Efficacy and Safety of Folisurge, a Biosimilar Recombinant Follicle-Stimulating Hormone, Versus Gonal-F in Assisted Reproductive Technology Practice in India: A Real-World Study
Shashank Sanagoudar, Vipin Chandra, Shipra Nigam, Anjali Gahalan, Ritu Punhani, Nihita Pandey, Sara Zaidi, Jyoti Panday, Nihar Ranjan Bhoi, Walmik Mistari, Isha Suwalka, Nitasha Gupta

TL;DR
This study compares the effectiveness and safety of Folisurge and Gonal-f in fertility treatments in India, finding similar safety but better outcomes with Folisurge.
Contribution
A real-world comparison of a biosimilar follicle-stimulating hormone (Folisurge) versus an innovator drug (Gonal-f) in ART practice in India.
Findings
Folisurge yielded significantly more oocytes and embryos compared to Gonal-f.
Baseline antral follicle count was higher in the Folisurge group.
Serum β-hCG positive rate was similar between the two groups.
Abstract
Objective: This study was conducted to compare the efficacy and safety of Folisurge, a biosimilar recombinant follicle-stimulating hormone (r-FSH), with Gonal-f, an innovator r-FSH, in patients undergoing assisted reproductive technology (ART). Methods: In this non-interventional, investigator-initiated, real-world, retrospective study, females aged 21-40 years with a body mass index (BMI) ranging between 17 and 34.9 kg/m2, with serum anti-Müllerian hormone (AMH) more than 1.2 ng/mL, undergoing controlled ovarian stimulation (COS), and those having received Folisurge or Gonal-f were included. The primary outcome was the mean number of metaphase II (MII) oocytes retrieved in each group. Secondary outcomes included the mean number of embryos formed and serum β-human chorionic gonadotropin (β-hCG) positive rate in each group. Results: A total of 3090 women were included, out of which…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
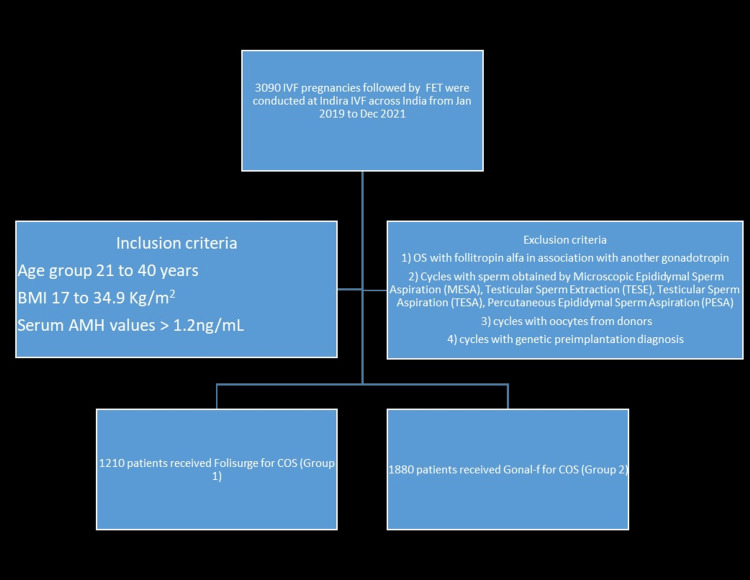 Figure 1
Figure 1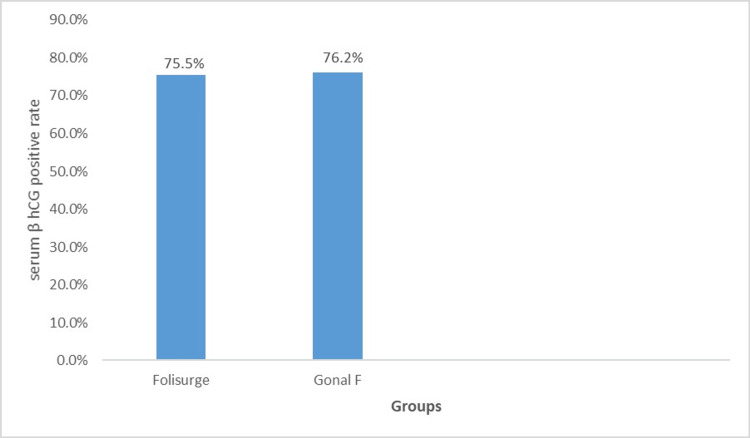 Figure 2
Figure 2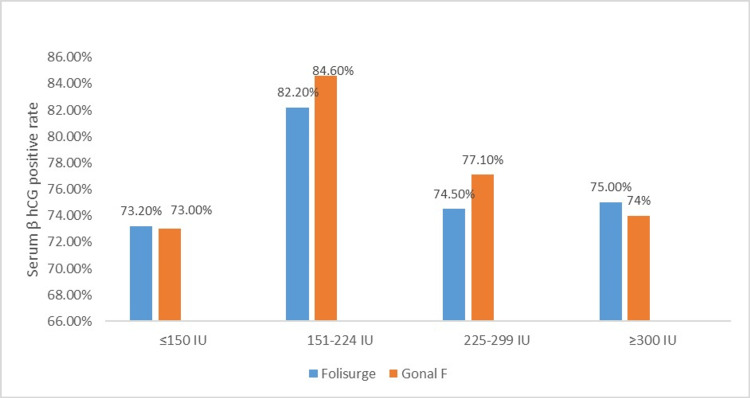 Figure 3
Figure 3| Overall (n = 3090) | Folisurge group (n = 1210) | Gonal-f group (n = 1880) | ||
| Characteristics | p-value | |||
| Age in years, mean (SD) | 29.6 (3.9) | 29.1 (3.6) | 29.9 (4.0) | 0.452 |
| BMI in kg/m2, mean (SD) | 24.7 (3.9) | 24.8 (3.9) | 24.6 (3.9) | 0.501 |
| Markers of ovarian reserve | ||||
| Serum AMH in ng/mL, mean (SD) | 4.5 (2.4) | 4.8 (2.4) | 4.3 (2.4) | 0.062 |
| AFC, mean (SD) | 21.8 (9.8) | 23.8 (10.1) | 20.6 (9.3) | <0.001 |
| Husband/donor's age | ||||
| Husband/donor's age in years, mean (SD) | 33.6 (4.24) | 33.4 (4.1) | 33.7 (4.3) | 0.064 |
| Semen parameters | ||||
| Sperm count in million/mL, mean (SD) | 45.6 (25.9) | 43.1 (26.9) | 47.2 (25.1) | <0.001 |
| Sperm motility (%), mean (SD) | 40.0 (20.8) | 39.0 (21.7) | 40.7 (20.1) | <0.001 |
| Normal sperm morphology (%), mean (SD) | 2.42 (1.4) | 2.13 (1.5) | 2.6 (1.4) | 0.106 |
| Folisurge (N = 1210) | Gonal-f (N = 1880) | |||||||
| Starting dose | ≤150 IU (n = 231) | 151–224 IU (n = 202) | 225-299 IU (n = 737) | ≥300 IU (n = 40) | ≤150 IU (n = 704) | 151–224 IU (n = 188) | 225-299 IU (n = 938) | ≥300 IU (n = 50) |
| Wife's age, mean (SD) | 30.8 (4.0) | 27.6 (3.3) | 29.0 (3.4) | 30.6 (3.6) | 31.2 (4.2) | 28.0 (3.4) | 29.3 (3.7) | 29.5 (3.4) |
| BMI, mean (SD) | 24.0 (3.9) | 23.8 (3.2) | 25.1(3.9) | 26.7 (4.3) | 24.4 (3.8) | 23.4 (3.6) | 24.9 (3.9) | 26.7 (4.4) |
| AMH, mean (SD) | 3.3 (2.3) | 7.1 (1.5) | 4.7 (2.2) | 4.3 (1.0) | 3.0 (2.0) | 7.1 (1.5) | 4.7 (2.1) | 4.2 (1.0) |
| AFC, mean (SD) | 18.0 (9.7) | 29.8 (9.4) | 24.1 (9.4) | 21.0 (10.0) | 15.0 (7.3) | 28.9 (9.1) | 23.1 (8.4) | 21.8 (7.2) |
| Husband/donor's age in years, mean (SD) | 34.3 (4.0) | 32.0 (3.9) | 33.4 (4.1) | 33.9 (3.6) | 34.6 (4.5) | 32.3 (3.9) | 33.3 (4.1) | 35.2 (4.6) |
| Sperm count (M/mL), mean (SD) | 38.6 (25.5) | 42.5 (25.3) | 44.6 (27.8) | 44.6 (24.5) | 46.9 (26.3) | 47.4 (24.5) | 47.4 (24.3) | 43.6 (26.9) |
| Sperm motility (%), mean (SD) | 35.2 (22.2) | 40.9 (22.0) | 39.6 (21.6) | 40.3 (18.6) | 40.2 (19.8) | 40.9 (20.2) | 41.1 (20.3) | 39.1 (20.8) |
| Sperm morphology (%), mean (SD) | 1.5 (1.4) | 1.8 (1.5) | 2.4 (1.5) | 2.7 (1.3) | 2.4 (1.4) | 2.7 (1.3) | 2.7 (1.4) | 2.8 (1.3) |
| Characteristics (n = 3090) | Starting dose of Folisurge (n = 1210) | Starting dose of Gonal-f (n = 1880) | ||||||
| <=150 IU | 151-224 IU | 225-299 IU | >=300 IU | <=150 IU | 151-224 IU | 225-299 IU | >=300 IU | |
| Days of stimulation, mean (SD) | 11.5 (1.4) | 11.0 (1.4) | 11.1 (1.3) | 11.6 (1.6) | 11.5 (1.3) | 11.3 (1.4) | 11.1 (1.3) | 11.3 (1.5) |
| Daily dose of r-FSH used for COS, mean (SD) | 150.0 (0.0) | 187.5 (0.0) | 229.6 (14.4) | 309.4 (25.1) | 150.0 (0.0) | 187.5 (0.0) | 228.0 (11.9) | 307.5 (22.7) |
| Total dose of r-FSH used, mean (SD) | 1718.8 (216.6) | 2065.3 (266.2) | 2538.2 (338.8) | 3579.4 (565.6) | 1731.2 (201.5) | 2116.0 (269.3) | 2533.9 (329.4) | 3454.5 (452.4) |
| Characteristics | All patients (n = 3090) | Folisurge patients (n = 1210) | Gonal-f patients (n = 1880) | P-value |
| Number of oocytes expected, mean (SD) | 15.6 (8.4) | 17.2 (9.2) | 14.5 (7.6) | <0.001 |
| Number of oocytes retrieved, mean (SD) | 16.5 (8.8) | 18.1 (9.4) | 15.5 (8.3) | <0.001 |
| Oocyte retrieval rate, mean (SD) | 114.1 (50.0) | 112.6 (48.3) | 115 (51.1) | 0.204 |
| Number of metaphase II oocytes, mean (SD) | 11.8 (7.1) | 13 (7.5) | 10.9 (6.6) | <0.001 |
| MII rate, mean (SD) | 70.5 (14.8) | 71.4 (14.5) | 69.9 (14.9) | 0.001 |
| Embryo details | ||||
| Number of embryos formed, mean (SD) | 4.8 (4.1) | 4.9 (4.1) | 4.7 (4.1) | 0.022 |
| Blastocyst rate, mean (SD) | 43.9 (28.5) | 42.3 (27.6) | 44.9 (29.0) | 0.008 |
| Good blastocyst rate, mean (SD) | 30.0 (21.8) | 28.2 (20.9) | 31.2 (22.3) | <0.001 |
| Number of embryos transferred, mean (SD) | 1.9 (0.4) | 1.9 (0.4) | 1.9 (0.4) | 0.078 |
| Key performance indicators of ovarian stimulation | ||||
| OSI, mean (SD) | 184.7 (140.9) | 176.5 (147.3) | 189.9 (136.4) | <0.001 |
| FOI, mean (SD) | 74.3 (16.3) | 74.6 (16.3) | 74.2 (16.2) | 0.408 |
| FORT, mean (SD) | 71.3 (19.1) | 72.4 (19.4) | 70.7 (18.8) | 0.004 |
| Characteristics (n = 3090) | Folisurge (n = 1210) | Gonal-f (n = 1880) | ||||||
| <=150 IU | 151-224 IU | 225-299 IU | >=300 IU | <=150 IU | 151-224 IU | 225-299 IU | >=300 IU | |
| Mean (SD) | ||||||||
| Outcomes of oocyte retrieval according to the starting dose of Folisurge or Gonal-f | ||||||||
| Oocytes expected | 13.3 (9.5) | 21.8 (9.7) | 17.3 (8.5) | 14.8 (7.8) | 10.1 (5.2) | 20.7 (8.6) | 16.5 (7.3) | 14.1 (6.1) |
| Oocytes retrieved | 13.3 (9.1) | 23.4 (9.4) | 18.2 (8.8) | 15.4 (9.0) | 11.0 (6.5) | 22.8 (8.6) | 17.3 (7.8) | 16.5 (7.1) |
| Oocyte retrieval rate | 110.2 (51.9) | 115.4 (45.4) | 112.5 (48.1) | 113.9 (45.1) | 116.2 (52.6) | 118.6 (50.1) | 112.4 (48.4) | 133.0 (75.2) |
| Number of MII oocytes | 9.9 (6.8) | 16.8 (7.5) | 13.1 (7.3) | 11.1 (7.6) | 7.8 (5.1) | 16.7 (7.5) | 12.1 (6.3) | 11.3 (5.1) |
| MII oocyte rate | 75.2 (15.6) | 72.2 (14.2) | 70.2 (13.8) | 68.5 (16.6) | 70.2 (15.4) | 72.4 (13.3) | 69.3 (14.9) | 69.3 (13.1) |
| Embryo details | ||||||||
| Embryos formed | 4.0 (3.7) | 5.7 (4.4) | 4.9 (3.9) | 6.1 (6.1) | 3.7 (3.1) | 7.7 (5.4) | 4.8 (4.2) | 4.0 (2.9) |
| Blastocyst rate | 47.5 (28.7) | 38.0 (27.3) | 41.3 (27.0) | 53.3 (27.5) | 51.0 (31.3) | 47.1 (27.5) | 40.2 (26.7) | 38.6 (28.0) |
| Good blastocyst rate | 34.8 (24.7) | 23.2 (16.9) | 27.1 (20.0) | 35.4 (22.7) | 35.7 (25.4) | 28.6 (18.8) | 28.5 (20.0) | 28.8 (19.5) |
| Number of embryos transferred | 1.8 (0.4) | 1.9 (0.3) | 1.9 (0.4) | 1.9 (0.5) | 1.8 (0.4) | 1.9 (0.4) | 1.9 (0.4) | 1.9 (0.5) |
| Key performance indicators of ovarian stimulation | ||||||||
| OSI | 215.8 (226.8) | 102.5 (42.4) | 177.7 (120.3) | 301.8 (182.0) | 218.7 (164.2) | 107.8 (50.5) | 180.8 (108.2) | 263.7 (218.9) |
| FOI | 71.4 (21.5) | 77.9 (15.0) | 74.8 (14.6) | 73.4 (15.5) | 72.6 (18.2) | 78.7 (15.2) | 74.4 (14.7) | 74.6 (15.1) |
| FORT | 71.0 (21.0) | 73.3 (19.4) | 72.6 (18.8) | 71.5 (20.6) | 68.4 (19.1) | 72.3 (19.3) | 72.3 (18.0) | 66.3 (23.0) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBiosimilars and Bioanalytical Methods · Ovarian function and disorders · Reproductive Health and Technologies
Introduction
As per the World Health Organization (WHO), in the developing nations, one in four couples suffers from infertility [1]. A study suggested that in India, about 15-20 million couples per year suffer from infertility, and approximately 25% of the world’s infertile couples belong to India [2,3]. Infertility takes an immense toll on the social, economic, and mental well-being of many couples in India.
Assisted reproductive technology (ART) has proved to be immensely beneficial to such couples with improved success rates in the current scenario. Follicle-stimulating hormone (FSH) in various formulations has been the backbone of ART cycles for controlled ovarian stimulation (COS) since the time of inception [4]. Initially, the source of FSH was the urine of menopausal women. However, the drawbacks of urine sources are batch-to-batch variability, risk of transmission of infection, and lack of consistency in results [5]. The advent of recombinant follicle-stimulating hormone (r-FSH) has revolutionized the outcome of stimulation as the oocytes respond more consistently to r-FSH and there are fewer inter-batch variations in their activity [5,6].
Gonal-f was the first recombinant follitropin-alpha (r-FSH α) manufactured by Merck Serono (Darmstadt, Germany). It was developed in 1988 but was licensed in the European Union in 1995 and received the United States Food and Drug Administration (USFDA) approval in 2004 [7]. Gonadotrophin therapy is a significant proportion of ART treatment costs, which in emerging economies like India [8] are out-of-pocket expenses for the patients [8]. Thus, the introduction of r-FSH biosimilars has the potential to reduce the treatment costs globally. This opened the doors for biosimilars, which are compounds similar in function, although not identical to the originator. Many countries have approved different biosimilars for use in ART [8-10].
Folisurge (manufactured by Intas Pharmaceuticals Ltd, Ahmedabad, India), a recombinant human follicle-stimulating hormone alpha (h-FSH-α) biosimilar, was approved by the Drugs Controller General of India (DCGI) in May 2013. However, any study with a direct comparison of Folisurge and Gonal-f in a real-world setting is not available. Hence, this real-world, non-interventional, retrospective, investigator-initiated study was conducted to compare the efficacy and safety of Folisurge versus Gonal-f in patients undergoing ART.
Materials and methods
Study design
This was a non-interventional, investigator-initiated, retrospective, real-world, observational study, conducted at Indira IVF, a private chain of ART hospitals, at multiple locations across India, from April 2019 to June 2021. The study utilized patient data extracted from the centralized hospital information system, which maintains comprehensive electronic medical records across the institution. Patient records from April 2019 to June 2021 were considered from the hospital's central data repository.
All females undergoing COS in in-vitro fertilization (IVF), followed by frozen embryo transfer (FET) cycles between the age groups of 21 and 40 years, with a body mass index (BMI) ranging between 17 and 34.9 kg/m2, and an anti-Müllerian hormone (AMH) level more than 1.2 ng/mL, were included in the study.
The research did not include data from participants undergoing the following treatments: (1) cycles with sperm obtained by microscopic epididymal sperm aspiration (MESA), testicular sperm extraction (TESE), testicular sperm aspiration (TESA), and percutaneous epididymal sperm aspiration (PESA); (2) cycles with donor oocytes; (3) cycles with genetic preimplantation diagnosis; (4) cycles with female fertility preservation; (5) ovarian stimulation with follitropin alfa in conjunction with another gonadotropin [8]. Four patient groups were examined for Folisurge and Gonal-f based on their initial r-FSH dosages: less than 150 IU, 150-224 IU, 225-299 IU, and more than 300 IU.
The study protocol and related documents were reviewed and approved by the Indira IVF Hospital Institutional Ethics Committee (Reg No: ECR/1773/Inst/PB/2023), The study was conducted in accordance with the ethical principles that have their origin in the Declaration of Helsinki and in accordance with the International Conference on Harmonization’s Good Clinical Practice (ICH-GCP) guidelines [11], New Drugs and Clinical Trial (NDCT) Rules - 2019 [12], Indian Council of Medical Research (ICMR) Guidelines for Biomedical Research (2017) [13], applicable regulatory requirements, and in compliance with the protocol. This was a retrospective study without patient identifiers; hence, the informed consent of patients was not taken.
Study assessments
The primary outcome was the mean number of metaphase II (MII) oocytes retrieved. Secondary outcomes included the mean number of embryos formed and serum β-human chorionic gonadotropin (β-hCG) positive rate in each group. Only variables consistently gathered by the various centers were used for secondary endpoints and demographic data. These variables were the number of days of r-FSH stimulation, the total dosage of r-FSH delivered, the number of oocytes retrieved, the number of MII oocytes, and the number of embryos produced.
Statistical analysis
Because the goal of this study was descriptive, no formal sample size calculations were performed; instead, the sample size was determined by assuring sufficient numbers to explain the efficacy of Folisurge in routine usage. Descriptive data are supplied with continuous data expressed as mean ± SD or, if non-normally distributed, as median [8]. All statistical analyses were carried out using SAS® version 9.4 (SAS Institute, Cary, NC). All statistical tests had to be two-sided at α = 0.05, unless otherwise noted.
Results
A total of 3090 women were studied, out of which 1210 received Folisurge, and 1880 received Gonal-f as described in the Consolidated Standards of Reporting Trials (CONSORT) diagram (Figure 1). The baseline characteristics were comparable between the two groups (Table 1). In the Folisurge group, the mean antral follicle count (AFC) was significantly higher than in the Gonal-f group (23.8 vs. 20.6, p < 0.001). The mean sperm count was significantly lower in the Folisurge group than in the Gonal-f group (43.1 million/mL vs. 47.2 million/mL, p < 0.001). Also, the mean sperm motility was significantly lower in the Folisurge group than in the Gonal-f group (39.0% vs. 40.7%, p < 0.001).
Patient enrollment flowchart.IVF: in-vitro fertilization; FET: frozen embryo transfer; AMH: anti-Müllerian hormone; OS: ovarian stimulation; COS: controlled ovarian stimulation.
In both groups, patients were administered r-FSH, and the starting dose ranged from 150 IU to 375 IU. Based on the starting dosage of r-FSH, there were no differences seen between the two groups in terms of age, BMI, and serum AMH levels (Table 2). The AFC in the Folisurge group was higher than the Gonal-f group in most of the dosage strengths used. The sperm count, motility, and morphology were lower in the Folisurge group vs. the Gonal-f group in most of the dosages studied.
The mean number of days of stimulation was similar in both groups across different starting doses (Table 3). Also, there was no major change in the starting dose and daily dose across different subgroups for both the Folisurge and Gonal-f groups. The mean (SD) number of oocytes retrieved was significantly higher in the Folisurge group vs. the Gonal-f group (8.1 (9.4) vs. 5.5 (8.3), p < 0.001) (Table 4).
The mean (SD) number of MII oocytes retrieved with Folisurge was significantly higher than Gonal-f (13 (7.5) vs. 10.9 (6.6), p < 0.001). The mean (SD) number of embryos formed was also higher in the Folisurge vs. Gonal-f group (4.9 (4.1) vs. 4.7 (4.1), p = 0.022) (Table 4). On comparing the key performance indicators of ovarian stimulation, the mean (SD) follicular output rate (FORT) was significantly higher in the Folisurge vs. the Gonal-f group (72.4 (19.4) vs. 70.7 (18.8), p = 0.004). Further analysis of the oocyte and embryo outcomes according to the starting dose suggested that more number of oocytes were retrieved in the Folisurge vs. the Gonal-f groups across most of the dosages studied (Table 5). On comparison of the number of MII oocytes formed, Folisurge performed better in all doses except ≥ 300 IU. It was found that Folisurge formed more embryos than Gonal-f across most of the doses studied.
The serum β-hCG positive rate was similar in both groups (75.5% vs. 76.2%; p = 0.667) (Figure 2). On further subgroup analysis according to the starting dose, there was not much variation among the two groups in the various doses studied (Figure 3). A review of patient records revealed no documented cases of severe ovarian hyperstimulation syndrome (OHSS) or other major adverse events leading to hospitalization in either group.
Serum β-hCG positive rate in each of the groups of participants receiving either Folisurge or Gonal-f.β-hCG: β-human chorionic gonadotropin.
Serum β-hCG positive rate according to starting dose in each of the groups of participants receiving either Folisurge or Gonal-f.β-hCG: β-human chorionic gonadotropin.
Discussion
In this current study, we examined the variance of the r-FSH beginning dose, a significant and contentious issue, and reported on the first usage of a biosimilar r-FSH, Folisurge, against the innovator Gonal-f in 106 ART sites throughout India. In terms of serum hCG-positive rates in actual clinical practice, this study also demonstrates that Folisurge and the pioneer Gonal-f are equally effective. Homogeneity of the comparison populations and intriguing information on the connection between FSH dose, conditions of usage of these doses, and outcomes are provided by the analyses based on the initial r-FSH dose [8].
Manzi et al. (2022) compared the structural features of Gonal-f vs. r-FSH biosimilar preparations in non-European regions, and Folisurge was the only biosimilar chosen from India. The biosimilars were compared with respect to glycosylation, macro- and micro-heterogeneity, sialylation, and immunogenicity. It was found that Folisurge was aligned with the Gonal-f across all N-glycosylation sites, and it had a higher degree of O-acetylation vs. Gonal-f, which is a representative of a lower risk of immunogenicity [14]. Despite minor changes in the structure of biosimilar preparations vis-à-vis the reference product, ultimately, the clinical efficacy and safety are of paramount importance. This study was conducted to obtain information on the comparison of Folisurge vs. Gonal-f on the efficacy aspect.
The number of oocytes retrieved is considered a surrogate marker of the efficacy of the medication and is often used in different studies [15]. Also, considering the fact that the number of MII oocytes retrieved may have a bearing on the clinical pregnancy outcomes [16], the number of MII oocytes retrieved was considered as the primary outcome in the current study. The mean (SD) number of MII oocytes retrieved in the Folisurge group was significantly higher than the Gonal-f group (13.0 (7.5) vs. 10.9 (6.6); p < 0.001). Also, the MII oocyte rate was significantly higher in the Folisurge group versus the Gonal-f group (71.4% vs. 69.9%; p = 0.001), suggesting that Folisurge was better in terms of the quality of oocytes retrieved per patient. In a similar study conducted by Barakhoeva et al. (2019) comparing Primapur (recombinant FSH alfa biosimilar) with Gonal-f showed that the mean number of MII oocytes retrieved was similar (Primapur = 9.6 (6.3) vs. Gonal-f = 9.9 (5.6); p = 0.617). This shows that biosimilars can also produce equal efficacy vis-à-vis originator [17].
It was observed that the mean (SD) number of embryos formed in the Folisurge group was significantly higher than the Gonal-f group (4.9 (4.1) vs. 4.7 (4.1); p = 0.022). Further, while comparing the subgroups based on the starting dose, it was found that more embryos were formed with Folisurge than Gonal-f in all dosage groups, except 151-224 IU. Folisurge was comparable to Gonal-f in terms of serum β-hCG positive rate (75.5% vs. 76.2%; p = 0.667). On further subgroup analysis, according to the starting dose, there was not much variation between the two drugs. Similar results were observed by Barakhoeva et al. (2019) in terms of serum β-hCG positive rate among Primapur and Gonal-f (34.7% vs. 36.7%; p = 0.833) [17].
The age, BMI, weight, polycystic ovarian syndrome, smoking history, severe endometriosis, prior ovarian response, prior pelvic surgery, AFC, ovarian volume, ovarian stromal blood flow, serum AMH, serum FSH, serum luteinizing hormone, serum estradiol, serum inhibin B, serum testosterone, and various dynamic tests of ovarian reserve are all important factors to consider when determining the starting dose of r-FSH. [8] The goal is to achieve an adequate response to ovarian stimulation while minimizing the risk of OHSS. The r-FSH starting dosage may be determined with the use of a variety of prediction algorithms [8,18]. The prescribing information of Gonal-f mentions that there have been a few cases of severe adverse effects, including hypersensitivity. This highlights the need for comprehensive safety monitoring with detailed surveillance for rare and atypical reactions (both clinical and biochemical) to ensure a complete understanding of its safety profile [19]. Furthermore, because prognostic variables combine in a complicated way, there is currently no universally accepted method for determining the first r-FSH alpha dosage for every patient; instead, the treating physician's professional opinion is eventually used [8]. In our study, when the subgroup analysis based on the starting dose of FSH was conducted between the Folisurge and Gonal-f groups, the results were comparable in both groups.
Limitations
Many bodies, such as the European Society of Human Reproduction and Embryology (ESHRE) and the International Committee Monitoring Assisted Reproductive Technologies (ICMART), consider live birth and cumulative live birth as the most relevant outcome for infertility treatment [18,20]; however, the same could not be captured in the current study. The lack of live birth rate data is a significant limitation, as it prevents full assessment of the comparative clinical efficacy of the two treatments. Being a real-world study, structured adverse event reporting was missing. Another limitation of our study was its retrospective nature. Multicenter, randomized, double-blind, controlled clinical studies are required to compare the clinical outcomes, especially live birth rate, of Folisurge vs. Gonal-f. A pharmacoeconomic analysis will be helpful in further evaluating the cost-effectiveness of biosimilars.
Conclusions
Folisurge was comparable to Gonal-f in terms of serum β-hCG positive rate. The higher yield of oocytes and embryos in the Folisurge group should be interpreted in the context of its higher baseline AFC, which may have influenced these results. No major safety concerns were observed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Prevalence of primary infertility and its associated risk factors in urban population of central India: a community-based cross-sectional study Indian J Community Med Katole A Saoji AV 3373414420193180279610.4103/ijcm.IJCM_7_19PMC 6881900 · doi ↗ · pubmed ↗
- 2Genetics of human male infertility Singapore Med J Poongothai J Gopenath TS Manonayaki S 336347502009 https://pubmed.ncbi.nlm.nih.gov/19421675/19421675 · pubmed ↗
- 3Regimen of ovarian stimulation affects oocyte and therefore embryo quality Fertil Steril Bosch E Labarta E Kolibianakis E Rosen M Meldrum D 56057010520162682627310.1016/j.fertnstert.2016.01.022 · doi ↗ · pubmed ↗
- 4Human recombinant FSH and its biosimilars: clinical efficacy, safety, and cost-effectiveness in controlled ovarian stimulation for in vitro fertilization Pharmaceuticals (Basel) Bergandi L Canosa S Carosso AR 1361320203260513310.3390/ph 13070136 PMC 7407829 · doi ↗ · pubmed ↗
- 5Gonadotrophins - filled-by-mass versus filled-by-bioassay Reprod Biomed Online Hugues JN Durnerin IC 111710200510.1016/s 1472-6483(11)60385-423577410 · doi ↗ · pubmed ↗
- 6European Medicines Agency. Gonal-f 5 2025 2018 https://www.ema.europa.eu/en/medicines/human/EPAR/gonal-f
- 7Comparison of pharmacokinetic and safety profiles between Bemfola® and Gonal-f® after subcutaneous application Eur J Drug Metab Pharmacokinet Wolzt M Gouya G Sator M Hemetsberger T Irps C Rettenbacher M Vcelar B 2592654120162563323910.1007/s 13318-015-0257-6PMC 4866993 · doi ↗ · pubmed ↗
- 8A real-world study of ART in France (REOLA) comparing a biosimilar r FSH against the originator according to r FSH starting dose J Gynecol Obstet Hum Reprod Barrière P Hamamah S Arbo E Avril C Salle B Pouly JL Jenkins J 1025105220233640390010.1016/j.jogoh.2022.102510 · doi ↗ · pubmed ↗