Associations of selective serotonin reuptake inhibitors and long COVID risk in patients with depression: a retrospective cohort study
Zhenxiang Gao, Tomasz Tabernacki, Pamela B. Davis, David C. Kaelber, Rong Xu

TL;DR
This study found that using SSRIs, a type of antidepressant, may lower the risk of long COVID in adults with depression compared to other antidepressants.
Contribution
The study provides new evidence that SSRIs might reduce long COVID risk in patients with depression.
Findings
SSRI use was associated with a 41-43% lower risk of long COVID diagnosis compared to non-SSRIs.
Sensitivity analyses confirmed reduced long COVID symptoms with SSRI use across different timeframes.
Results were consistent across symptom categories and pandemic periods.
Abstract
To evaluate the potential of selective serotonin reuptake inhibitors (SSRIs) in reducing the risk of long COVID in patients with depression. This retrospective cohort study analyzed U.S. electronic health records from TriNetX platform to compare the risk of long COVID among adults with depression who were prescribed SSRIs versus non-SSRI antidepressants between March 2020 and December 2022. The main outcome was the long COVID diagnosis. As a sensitivity analysis, CDC-defined long COVID symptoms were used as alternative outcomes. Cox proportional hazards models were used to assess outcomes occurring 3–6 and 3–12 months after the index SARS-CoV-2 infection, with hazard ratios (HRs) and 95% confidence intervals (CIs) calculated. After propensity score matching, the study included 31,264 patients, and the risk of long COVID diagnosis was significantly lower in the SSRI cohort compared to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
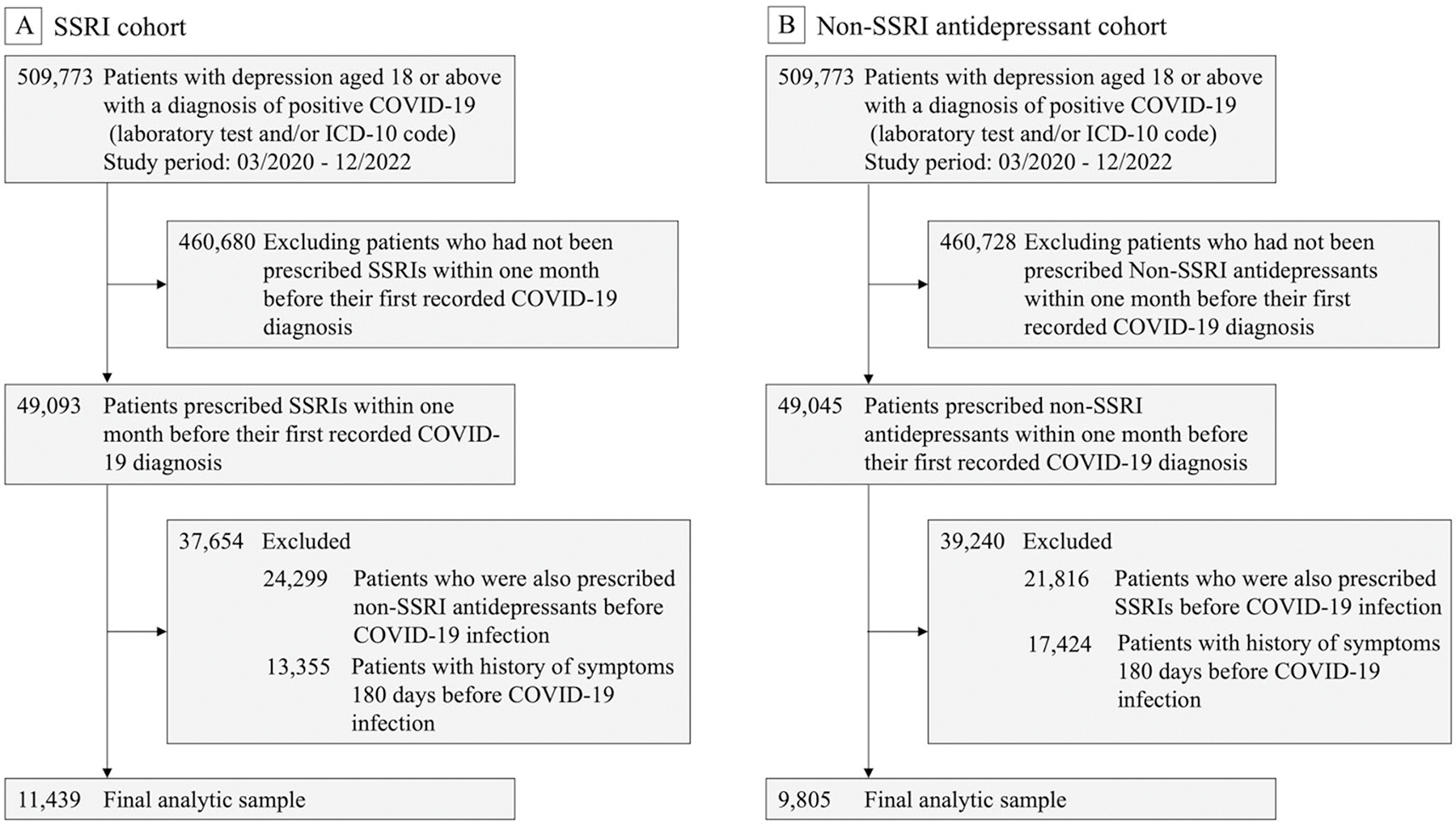 Figure 1
Figure 1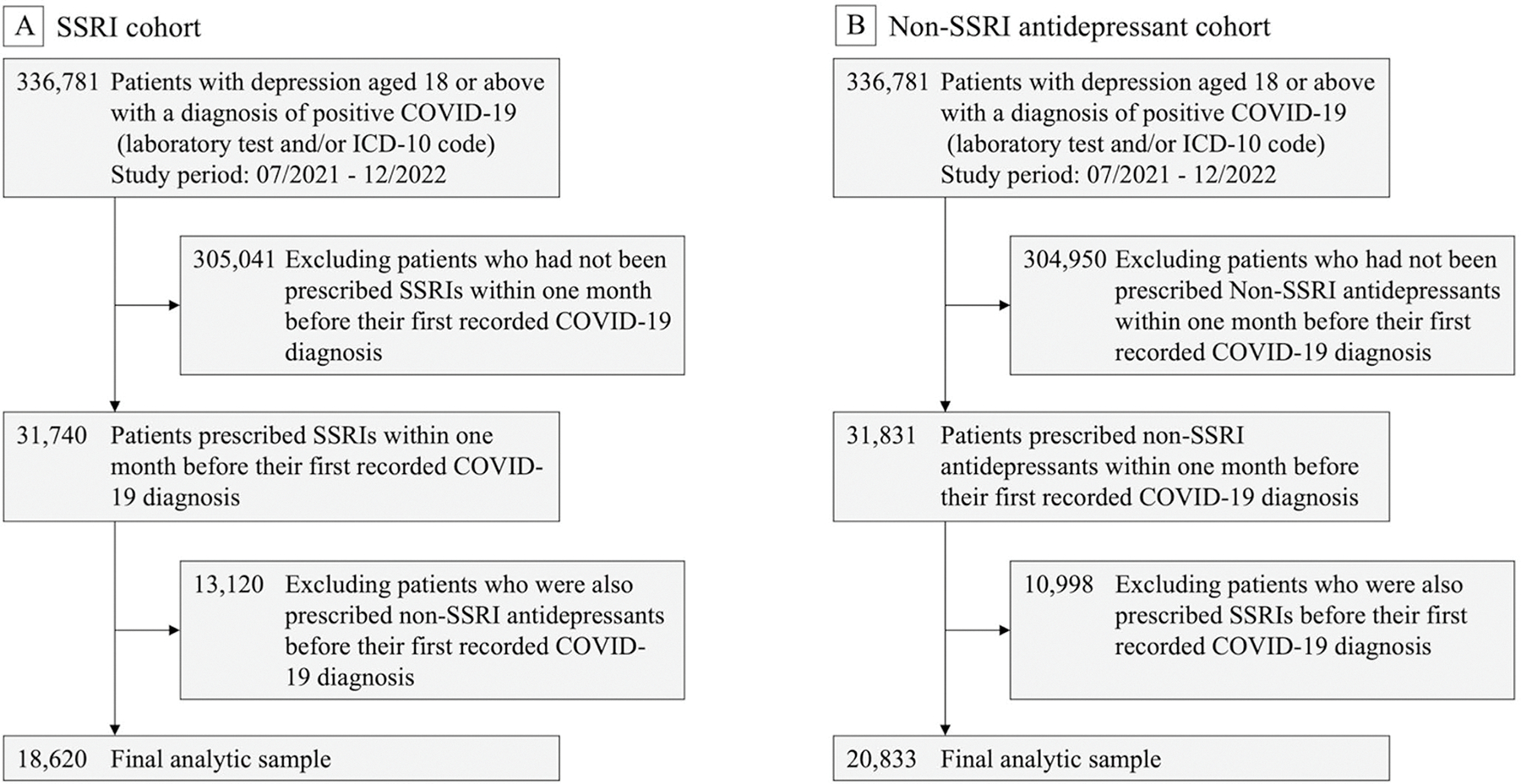 Figure 2
Figure 2 Figure 3
Figure 3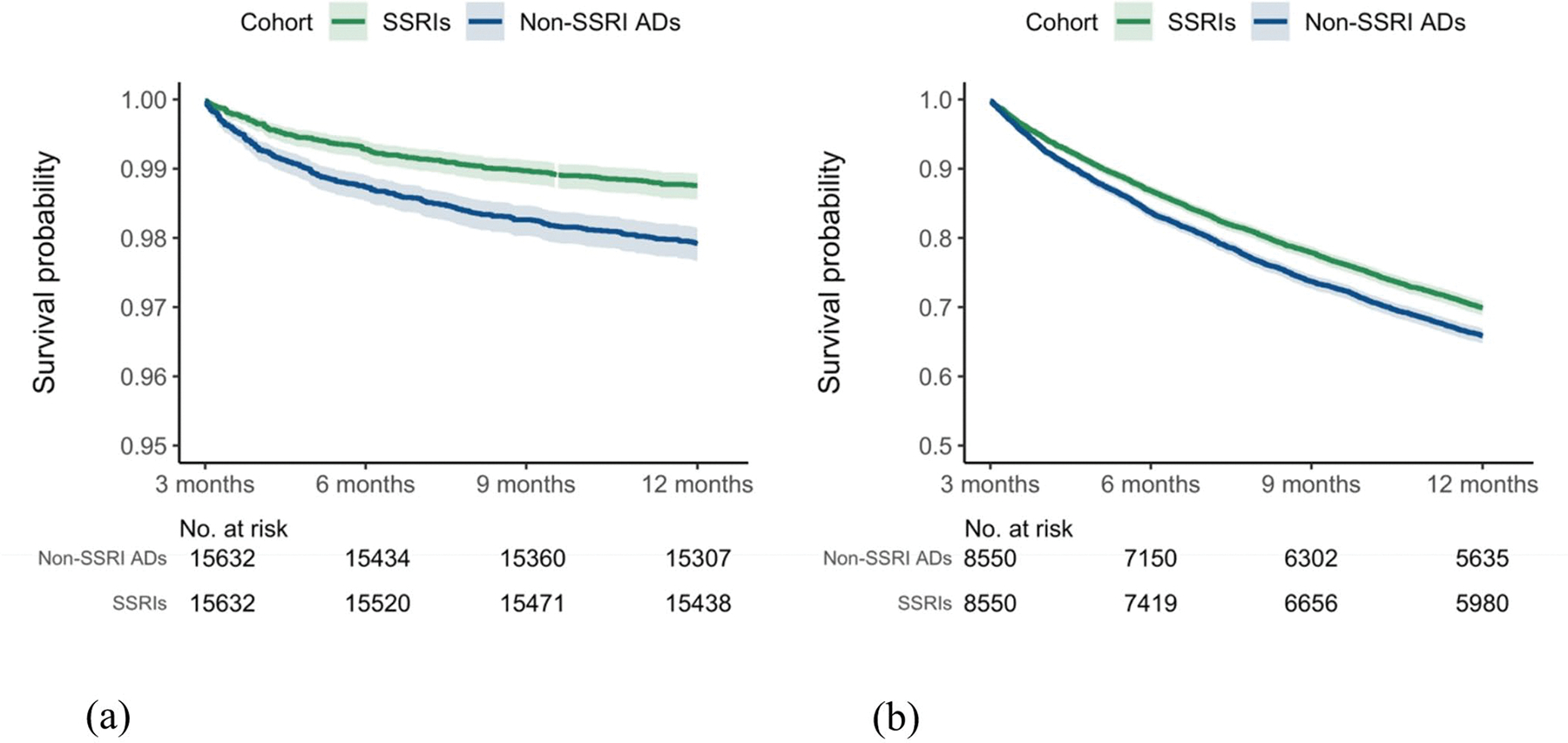 Figure 4
Figure 4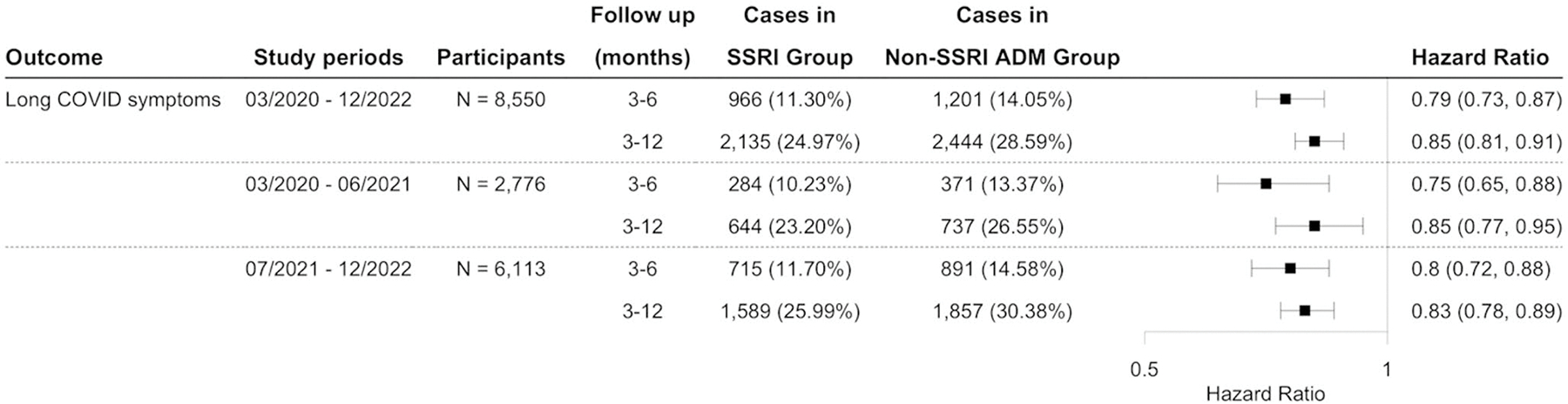 Figure 5
Figure 5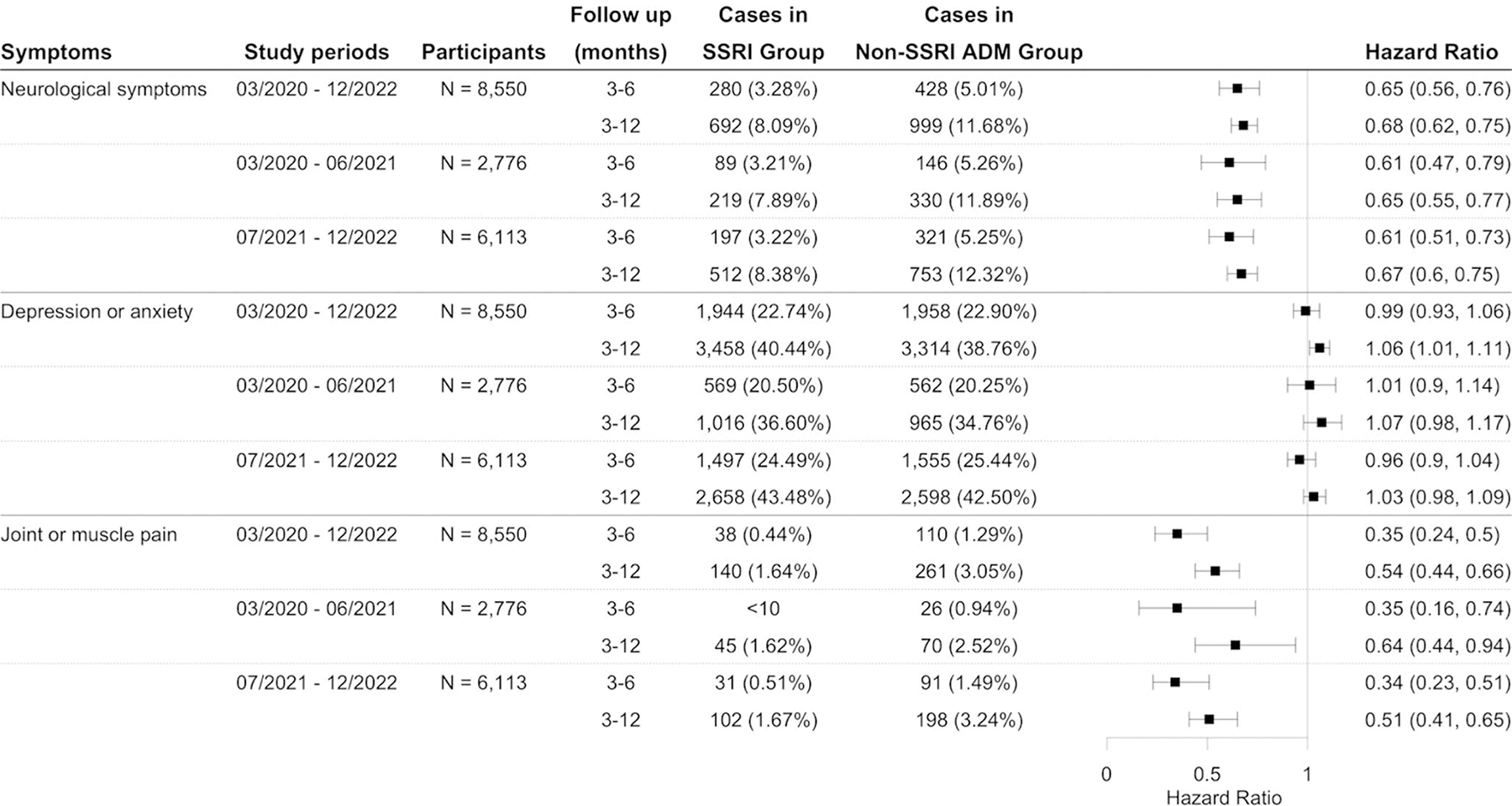 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLong-Term Effects of COVID-19 · COVID-19 and Mental Health · Tryptophan and brain disorders
Introduction
Long COVID, also known as post-acute sequelae of SARS-CoV-2 infection (PASC), has rapidly evolved into one of the most pressing health crises of the post-pandemic era, affecting an estimated 65 million people worldwide and imposing enormous burdens on patients, healthcare systems, and societies [1, 2]. Defined by the World Health Organization (WHO) and Centers for Disease Control and Prevention (CDC) as persistent chronic symptoms emerging at least 3 months post-infection, long COVID commonly presents with debilitating fatigue, cognitive impairment (“brain fog”), dyspnea, and musculoskeletal pain [3, 4]. Despite its high prevalence, there is a lack of effective treatments for long COVID.
Depression appears to compound this challenge, possibly through shared neuroinflammatory pathways. SARS-CoV-2 infection triggers systemic and central inflammatory responses, correlating strongly with acute depressive symptoms [5–7]. Prospective cohorts show that patients who screen positive for depression one month after COVID-19 infection were more likely to report persistent physical and cognitive complaints at three months [8, 9]. Because depression itself is accompanied by immune dysregulation, timely treatment might lessen downstream inflammatory sequelae. Selective serotonin reuptake inhibitors (SSRIs), commonly prescribed as first-line treatments for depression, reduce neuroinflammation and have been observed to alleviate proinflammatory cytokine levels in clinical studies [10, 11]. We hypothesize that SSRI therapy at the time of infection had potential in preventing long-COVID development.
Several studies have investigated the association between SSRI use and long COVID [12, 13]. A completed phase 2 trial of vortioxetine reported cognitive improvement in adults with post-acute COVID symptoms, especially in those with metabolic dysregulation and low-grade inflammation [14]. Meanwhile, additional SSRI treatment trials testing fluvoxamine and fluoxetine are ongoing [15]. Observational studies have shown inconsistent results. Analyses using the National COVID Cohort Collaborative (N3C) dataset indicated that SSRI use may reduce the risk of Long COVID [16, 17], whereas a study using the U.S. Veterans’ dataset found no such association [18]. These inconsistent findings may have resulted from different long COVID definitions, study periods, follow-up times, heterogeneous study populations, and non-active comparators.
In this study, we conducted a retrospective cohort study using electronic health records from the TriNetX database to investigate the association between SSRI use and the risk of long COVID compared with non-SSRI antidepressants in patients with depression. We also conducted extensive sensitivity analyses using two different definitions of long COVID, across different pandemic periods and follow-up durations. Additional subgroup analyses were performed based on symptom categories.
Methods
Data source
This study utilized data from TriNetX [19], a global federated health research network that provides continuously updated electronic health records (EHR) from over 100 million patients across 59 healthcare organizations in the United States. The patient distribution within the TriNetX network includes 25% from the Northeast, 17% from the Midwest, 41% from the South, and 12% from the West, with 5% of origins unknown. This retrospective study is exempt from informed consent. The data reviewed is a secondary analysis of existing data, does not involve intervention or interaction with human subjects, and is de-identified per the de-identification standard defined in Section § 164.514(a) of the HIPAA Privacy Rule. The process by which the data is de-identified is attested to through a formal determination by a qualified expert as defined in Section § 164.514(b)(1) of the HIPAA Privacy Rule. This formal determination by a qualified expert was refreshed in December 2020. Previously, we have utilized the TriNetX Analytics platform to conduct cohort studies, including evaluations of the potential clinical efficacy of drugs [20–25].
Study population
The study cohort consisted of depression patients aged 18 years or older with documented COVID-19 infection, identified through either an encounter diagnosis code for COVID-19 or a positive SARS-CoV-2 antibody test result. COVID-19 diagnosis was identified using the ICD-10 code U07.1 or a positive RNA-based COVID-19 test recorded in TriNetX (code 9088, “SARS coronavirus 2 and related RNA”). Depression diagnoses were determined using ICD-10 codes for “Depressive Episode” (F32) and “Recurrent Major Depressive Disorder” (F33). The exposure was selective serotonin reuptake inhibitors (SSRIs), including citalopram, escitalopram, paroxetine, sertraline, fluvoxamine, fluoxetine, vortioxetine, and vilazodone. The comparison was with antidepressants other than SSRIs (non-SSRI antidepressants).
This study investigated the risk of long COVID in patients with preexisting depression following SARS-CoV-2 infection, focusing on the impact of SSRI use compared to non-SSRI antidepressants. The primary outcome, long COVID, was defined in TriNetX using the ICD diagnosis code U09.9 (“Post COVID-19 condition”). Since the ICD code U09.9 became effective on October 1, 2021, the study population included individuals who had a documented depression diagnosis with an active prescription for an antidepressant within one month prior to their first recorded COVID-19 diagnosis, between July 2021 and December 2022. The patients were categorized into two groups: (1) the SSRI group, consisting of individuals who were prescribed SSRIs without any other antidepressants, and (2) the non-SSRI antidepressant group, which included patients prescribed antidepressants but not SSRIs. Cohort selection details are illustrated in Fig. 1, which outlines the study design and inclusion criteria.
For sensitivity analyses, we used long COVID symptoms defined by the CDC as a range of symptoms or conditions that occur after SARS-CoV-2 infection and persist for at least three months [24]. Patient data were collected from March 2020 through December 2022. The SSRI group consisted of individuals with a documented diagnosis of depression who were prescribed SSRIs within one month prior to their first recorded COVID-19 diagnosis. The non-SSRI antidepressant group comprised patients prescribed other antidepressants during the same pre-infection window. Both groups had no history of long COVID symptoms within 180 days before SARS-CoV-2 infection. Figure 2 illustrates the details of cohort selection. For subgroup analyses, the study period was stratified into two phases based on the dominant SARS-CoV-2 variants: March 2020 to June 2021, primarily characterized by Alpha and Beta variants, and July 2021 to December 2022, predominantly marked by Delta and Omicron variants. Additionally, we categorized long COVID symptoms into groups, including general symptoms, respiratory and cardiovascular symptoms, neurological symptoms, digestive symptoms, and other symptoms including skin rashes, joint or muscle pain. We separately examined the associations of SSRIs with each of these symptom groups. Details of specific ICD-10 codes for identifying these groups are provided in Supplementary Table S1 [26]. Since this study specifically focused on patients with depression, depression and anxiety symptoms were separated from the neurological category and analyzed as a distinct group. We further evaluated consistency across different drug exposure windows and compared outcomes between SSRIs with and without sigma-1 receptor (S1R) agonist activity, because previous studies suggest that S1R agonism may be a mechanism by which SSRIs reduce inflammatory responses [17].
Propensity score matching was applied to balance key characteristics between the exposure and control groups. Covariates were selected based on their relevance to long COVID risk [16, 17, 27–29] and included demographics (age, sex, and ethnicity), socioeconomic factors (education level, employment status, social and psychosocial environment, and housing conditions), problems related to lifestyle, and psychiatric comorbidities (schizophrenia, mood disorders, and anxiety disorders). Additionally, we controlled for chronic health conditions such as hypertension, diabetes, heart disease, cerebrovascular disease, respiratory diseases, cancer, kidney disease, liver disease, nicotine dependence, alcohol addiction, and obesity. We also adjusted for prior hospital inpatient and observation care services, medication history, including prescriptions associated with COVID-19. The list of covariates is included in Supplementary Table S2.
Statistical analyses
To evaluate differences in long COVID risk between patients prescribed SSRIs and those prescribed non-SSRI antidepressants, hazard ratios (HRs) with 95% confidence intervals (CIs) were estimated using Cox proportional hazards regression models to quantify the relative risk between the two treatment groups. Cumulative incidences were estimated using Kaplan-Meier survival analysis. The index event, marking the start of follow-up, was defined as the first recorded COVID-19 diagnosis. Patients in the matched cohorts were followed until the occurrence of the outcome, death, loss to follow-up, or the end of the predefined follow-up windows (3–6 months and 3–12 months post-index), whichever occurred first. All statistical analyses were conducted using the TriNetX Analytics platform. Statistical significance was determined using a two-sided p-value threshold of < 0.05, with analyses finalized in April 2025.
Results
Using the ICD-10 diagnosis code-based definition of long COVID for the study period from July 2021 to December 2022, the initial population comprised 18,620 patients prescribed SSRIs, and 20,833 patients prescribed non-SSRI antidepressants between July 2021 and December 2022 (Table 1). Compared to the SSRI group, those in the non-SSRI cohort had a higher proportion of males and African Americans and a higher prevalence of heart failure, hypertension, respiratory diseases, alcohol/nicotine addiction, and obesity. After propensity-score matching, the two cohorts were balanced. As illustrated in Fig. 3, patients receiving SSRIs exhibited a significantly lower hazard ratio for developing long COVID after COVID-19 infection compared to those prescribed non-SSRI antidepressants, with hazard ratios of 0.57 (95% CI: 0.44–0.73) and 0.59 (95% CI: 0.49–0.72) at follow-up periods of 3 to 6 months and 3 to 12 months, respectively. The Kaplan-Meier curve for the study cohort with the outcome of long COVID using the ICD-10 diagnosis code was shown in Fig. 4(a). Consistent protective associations were observed in analyses using alternative drug exposure windows (Figure S1 in Supplementary File). Furthermore, no significant reduction in long COVID risk was observed between patients prescribed S1R agonist SSRIs and those prescribed other SSRIs without S1R agonist activity (Figure S2 in Supplementary File).
Using the long COVID definition based on the CDC definition for the study period from March 2020 and December 2022, this study identified an initial cohort of 11,439 patients who received SSRIs, and 9,850 patients prescribed non-SSRI antidepressants. The characteristics of the matched cohorts are presented in Supplementary Table S3. SSRI was significantly associated with a reduced risk of long COVID-related symptoms compared to non-SSRI antidepressants, with hazard ratios of 0.79 (95% CI: 0.73–0.87) and 0.85 (95% CI: 0.81–0.89) at 3–6 and 3–12 months of follow-up, respectively (Fig. 5). Figure 4(b) presents the Kaplan-Meier curve for the study cohort with long COVID symptoms as the outcome. This reduced risk remained consistent when the analysis was stratified by study period according to the dominant SARS-CoV-2 variants (Fig. 5). Sensitivity analyses by the symptom group revealed that patients prescribed SSRIs had a lower risk of developing neurological symptoms and joint or muscle pain compared to those receiving non-SSRI antidepressants (Fig. 6), but not depression or anxiety symptoms. Additional details of other symptoms are provided in Figure S3 of the supplementary file. Analyses using different drug exposure windows showed consistent protective associations, while no significant difference in long COVID risk was observed between patients prescribed S1R agonist SSRIs versus SSRIs without S1R agonist activity (Figures S4–S5, Supplementary File).
Discussion
In this study, we conducted a retrospective observational study that showed that patients with depression who were prescribed SSRIs exhibited a significantly lower risk of long COVID - particularly neurological and musculoskeletal symptoms - after SARS-CoV-2 infection compared to matched patients prescribed non-SSRI antidepressants. These findings were consistent across different long COVID definitions, follow-up intervals, and SARS-CoV-2 variant periods.
Our study findings align with recent large-scale observational evidence suggesting SSRIs may be associated with a reduced risk of developing long COVID after SARS-CoV-2 infection. A retrospective study of 302,626 patients with a diagnosis of depression before COVID diagnosis found that SSRI use was associated with a risk ratio of 0.92 (95% CI: 0.86, 0.99) for diagnosis with long COVID compared to those not using an SSRI [16]. Similarly, in a study of 17,908 patients with COVID-19 from the National COVID Cohort Collaborative (N3C), individuals exposed to S1R agonist SSRIs showed a 29% reduction in relative risk of long-COVID [17]. In contrast, one study analyzing the U.S. veterans’ dataset reported no significant association between SSRI use and the risk of long COVID [18]. However, this study included a heterogeneous cohort of patients with anxiety, depression, or post-traumatic stress disorder (PTSD) and compared users of SSRIs with patients who did not use any antidepressants, which could suffer confounding effects by indications. Our study included 31,264 COVID patients with depression and compared patients prescribed SSRIs to those receiving non-SSRI antidepressants. We found that SSRI use was associated with a reduced risk of long COVID compared to non-SSRI antidepressants. Taken together, findings from our study suggest that SSRIs may have a protective effect in preventing or delaying the development of long COVID in patients with depression following COVID-19 infection.
In an exploratory cohort of 95 post-COVID-19 patients treated with SSRIs, Rus et al. observed substantial symptom amelioration across neuropsychiatric and musculoskeletal domains: “brain fog” and sensory overload scores decreased by an average of 3.8 and 3.6 points respectively, and Bell functional scores nearly doubled from 23.5 to 47.2 within 4–6 weeks of SSRI initiation [12]. These findings mirror our subgroup analyses, which showed that SSRI initiation prior to SARS-CoV-2 infection was chiefly associated with reduced neurological manifestations (e.g., cognitive impairment, headache, sleep disturbance) and musculoskeletal pain, while affective, constitutional, gastrointestinal, and dermatological PASC symptoms were unchanged. By contrast, our propensity-matched comparison of SSRI versus non-SSRI antidepressant users revealed no significant difference in rates of ongoing depression or anxiety symptoms. This diverges from earlier work by Mazza et al., who reported a 92% response (≥ 50% reduction on Hamilton Depression Rating Scale) in 60 post-COVID depression patients treated with SSRIs versus non-users [13]. However, this study only compared SSRIs against SSRI-naïve groups, whereas we compared versus individuals receiving other antidepressant medications.
SSRIs modulate both innate and adaptive immune pathways in ways that could attenuate the persistent inflammation underlying long-COVID. Long COVID is characterized by persistent immune activation with elevated proinflammatory cytokines, chemokines, and type I interferon signatures that correlate with prolonged neurocognitive and somatic symptoms [30, 31]. SSRIs possess well-described immunomodulatory properties: they suppress proinflammatory cytokine release, restore IFN/IL-10 balance, deplete platelet serotonin to limit neutrophil endothelial adhesion, and modulate lymphocyte signaling [32, 33]. Clinical meta-analyses further show SSRI therapy reduces circulating IL-6, IL-1β, and TNF-α [34, 35]. Though further work is needed to further characterize long-COVID associated immunomodulatory mechanisms, there is a plausible biological rationale for SSRIs to attenuate the maladaptive inflammation of long COVID and thereby decrease its incidence and severity.
Strengths and limitations
Our study has several key strengths. First, we employed both a clinician-coded U09.9 diagnosis and the CDC symptom-based definition of long COVID to ensure robustness of our overall findings. Second, our findings were consistent across multiple SARS-CoV-2 variant periods and follow-up intervals.
Several limitations of our analysis merit consideration. First, the retrospective EHR-based observational study has limitations of residual confounding and biases, therefore causality cannot be established. Second, our primary outcome (clinician-coded long COVID via ICD-10 U09.9) became available only in October 2021 and underestimated the true incidence of long COVID. For sensitivity analysis, we used the CDC symptom-based definition, and the overall findings were consistent for these two long COVID definitions. Third, details on SSRI dose, duration, and adherence were not able to be ascertained from patient EHRs. In addition, our cohort is restricted to patients with diagnosed depression engaged in healthcare systems contributing to TriNetX. The generalizability of our findings needs to be validated in other populations or other databases.
Conclusions
In summary, our findings suggest that SSRIs were associated with a lower risk of developing long-COVID, particularly its neurologic and musculoskeletal sequelae, in patients with depression, compared with non-SSRI antidepressants. If confirmed in prospective trials, this could identify SSRIs as readily available, well-tolerated agents for long-COVID mitigation. Future work should include randomized clinical trials to establish causality and mechanistic investigations.
Supplementary Material
Supplement
Supplementary Information The online version contains supplementary material available at https://doi.org/10.1007/s15010-025-02648-z.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ballering AV, van Zon SK, olde Hartman TC, Rosmalen JG. Persistence of somatic symptoms after COVID-19 in the netherlands: an observational cohort study. Lancet. 2022;400(10350):452–61.35934007 10.1016/S 0140-6736(22)01214-4PMC 9352274 · doi ↗ · pubmed ↗
- 2Al-Aly Z, Davis H, Mc Corkell L, Long COVID science, research and policy. Nat Med. 2024;30(8):2148–64.39122965 10.1038/s 41591-024-03173-6 · doi ↗ · pubmed ↗
- 3Soriano JB, Murthy S, Marshall JC, Relan P, Diaz JV. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect Dis. 2022;22(4):e 102–7.34951953 10.1016/S 1473-3099(21)00703-9PMC 8691845 · doi ↗ · pubmed ↗
- 4Chaichana U, Man KK, Chen A, Definition of post–COVID-19 condition among published research studies. JAMA Netw Open. 2023;6(4):e 235856.37017970 10.1001/jamanetworkopen.2023.5856 PMC 10077105 · doi ↗ · pubmed ↗
- 5Monje M, Iwasaki A. The neurobiology of long COVID. Neuron. 2022;110(21):3484–96.36288726 10.1016/j.neuron.2022.10.006PMC 9537254 · doi ↗ · pubmed ↗
- 6Vanderheiden A, Klein RS. Neuroinflammation and COVID-19. Curr Opin Neurobiol. 2022;76:102608.35863101 10.1016/j.conb.2022.102608 PMC 9239981 · doi ↗ · pubmed ↗
- 7Almutairi MM, Sivandzade F, Albekairi TH, Alqahtani F, Cucullo L. Neuroinflammation and its impact on the pathogenesis of COVID-19. Front Med (Lausanne). 2021;8:745789.34901061 10.3389/fmed.2021.745789 PMC 8652056 · doi ↗ · pubmed ↗
- 8Bottemanne H, Gouraud C, Hulot JS, Do anxiety and depression predict persistent physical symptoms after a severe COVID-19 episode? A prospective study. Front Psychiatry. 2021;12:757685.34858230 10.3389/fpsyt.2021.757685 PMC 8631493 · doi ↗ · pubmed ↗