned factors to the integration process. We will not empirically test the different causal pathways outlined in this figure, but the figure aims to capture the relations between various factors and integration as well as potential health selection in other integration outcomes.Fig. 1. Conceptual framework of the study.Note: The dashed lines in the boxes on need factors and health status indicate that we do not have information on these in our data.Fig 1
The Finnish context
2.2
In Finland, health care is largely publicly financed, organized, and produced. Primary care and specialized medicine are mostly organized and produced by local authorities, but public health care is complemented with an occupational health care system and private care. Occupational health care and private care consist mostly of ambulatory primary care but may give referrals to public specialized medicine. All residents are entitled to use public care, but access to occupational health care depends on being employed and services covered differ between employers. Occupational health care is mainly produced by private firms and is paid for by payroll deductions from employers and employees. There is a National Health Insurance system that partly reimburses the use of private care, but the subsidies are small, and access is therefore largely determined by the ability to pay. Outpatient drugs are not provided by local authorities and are instead reimbursed by the National Health Insurance. Unfortunately, for our study period there is no comprehensive register data available for use of public primary care, occupational health care and private health care. Because of this, we focus on specialized care which is almost completely produced by the public sector. In Finland, the specialized care amount to around two-thirds of all public health care costs. During the study period, the local authorities financed health care by a combination of local taxation, funding from the state and relatively low user fees with an annual ceiling. Because of autonomy and the differences in ability to raise taxes, there are geographical differences in supply. These are partly taken into account by including information on the region of residence in the models.
Data and methods
3
Data and analysis sample
3.1
We utilize various linked Finnish register data sources. The data combine rich background information on the total population of Finland from Statistics Finland and information on health care use and costs from the Finnish Institute for Health and Welfare (THL). The data are put together by the INVEST Flagship Research Centre.1 The data include the total population residing permanently in Finland. A 10 per cent random sample of Finns was drawn for the analyses for analytical feasibility, while the immigrant population includes all immigrants who arrived in Finland between 2008–2010. For additional analyses on cohort differences, we also included immigrants who have arrived earlier. We restrict the analysis sample to population aged 18–64 and those who are observed in the data for the total 7-years observation period (2011–2017). These criteria leave us with a sample of 296,956 individuals, and 2,078,692 observations in the pooled data 2011–2017. Because all analyses are conducted separately for Finnish-born and immigrant groups, the differing sampling fractions do not bias the within-group estimates. The Finnish subsample is random and therefore representative of that population, while the immigrant group is exhaustive. For this reason, and because our models control for demographic and socioeconomic characteristics (e.g., age, sex, and socioeconomic status) that would typically underlie sampling weights, we do not apply weighting in the analyses.
Of all the immigrants aged 18–64 who arrived in Finland 2008–2010, around 67 per cent remain in Finland in 2017 and are included in the analyses. On average, those who are included in the analytical sample are younger than those who leave Finland before the end of the follow-up and have slightly higher health care costs at the baseline when they come from other Eastern Europe, Asia, Africa and Middle East, but lower costs when they come from Western countries, Russia and Estonia. It is important to note that our results consider a group of immigrants that have become longer-term residents in the country, which makes sense when we are studying health care as an aspect of integration.
Variables
3.2
Our outcome variable is health care use and health care costs. The information on health care visits is derived from the Finnish Care Register for Health Care (HILMO), which includes inpatient care from both public and private providers, as well as specialized outpatient care exclusively from public providers. The cost information for psychiatry services is estimated based on the cost information reported by the hospitals, while for other services, the health care classification system (DRG) is used to productizing and pricing. The cost data has been adjusted to reflect the value of money in the year 2020. The complete cost data is available only for years 2011–2017, which limits our observation period to these years. Using costs as the outcome provides a unified metric that captures both the volume and intensity of health care use across different types of services. This measure aggregates expenditures from inpatient and outpatient care, specialist and psychiatric services, and expensive medications consumed in the hospital as part of the treatment. By using total costs rather than simple counts of visits or hospitalizations, we account for the heterogeneity in service intensity, treatment duration, and resource use. In addition to total health care costs, we estimate models with a binary outcome indicating any use of health care services and health care costs among those who have used services. This distinction allows us to separate differences in the likelihood of using any services (extensive margin) from differences in the amount or intensity of care among those who use services (intensive margin), clarifying whether observed cost differences reflect variation in access to care or in the level and type of services utilized.
Our principal independent variable is immigrant status. Immigrants are classified into eight groups by their country of birth as follows: 1) Western countries (including Western Europe together with USA, Canada, Australia and New Zealand), 2) Russia / former USSR, 3) Estonia, 4) other Eastern European countries, 5) Middle East, 6) Asia, 7) Africa, 8) other or unknown (not included in growth curve models). Individuals born in Finland or individuals born abroad to Finnish-born parents are categorised as native-born Finns.
Control variables included in the models are gender, age as a continuous variable, region of residence, labour market status (employed or not), annual taxable income of the individual as a continuous variable (in Euros), and the number of children below the age of 18 in the household. We control for age in every model, as individuals get older over the period, and older people are known to generally use more health care.
These background characteristics are presented in Table 1. There are some differences between immigrant groups and the native Finns. The native-born Finns are on average older, close to 42 years, while immigrants from Middle East and Africa are on average around 33 years old. The Finns and immigrants from Western countries have significantly higher income level, and native Finns and Estonians are more likely to be employed. More than a third of Estonians and Africans were never in a partnership during the observation period, while a majority of Western immigrants was in a partnership with a native-born Finn (67 %). In other immigrant groups, the share was significantly lower.Table 1. Basic statistics (pooled data 2011–2017).Table 1. Number of observationsShare of womenMean ageStd.dev. ageMean number of childrenStd.dev. number of childrenMean personal income (EUR)Std.dev. personal income (EUR)Share employedShare with non-Finnish partnerShare with Finnish partnerShare no partnerFinnish1 834 69349 %41.712.20.671.0532 27121 78176 %2 %62 %37 %Western countries19 51632 %36.18.50.630.9630 10025 59756 %11 %54 %35 %Russia/USSR37 87761 %38.410.60.710.9418 75415 56247 %53 %14 %32 %Estonia38 96251 %39.510.40.590.9325 23416 03868 %40 %7 %53 %Other Eastern Europe22 25346 %35.48.70.791.0122 20615 50656 %51 %15 %35 %Middle East33 15930 %32.88.30.801.1414 00812 58934 %41 %12 %47 %Asia47 07557 %34.08.00.590.8918 88615 49951 %35 %27 %38 %Africa26 50939 %32.78.30.961.4114 83810 41939 %29 %11 %60 %Other/unknown10 38842 %36.38.70.620.9022 21816 52058 %25 %34 %41 %*All immigrants235 73947 %35.79.40.701.0420 01916 389**51 %**38 %**19 %*43 %
Moderating variables on other aspects of integration
3.3
We further study the role of other aspects of integration in health care use. We use different proxies for socio-cultural integration, namely partnership with a native-born Finn, living in a neighbourhood with dominantly native population, and working in a workplace with dominantly native-born co-workers. As for economic integration, we examine the role of employment and income as moderating factors between immigrant status and health care use. It should be noted that these factors – being married in general, being employed, and having higher income – are generally associated with lower health care costs in the native population. Therefore, while they are good proxies for integration, they are also likely to be associated with even lower costs among the immigrants too. Consequently, the comparison group should be native-born Finns in the same sociodemographic or socioeconomic category.
Individuals are categorised into three groups based on partnership status: 1) has a non-Finnish partner (at any point during the observation period), 2) has a Finnish partner (at any point during the observation period), 3) has never been in a partnership during the observation period. If the person is registered to have both a Finnish origin and a non-Finnish origin partner at some point during the observation period, the person is categorised in group 2. Partnerships include both marriages and cohabitation.
Employment status is based on the status at the end of the year and is categorised either as being employed or not. Individuals are grouped into two groups based on equivalised disposable household income: those whose income is below the native-Finn median and those whose income is equal or above the median. Median is calculated from the sample’s native-born Finns separately for each year. Neighbourhood (at a post code level) and workplace characteristics refer to living and working in a place with <75 per cent of native-born Finns.
Methods
3.4
Growth curve models are appropriate for modeling trajectories over time and across different groups as they capture initial variation in health care use and trajectory over time within individuals (e.g., Jackson, 2015). In our models, time (t) refers to calendar years 2011–2017 when outcomes are measured. We estimate linear models with random intercept and random slope by immigrant group. Preliminary tests comparing linear and quadratic time specifications using likelihood-ratio tests indicated that the linear growth model provided a better fit to the data; therefore, all analyses were conducted using a linear time specification.
In addition, we run separate models by partnership status, employment status, and income level to investigate the role of cultural and economic capital as well as separate models by region of origin. We interpret group differences in health care use trajectories based on average marginal effects derived from the growth curve models. Because the main group coefficient represents only the difference at the baseline year (2011), we rely on predicted values over time to illustrate how trajectories evolve. Marginal predictions were estimated using Stata’s margins command, averaging over the observed covariate distributions. Figures display these predicted values and demonstrate changes in the gap between groups over time. Our assessment of convergence towards the native level relies on looking at the marginal effects in the figures and detecting whether the gap between immigrant groups and natives diminish over time. This takes into account any changes in the background factors that affect health care use.
Our main outcome variable is annual health care costs for individual i in year t. To estimate the linear effect of time, we specify:
where and represent individual-specific intercepts and slopes and is person-year error term. The model allows trajectories to vary as a function of individual covariates, for example:
We are especially interested in estimating random slopes by country of origin (and other aspects of integration) as specified in:
where are dummies for immigrant groups. is the baseline for the group and gives the difference in slope (or trend over time) relative to the reference group (native Finns).
We use this same model specification to estimate health care use, defined as a binary variable of any costs during the year. The binary outcome is modelled using a linear probability model.
Results
4
Descriptive evidence on costs by category
4.1
Based on Table 2 (averages by cost category), we see that native Finns have annual total costs of around 925 Euros, around double compared to immigrants from Western countries or Asia. Costs among immigrants from Middle East and Africa are close to the Finnish average. We also see remarkable differences across cost categories: it is especially psychiatric costs that are higher among the native Finns. In the following, we only focus on total health care costs or use.Table 2. Average annual costs (and standard deviations) in euros by service categories (pooled data 2011–2017).Table 2. All costs, meanAll costs, sdt.dev.Psychiatric costs, meanPsychiatric costs, std.dev.Somatic costs, meanSomatic costs, std.dev.Fertility-related costs, meanFertility-related costs, std.dev.In-patient costs, meanIn-patient costs, std.dev.Out-patient costs, meanOut-patient costs, std.dev.ER costs, meanER costs, std.dev.Finnish925481820332487223447797254534132472180362279Western countries45020377410953761644865831811416269103640162Russia/USSR51526883388848125151548252482153267112846173Estonia5252620551149470229488562254214627196648191Other Eastern Europe54922403868351121061588232411558308119062219Middle East8475048129278571841121558794284547419144291266Asia4542307347814202149165837240194521483240164Africa8843913952101788327327912514693233414161285244Other/unknown5171831577124591638128815211130830593758213All immigrants590310762149052826781538432902612301116157205
Results based on growth curve models
4.2
We move on to results where we control for important background factors associated with health care use. Fig. 2 illustrates probability for using any specialised health care during the year controlling for age and gender (left panel) and additionally controlling for employment, personal annual income, number of children in the household, and region of residence. Fig. 3 illustrates similarly the estimated annual total costs in Euros. There appears to be modest convergence when overall use is the outcome, while no convergence in costs. Adding more control variables in the model affects the group trajectories or ordering of countries, but not convergence. The native-immigrant difference appears statistically significant in almost all immigrant groups and the confidence intervals are narrow in all groups.Fig. 2. Health care use by country of origin.Note: Model A controls for age and gender. Model B controls for age, gender, region of residence, employment, annual taxable income, and number of children in the household. Y-axis denotes the probability of having any health care costs, i.e., use of health care. Full models are presented in Appendix Table A1.Fig 2. Fig. 3Total health care costs by country of origin.Note: Model A controls for age and gender. Model B controls for age, gender, region of residence, employment, annual taxable income, and number of children in the household. Costs are deflated to the price level of 2020. Full models are presented in Appendix Table A1.Fig 3
The differences between immigrants arriving in Finland between years 2008 and 2010 and natives are large in 2011 and remain so through the follow-up period, with most immigrant groups using significantly less health care. Interestingly, immigrants from Africa and Middle East seem to have used more health care in 2011 than natives, but their average health care use drops over the years. Their higher costs are partly explained by background characteristics as this is not visible in model B of Fig. 3. Also, while their probability of use remains slightly higher than among natives (Fig. 2), their costs in 2017 are significantly below that of natives (Fig. 3). If there is any convergence in costs, it regards to immigrants from Western countries with steeper than average increase in both use and costs. In Fig. 4, we further look at costs among those with any use. This shows that native-immigrant gap is considerable also among those who use services (with wider and partly overlapping confidence intervals in Model A), and convergence mainly happens between immigrants from Western countries and Estonia and native Finns.Fig. 4. Total health care costs of those with any use.Note: Model A controls for age and gender. Model B controls for age, gender, region of residence, employment, annual taxable income, and number of children in the household. Costs are deflated to the price level of 2020. Full models are presented in Appendix Table A2.Fig 4
Fig. 5 additionally shows results of model B separately for men and women. While the results regarding men follow the overall pattern in Fig. 3, among women there are more diverse patterns to be seen (however, with wider and partly overlapping confidence intervals): convergence in costs among Western immigrants, but divergence regarding women from Middle East. As in the native population, the costs among women are higher than among men.Fig. 5. Total health care costs by country of origin, separately for men and women.Note: Model controls for age, region of residence, employment, annual taxable income, and number of children in the household (as in Model B in Fig. 2). Costs are deflated to the price level of 2020. Full models are presented in Appendix Table A2.Fig 5
Fig. 6 graphs health care costs by partnership status. In Appendix Fig. A1, graphs can also be found in separate plots by country of origin to compare the role of partnership status within groups. For natives, health care use is higher for those with no partner. The health premium of marriage (or health selection into marriage) is well documented in the literature (e.g., Dupre et al., 2009; Lawrence et al., 2019), and these results seem to confirm this for health care costs as well. The results differ between the immigrant groups and are not easily summed. Also, overlapping confidence intervals illustrate that not all groups are statistically different from natives. Whether the partner is Finnish or non-Finnish does not seem to matter in all groups, and among Estonian, Russian, and other Eastern European immigrants, those with a Finnish partner, have the highest costs and not those without a partner like in other groups at the end of the observation period. For Africans, we see health care use decreasing for those with non-Finnish partner, while it increases slightly for those with Finnish partner. What is curious is that for Western and Middle East immigrants, health care use grows strongly over the period for those with no partner, compared to those with partner. These results might reflect selection into partnership with natives or in general as discussed by Vaalavuo and Rask (2024). Therefore, rather than being a proxy of integration, a Finnish partner (or any partner, for that matter) might reflect health selection into partnership, which is stronger among some groups than others. All in all, there seems to be no convergence in costs when partner is a native Finn, against our hypothesis.Fig. 6. Health care costs by partnership status.Note: Model controls for age, gender, region of residence, employment, annual taxable income, and number of children in the household. Models have been run separately by partnership status. Costs are deflated to the price level of 2020. Full models are presented in Appendix Table A3. Note that y-axis scale is different for the group “never partner”.Fig 6
In Fig. 7, employed and non-employed are compared. In Appendix Fig. A2, the results are plotted by country. In these figures we see a more systematic pattern that in every group non-employed have higher costs than employed. However, as with native-Finns, the costs of employed seem to grow slightly more over time in most groups, especially among African immigrants, while the opposite is true for Western immigrants. Foreign-born employed are generally closer to the cost level of the natives and there are only modest differences in costs. This would partly support our expectation that integration in one area is associated with smaller native-immigrant gap in health care costs.Fig. 7. Health care costs by employment status.Note: Model controls for age, gender, region of residence, annual taxable income, and number of children in the household. Models have been run separately by employment status. Costs are deflated to the price level of 2020. Full models are presented in Appendix Table A4. Note that y-axis scales are different.Fig 7
Similarly, results by relative income level are presented in Fig. 8 and separately by country in Appendix Fig. A4. Again, the common pattern is that those with lower income (below median income) have higher costs. Fig. 8 also illustrates that there seems to be rather divergence than convergence in costs when those with income above the median are analysed. However, as with employment, the native-immigrant gaps in costs are smaller among those having above median income. In other words, if we do not consider convergence over time, we might also conclude that economic integration is definitely associated with smaller gaps in health care use.Fig. 8. Total health care costs by relative income level, separately by country of origin.Note: Relative income status refers to income lower than the median of native-born Finns in the sample and the year in question and equal or higher than the median. model controls for age, gender, region of residence, employment, and number of children in the household. models have been run separately by income status. Costs are deflated to the price level of 2020. Full models are presented in Appendix Table A5.Fig 8
In Table 3 only immigrants are included in the analyses because very few native Finns work or live in places with <75 per cent of native-born Finns (see Appendix Table A6). In addition, the workplace information is naturally only available for employed immigrants. For comparison, we also include results on neighbourhood characteristics for those employed. The results show that neighbourhood characteristics – as we have defined them – are not statistically significantly associated with health care costs. However, working in a workplace with a lower native share seems to be associated with lower costs supporting our expectation. However, it is also possible that this workplace characteristic is associated with unobserved characteristics of immigrants, a result of non-random selection into such workplaces.Table 3. Results from growth curve models with neighborhood and workplace characteristics.Table 3. Workplace, only employed immigrantsNeighborhood, all immigrantsNeighborhood, only employed immigrantsTime26.12235.759^⁎⁎^23.623(11.054)(13.686)(11.988)Immigrant group (ref. Western immigrants)Russia/USSR−76.637−160.105*−85.828(59.218)(77.110)(68.691)Estonia−61.923−75.850−77.372(54.513)(76.525)(63.608)Other Eastern Europe−25.786−16.165−46.193(62.476)(84.584)(72.838)Middle East154.390394.680^⁎⁎⁎^167.062(67.160)(78.612)(77.447)Asia−33.413−9.836−6.373(55.790)(75.089)(64.769)Africa124.295421.205^⁎⁎⁎^115.177(66.423)(81.664)(77.490)Other/unknown15.128−29.79312.759(75.917)(103.144)(88.533)Age1.4483.609^⁎⁎^1.622(0.898)(1.103)(0.957)Female321.801^⁎⁎⁎^410.762^⁎⁎⁎^337.159^⁎⁎⁎^(16.299)(20.729)(17.232)Number of children89.852^⁎⁎⁎^117.931^⁎⁎⁎^96.134^⁎⁎⁎^(8.221)(8.599)(8.579)Personal annual income−0.001*−0.001−0.000(0.000)(0.001)(0.000)Native share at workplace <75 %−49.908^⁎⁎⁎^(14.750)Employed−237.345^⁎⁎⁎^(18.221)Native share in neighborhood <75 %14.15410.224(31.599)(30.492)Constant129.138*220.338^⁎⁎^78.338(56.566)(75.421)(63.522)Observations115,972202,885**116,055Note: Region of residence and interaction between time and country of origin are also controlled for, but not shown, as we are mainly interested in the coefficient for “native share”. Standard errors in parentheses, * p < 0.05, ^⁎⁎^p < 0.01, ^⁎⁎⁎^p < 0.001.
Finally, we extend the analysis to immigrant cohorts that have arrived in Finland since the 1980s. This is to see whether a much longer residence in Finland affects the results and whether we can (finally) observe patterns of convergence in costs. This indeed seems to be the case as earlier arrived immigrants have higher costs than more recent immigrant cohorts (Fig. 9). We can observe that each subsequent cohort has smaller costs. However, it should be highlighted that immigrant cohorts that have arrived in the early 1980s differ from the most recent cohorts in many ways, also in terms of country of origin, age at migration, and reason for migration. Also, we do not observe their health care costs immediately after arrival, so we do not know whether they have started with similar health costs relative to natives as the cohort of 2008–2010 immigrants under focus in the above analyses.Fig. 9. Health care costs by immigrant cohort.Note: Model controls for age, gender, region of residence, employment, personal taxable income, and number of children in the household. costs are deflated to the price level of 2020. full models are presented in Appendix Table A6. As country of origin is not known for all immigrants who have arrived in the 1980s, we do not control it in the model.Fig 9
Conclusions
5
In this article we examined the health care use and costs among a cohort of recently arrived working-age immigrants in Finland and studied whether their costs converge to the native levels over a 7-year observation period. The study contributes to the literature on the healthy immigrant effect, ethnic health and service-use disparities, and implications of rising immigration for national and regional health care costs. We approached the convergence of health care costs between immigrants and natives as a potential indicator of integration within the health care system, expecting to see convergence in costs over time and especially along other dimensions of integration. We studied both proxies for cultural and social integration as well as economic integration. This evidence in a novel contribution to the prior literature.
The results are important as differences in population structure affect regional health disparities and the need for health care services. Immigration is likely to increasingly affect the population structure in Finland, and therefore also the health care needs across regions. Immigrants are on average younger than native population and tend to live in urban areas. However, immigrants too get older and need more health care as they age. While the healthy immigrant thesis expects lower costs and use among immigrants, the acculturation thesis expects the health status of immigrants to converge to native level over time. The acculturation thesis attributes immigrants’ initial health advantage to healthier life styles (Hagos and Hamilton, 2024). However, we argue that lower initial costs may also reflect unmet needs arising from, for example, limited knowledge about available services. Therefore, integration in other areas of life would promote more equal use of services and thereby convergence in costs over time. As we note, there might be health-related selection in other dimensions of integration, for example in being employed or having a native partner, therefore we need to be prudent in drawing causal inferences and rather illustrate the various interrelationships between these factors.
We found that health care costs are lower among immigrants compared to natives even (or especially) when controlling for various background characteristics. There also appears to be almost no convergence over time. However, differences between immigrant groups and cost categories are clearly visible, but quite systematically only immigrants from Western countries seem to slightly approach the cost level of native Finns. We also noted that other dimensions of immigrant integration (having a native partner, neighborhood and workplace characteristics, and socioeconomic status) have some role in moderating the association between immigrant background and health care costs.
The native-immigrant cost gap was smaller and sometimes differences were not statistically significant when we analyzed different groups that can be considered more culturally or economically integrated. Moreover, these factors – such as having a partner and higher income – appeared to affect costs the same way among natives and immigrants in most cases. The smallest gap in costs appeared among employed immigrants and natives. Therefore, economic integration was indeed strongly associated with smaller differences in costs between any immigrant group and natives. The results could also indicate that there is positive health selection to having higher income, being employed, and having a Finnish partner. Such non-random selection regarding unobserved characteristics makes it difficult to analyze the connection between integration and health service use, but the results might suggest which groups should be targeted to improve access to health care. We found remarkable variation in health care costs when looking beyond the averages and even within immigrant groups from same regions. The variation in the results demonstrate that the healthy immigrant effect is an oversimplification of the reality. On the other hand, our results together with the results found by Kemppainen et al. (2024) concerning lower mortality risk for older migrants, could indicate that migrants tend to be healthier on average and that convergence may take more time as suggested by the results on earlier immigrant cohorts.
While the analyses are based on rich register data, we were not able to account for all factors affecting health care need. Therefore, there is causal ambiguity in the findings, and we are currently not able to say whether the findings indicate unequal access, unmet needs, efficiency of care or better health status among most immigrant groups. This also makes it challenging to interpret potential convergence as integration, and other data sources, including survey data, might be necessary to complete the analysis of health care use as an aspect of immigrant integration. Future research should link administrative cost data with diagnostic, morbidity, and mortality data, as well as survey data on perceived needs, barrier in access and perceptions of quality of services to clarify whether observed cost differences stem from differences in health needs, access, or efficiency of care. Previous evidence suggests that immigrants face considerable obstacles in accessing health care and suffer from unmet health care needs also in Finland (Kuusio et al., 2023). However, when we look at immigrants who have a Finnish partner, we would assume that they would get the relevant information on accessing the services they need, which might indicate that at least those immigrants with a native partner might indeed be in better health than the natives. Further studies should explore whether the gender of the Finnish partner may have an influence, as it may be that native Finnish women are more informed of the Finnish health care system than native Finnish men. Additionally, further studies should explore the sector of employment and reasons for migration, as it is possible that the persons in this group are highly skilled international migrants and may be therefore more likely to be selected with better health.
The finding on the cost differences among service users could also indicate that immigrants do not need as intensive and expensive care as the native Finns. However, this result could also indicate that even when immigrants access services, they do not get equal care compared with natives. Culturally competent health systems should be developed in increasingly diverse societies, while effectiveness of tools to this end should be improved (Anderson et al., 2003). These are questions that need to be tackled in future research with a more focused research design suitable for disentangling such questions. Despite these limitations, the use of register data is promising and has many advantages. For example, prior evidence has demonstrated that immigrants report more health care visits in surveys than is observable in administrative data (García-Velázquez et al., 2022). Disparity between register and self-reported data is likely to be at least partially attributable to regional differences in how complete the administrative health register data is in some regions. Further studies should consider using multisource data to get a more complete overview of the use of services, and background factors associated with service use. The current study used data up to 2017, which is the time prior to Covid-19 pandemic. Further studies should explore whether the need for care and health care costs have changed after the pandemic.
In the future research on the topic, it would be important to analyze outcomes of health care use in different immigrant groups, and the social and economic consequences of ill health among immigrants. Some evidence already suggests that outcomes are worse among immigrants, for example cancer mortality among immigrant children is significantly higher than among native children (Kyrönlahti et al., 2020). Also, as was suggested by descriptive evidence of our data, a considerable difference in costs exists across health care sectors – a topic that should be investigated further. A few concrete implications for health care providers could be highlighted. First, regional service providers should disaggregate data on service use by region of origin in order to identify groups with high and low health care use, and to determine the underlying mechanisms. Lower use of health care does not necessarily equate to better health. Second, if lower health care use is found to be related to unmet health needs, emphasis should be placed on inclusive and accessible communication, culturally appropriate care, and addressing implicit bias among the health care professionals.
CRediT authorship contribution statement
Maria Vaalavuo: Writing – original draft, Supervision, Project administration, Methodology, Funding acquisition, Formal analysis, Data curation, Conceptualization. Tuukka Holster: Writing – original draft, Conceptualization. Natalia Skogberg: Writing – original draft, Conceptualization. Heidi Kuusinen: Writing – original draft, Data curation.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Aaltonen K.Vaalavuo M.Financial burden of medicines in five Northern European countries: a decommodification perspective Soc. Sci. Med.347202411679910.1016/j.socscimed.2024.11679938518482 · doi ↗ · pubmed ↗
- 2Akhtar S.S.Heydon S.Norris P.Access to healthcare system: experiences and perspectives of Pakistani immigrant mothers in New Zealand J. Migr. Health 202210007710.1016/j.jmh.2021.100077 PMC 872494535024677 · doi ↗ · pubmed ↗
- 3Andersen R.Newman J.F.Societal and individual determinants of medical care utilization in the United States Milbank Meml. Fund. Q Health Soc.5111973951244198894 · pubmed ↗
- 4Anderson L.M.Scrimshaw S.C.Fullilove M.T.Fielding J.E.Normand J.Culturally competent healthcare systems: a systematic review Am. J. Prev. Med.2432003 Supplement 10.1016/s 0749-3797(02)00657-812668199 · doi ↗ · pubmed ↗
- 5Arsenijevic J.Seibel V.Do immigrants know less than natives about cancer screening tests? The case of Netherlands J. Migr. Health 202410025810.1016/j.jmh.2024.100258 PMC 1136382139220098 · doi ↗ · pubmed ↗
- 6Barlow P.Mohan G.Nolan A.Utilisation of healthcare by immigrant adults relative to the host population: evidence from Ireland J. Migr. Health 5202210007610.1016/j.jmh.2021.100076 PMC 871532835005673 · doi ↗ · pubmed ↗
- 7Çilenti K.Rask S.Elovainio M.Lilja E.Kuusio H.Koskinen S.Koponen P.Castaneda A.E.Use of health services and unmet need among adults of Russian, Somali and Kurdish origin in Finland Int. J. Env. Res. Public Health 185202122293366824110.3390/ijerph 18052229 PMC 7956472 · doi ↗ · pubmed ↗
- 8Dehkordy S.F.Hall K.S.Dalton V.K.Carlos R.C.The link between everyday discrimination, healthcare utilization, and health status among a national sample of women J. Women's Health 251020161044105110.1089/jwh.2015.5522 PMC 506972527429363 · doi ↗ · pubmed ↗