Triage Accuracy and the 2015 Field Trauma Triage Criteria Update
Bourke W. Tillmann, Avery B. Nathens, Matthew P. Guttman, Corey Freedman, Priscila Pequeno, Damon C. Scales, Petros Pechlivanoglou, Barbara Haas

TL;DR
Updating trauma triage guidelines initially reduced undertriage but led to a gradual increase over five years, highlighting the need for ongoing monitoring.
Contribution
The study evaluates the long-term impact of updated trauma triage guidelines on triage accuracy in a mature trauma system.
Findings
Implementation of updated FTT guidelines caused a 15.2% immediate decrease in undertriage.
Undertriage rates increased by 2.4% annually over five years after guideline implementation.
Overtriage rates decreased by 3.8% annually following the updated guidelines.
Abstract
Was the implementation of updated field trauma triage (FTT) guidelines on triage practices associated with changes in rates of overtriage or undertriage in a large, regional trauma system? In this population-based cohort study of 281 268 injured patients, the implementation of updated FTT guidelines was associated with a 15.2% instantaneous decrease in the rate of undertriage. However, during the 5 years after the implementation of the new guidelines, rates of undertriage increased by 2.4% annually. These findings suggest that while implementation of updated FTT guidelines was associated with a decrease in undertriage, ongoing monitoring is required to ensure that the benefits associated with new guidelines are maintained. This cohort study examines the association between the 2015 update to field trauma triage guidelines and trends in trauma triage in Ontario, Canada. Despite…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
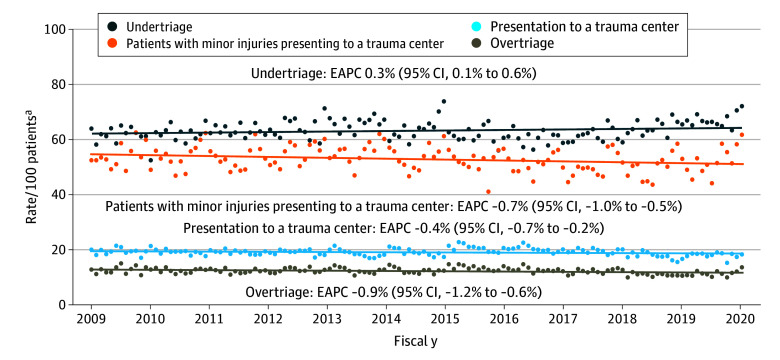 Figure 1
Figure 1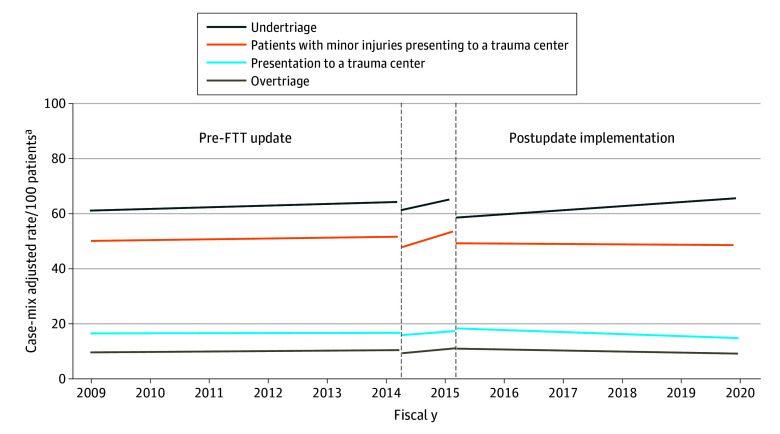 Figure 2
Figure 2| Criteria | Preimplementation guidelines | Postimplementation guidelines |
|---|---|---|
| Transport time | If <30 min, bypass local hospitals and transport to nearest trauma center If >30 min, transport by air ambulance to trauma center when available | If <30 min, bypass local hospitals and transport to nearest trauma center (may be extended to 60 min in specific scenarios) If >30 min, transport by air ambulance to trauma center when available and air travel time is less than land time |
| Physiologic criteria | GCS ≤10 If GCS >10 any 2 of: Altered level of consciousness HR <50 or >120 bpm SBP <80 mm Hg or absent radial pulse RR <10 or >24 breaths per min | GCS <14 SBP <90 mm Hg RR<10 or ≥30 breaths per min or need for ventilatory support |
| Anatomic | Penetrating injury to head, neck, trunk, or groin Amputation above wrist or ankle Spinal cord injury with paraplegia or quadriplegia | Penetrating injury to head, neck, trunk, or proximal to elbows or knees Chest wall instability or deformity (eg, flail chest) ≥2 Proximal long-bone fractures Crusted, degloved, mangled, or pulseless extremity Amputation proximal to wrist or ankle Pelvic fractures Open or depressed skull fracture Paralysis |
| Mechanism | Fall >5 m (16.4 ft) MVC >30 km/h (18.6 mi/h) or death of a co-occupant Person ejected from vehicle at speed >30km/h (18.6 mi/h) MVC rollover with unbelted occupant Vehicle struck fixed object (eg, rock cut, tree, pole) or large animal (eg, moose, deer, bear) Pedestrian struck by vehicle >15km/h (9.3 mi/h) | Fall ≥6 m (19.7 ft) MVC with intrusion ≥0.3 m (1 ft) on patient’s side or ≥0.5 m (1.6 ft) at any site Person ejected from vehicle MVC with death in the same passenger compartment MVC with telemetry data consistent with high-risk injury Motorcycle crash ≥30 km/h (18.6 mi/h) Pedestrian or bicyclist thrown, run over, or struck by vehicle ≥30 km/h (18.6 mi/h) |
| Diversion | Uncomfortable with safety of patient during transport Concern patient will not survive transport to nearest trauma center Despite the above, VSA patients with penetrating thoracoabdominal injuries may bypass local EDs to facilitate transportation to nearest trauma center | Unable to secure airway Patient unlikely to survive transport to trauma center Despite the above, transport patients to nearest trauma center if they meet all the following: Penetrating torso, head, or neck injury VSA but do not meet TOR criteria Transport to the trauma center <30 min |
| Special criteria suggesting lower threshold for transport to trauma center | None | Age >55 y Age >65 y and SBP <110 mm Hg Using anticoagulants or having a bleeding disorder Combined burns and trauma ≥20 wk pregnant |
| Characteristic | Patients, No. (%) | Standardized differences | ||
|---|---|---|---|---|
| Overall (N = 281 286) | Preimplementation (n = 127 275) | Postimplementation (n = 130 680) | ||
| Age, y | ||||
| Mean (SD) | 62.4 (22.5) | 60.4 (22.7) | 64.1 (22.1) | 0.16 |
| ≥65 | 142 980 (50.8) | 59 862 (47.0) | 70 938 (54.3) | 0.15 |
| Sex | ||||
| Female | 141 450 (50.3) | 63 152 (49.6) | 66 350 (50.8) | 0.02 |
| Male | 139 818 (49.7) | 64 123 (50.4) | 64 330 (49.2) | |
| Comorbidity level | ||||
| Low | 110 340 (39.2) | 52 390 (41.2) | 48 748 (37.3) | 0.08 |
| Moderate | 84 144 (29.9) | 38 345 (30.1) | 38 877 (29.7) | 0.01 |
| High | 86 784 (30.9) | 36 540 (28.7) | 43 055 (32.9) | 0.09 |
| Frail | 49 171 (17.5) | 19 584 (15.4) | 23 394 (19.4) | 0.11 |
| Long-term home care | 29 004 (10.3) | 12 224 (9.6) | 14 306 (10.9) | 0.04 |
| Nursing home resident | 23 423 (8.3) | 8831 (6.9) | 12 617 (9.7) | 0.10 |
| Rural | 40 439 (14.4) | 20 001 (15.7) | 17 189 (13.2) | 0.07 |
| Marginalization score, mean (SD) | 3.2 (0.8) | 3.2 (0.8) | 3.2 (0.8) | 0.02 |
| ISS, median (IQR) | ||||
| Median (IQR) | 4 (4-9) | 4 (4-9) | 4 (4-9) | 0.10 |
| Category | ||||
| 1-8 | 159 030 (56.5) | 74 898 (58.8) | 70 885 (54.2) | 0.09 |
| 9-15 | 73 069 (26.0) | 31 148 (24.5) | 35 837 (27.4) | 0.07 |
| 16-24 | 25 593 (9.1) | 10 682 (8.4) | 12 816 (9.8) | 0.05 |
| 25-34 | 6289 (2.2) | 2568 (2.0) | 3228 (2.5) | 0.03 |
| 35-75 | 5292 (1.9) | 2305 (1.8) | 2584 (2.0) | 0.01 |
| Mechanism of injury | ||||
| MVC | 28 053 (10.0) | 12 780 (10.0) | 13 010 (10.0) | <0.01 |
| Fall | 190 611 (68.0) | 84 148 (66.1) | 90 351 (69.1) | 0.06 |
| Pedestrian or cyclist struck | 14 555 (5.2) | 6773 (5.3) | 6580 (5.0) | 0.01 |
| Other blunt mechanism | 34 637 (12.4) | 17 581 (13.8) | 14 331 (11.0) | 0.09 |
| Cut or pierce | 10 677 (3.8) | 5017 (3.9) | 4865 (3.7) | 0.01 |
| GSW | 1823 (0.7) | 672 (0.7) | 1016 (0.8) | 0.03 |
| Severe injury | 37 174 (13.2) | 15 555 (12.2) | 18 628 (14.3) | 0.06 |
| ACS specified injury | 67 129 (23.9) | 27 789 (21.8) | 33 830 (25.9) | 0.10 |
| Triage score | ||||
| 1 (highest acuity) | 29 802 (10.6) | 11 934 (9.4) | 15 377 (11.8) | 0.08 |
| 2 | 100 588 (35.8) | 44 435 (34.9) | 47 467 (36.3) | 0.03 |
| 3 | 128 006 (45.5) | 58 448 (45.9) | 58 999 (45.1) | 0.02 |
| 4 | 21 299 (7.6) | 11 768 (9.2) | 8038 (6.2) | 0.12 |
| 5 (lowest acuity) | 919 (0.3) | 369 (0.3) | 520 (0.4) | 0.02 |
| Time of presentation | ||||
| Weekday | 107 327 (38.2) | 48 342 (38.0) | 49 950 (38.2) | <0.01 |
| Evening or weekend | 137 634 (48.9) | 62 481 (49.1) | 63 781 (48.8) | 0.01 |
| Night | 36 307 (12.9) | 16 452 (12.9) | 16 949 (13.0) | <0.01 |
| Season | ||||
| Spring | 65 497 (23.3) | 32 047 (25.2) | 27 207 (20.8) | 0.10 |
| Summer | 75 385 (26.8) | 34 580 (27.2) | 36 148 (27.7) | 0.01 |
| Fall | 70 441 (25.0) | 30 008 (23.6) | 34 055 (26.1) | 0.06 |
| Winter | 69 945 (24.9) | 30 640 (24.1) | 33 270 (25.5) | 0.03 |
| Outcome | Rate ratio (95% CI) | ||||
|---|---|---|---|---|---|
| Baseline period | Implementation period | Postimplementation period | |||
| Rate change, per 1-y | At announcement | Annual rate change vs baseline | At full rollout | Annual rate change vs baseline | |
| Transport to a trauma center | 1.00 (0.99-1.01) | 0.96 (0.90-1.02) | 1.07 (0.97-1.19) | 1.02 (0.93-1.12) | 0.89 (0.81-0.98) |
| Undertriage | 1.01 (1.00-1.02) | 0.95 (0.89-1.01) | 1.07 (0.97-1.18) | 0.85 (0.77-0.94) | 0.95 (0.86-1.05) |
| Population-level overtriage | 1.01 (1.00-1.03) | 0.89 (0.82-0.97) | 1.18 (1.02-1.36) | 0.90 (0.79-1.04) | 0.80 (0.70-0.93) |
| Trauma center-level overtriage | 1.00 (1.00-1.01) | 0.92 (0.87-0.99) | 1.13 (1.01-1.25) | 0.86 (0.77-0.95) | 0.88 (0.79-0.98) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTrauma and Emergency Care Studies · Emergency and Acute Care Studies · Disaster Response and Management
Introduction
Severely injured patients transported directly to a trauma center are 30% less likely to die within the first 48 hours than those transported to nontrauma centers.^1^ Nonetheless, undertriage (the transportation of severely injured patients to nontrauma centers) remains common.^2,3^ Prehospital triage is challenging; there is minimal time to determine injury severity, diagnostic information is limited, and most patients have minor injuries that do not require trauma center care.^4^ National expert panels have developed field trauma triage (FTT) guidelines to help prehospital personnel identify patients likely to have severe injuries.^5,6^ While FTT criteria can accurately identify severely injured patients, how implementation of updated FTT guidelines alters triage patterns in a well-established trauma system is unknown.^7,8^
Multiple jurisdictions with long-standing FTT guidelines continue to report high rates of undertriage.^2,3,9,10,11^ Hypotheses for these high rates include a lack of geographic access to trauma centers, inadequate familiarity with triage guidelines, implicit biases related to age and gender, and limited experience in treating injured patients.^12,13,14,15,16,17^ Given that a lack of experience and implicit bias have been identified as potential drivers of undertriage, it is unclear to what extent the existence or modification of FTT guidelines can impact triage practices. In other words, it is unclear whether these guidelines increase the identification of severely injured patients or only direct emergency medical service (EMS) personnel to transport patients they already perceive as severely injured to trauma centers. To this end, the goal of this study was to analyze the association between updates to FTT guidelines and triage practices in a large, regional trauma system.
Methods
Study Design
This was a retrospective, population-based cohort study that used interrupted time series analyses to examine the association between updated FTT guidelines and triage patterns of injured adults. This study was approved by the ICES Privacy and Compliance Office with a waiver of informed consent because ICES is a prescribed entity under Personal Health Information Protection Act and the Coroners Act. This status allow ICES to conduct analyses and compile statistical information about the management and effectiveness of the health system and the health or safety of the public. This study is reported following the Reporting of Studies Conducted Using Observational Routinely Collected Data (RECORD) statement, an extension of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline developed for observational studies conducted using routinely-collected health data.^18,19^
Setting
This study was conducted in Ontario, Canada, between April 1, 2009, and March 31, 2020. Ontario is Canada’s most populous province (population, 14.6 million) and encompasses an area of 415 000 square miles (approximately 1.5 times the size of Texas). The first trauma center in Ontario was established in 1976.^20^ Currently, its regional health care system has 217 acute care hospital sites, including 9 provincially designated adult lead trauma hospitals.^12,21^ More than 80% of the population lives within 1 hour of a lead trauma hospital.^22^ Prehospital care is provided by 55 government-designated delivery agents for land ambulance and 1 air ambulance service.^23,24^ All paramedics must complete an approved training program and receive medical delegation and oversight through 1 of 7 regional base hospitals. There is 1 provincial set of paramedic practice standards, which includes provisions for FTT.^25^
Data Sources
Data were derived from administrative datasets held at ICES. Patients were identified using the National Ambulatory Care Reporting System and Discharge Abstract Database. Details of the datasets are available in eAppendix 1 in Supplement 1 and have been previously described.^1,26,27^ ICES datasets were linked using unique encoded identifiers and analyzed at ICES.
Study Participants
We identified all individuals aged at least 16 years who presented to an emergency department (ED) secondary to a traumatic injury. Traumatic injuries were identified by the presence of *International Statistical Classification of Diseases and Related Health Problems, Tenth Revision *(ICD-10) diagnosis codes in the range S1.0-T14.9. We excluded Ontario nonresidents, patients missing age, sex, or home address data, and those who left the ED without being seen or against medical advice. Additionally, we excluded patients with environmental injuries and older adults (age ≥65 years) with isolated hip fractures, as these patients are not triaged using the same guidelines as patients with other traumatic injuries. To eliminate patients who presented for sequelae of a previous injury, we excluded patients who had any injury-related ED visit in the 90 days prior to the index event or an admission for a severe injury in the prior year. To ensure that our study was not confounded by patients with minor injuries (to whom FTT criteria do not apply) we also excluded patients who either were discharged directly home from the ED of the nontrauma center to which they presented, regardless of the calculated Injury Severity Score (ISS), or, despite being transferred between nontrauma centers, did not have a severe injury and were not admitted.
Patient Characteristics
Patients were characterized by age, sex, comorbidity, frailty, receipt of long-term home care, nursing home residence, location of residence, and socioeconomic status. Adjusted Clinical Groups were used to identify comorbidity level and frailty.^28,29^ Location of residence was categorized as urban or rural based on the rural and small town definition used by Statistics Canada.^30^ Socioeconomic status was defined using the Ontario Marginalization Index.^31,32^ Injuries were characterized based on ISS, presence of a severe head, chest, or abdominal injury, mechanism of injury (MOI), date and time of presentation, and triage acuity.^33,34,35^ ISS were calculated using an validated algorithm to derive Abbreviated Injury Scale scores from ICD-10 diagnosis codes.^36^ As early deaths limit full injury ascertainment, if a patient died within 24 hours of presentation and their ISS was below 15, they were assigned to the highest ISS category. Details of all characteristics are available in eAppendix 1 in Supplement 1.
We dichotomized patients as having a severe or minor injury. If a patient had an ISS of at least 16 or died within 24 hours of presentation, they were identified as having a severe injury. All other patients were categorized as having a minor injury. We also identified patients with a high-risk injury independent of ISS. These patients included those who had a critical injury (as defined by the American College of Surgeons, as shown eAppendix 1 in Supplement 1), received mechanical ventilation in an ED, or received blood within 24 hours of presentation.^37,38^
Exposure
The exposure of interest was implementation of the 2015 update to the FTT guidelines as specified in version 2.1 of the Ontario Basic Life Support Patient Care Standards.^39^ This version of the FTT guidelines was based on the 2011 Recommendations of the National Expert Panel on Field Triage.^5^ However, the 2015 Ontario guidelines did not include ground-level falls in older adults as a special consideration for trauma center transport. Prior to the rollout of updated FTT guidelines, triage decisions were based on those included in version 2 of the provincial Basic Life Support Patient Care Standards.^40^ The new guidelines made significant changes to the physiologic, anatomic, and mechanistic criteria used to identify patients who required transport to a trauma center and added special circumstances requiring lower thresholds for transport (Table 1).
The updated FTT guidelines were announced on June 23, 2014, and all ambulance services were mandated to implement them by June 1, 2015. To facilitate implementation of the updated FTT guidelines, in June 2014, the Ministry of Health electronically published the revised FTT Standard. In a memorandum from the Director of the Emergency Health Services to the EMS chiefs, municipal chief administrative officers, and Ornge, information regarding the revised standard and expectations for dissemination and training to their personnel was outlined. To support the update, a training bulletin was drafted with information about the revised standard and how it was to be followed. The bulletin was printed by the Ministry of Health and made available to all paramedic services should they wish to distribute it to the frontline staff, or alternatively, provided in electronic format. Laminated copies of the flow diagram were also made available. Paramedic services further educated their staff using the training bulletin or through additional means, such as in-person annual continuing medical education or online modules.
Given the 1-year training and rollout period, the exposure was divided into 3 timeframes: pre-FTT (April 1, 2009, to June 30, 2014), implementation (July 1, 2014, to May 31, 2015), and postimplementation (June 1, 2015, to March 31, 2020). The decision was made to not extend the study cohort past March 2020, as the first wave of the COVID-19 pandemic started in Ontario on March 20, 2020, substantially altering hospital resource availability and triage patterns.^41^ Consequently, associations between subsequent updates to FTT guidelines, based on the 2021 Recommendations of the National Expert Panel on Field Triage, were not examined in this analysis.^6^
Outcomes
The primary outcome was presentation to a trauma center as the first treating hospital (ie, primary triage). As level III trauma centers were not formally identified in Ontario until 2021, all patients identified as presenting to a trauma center presented to a provincially designated lead trauma hospital.^42^ Patients were then classified as undertriaged or overtriaged based on injury severity. If a patient had a severe injury and was not transported to a trauma center, they were categorized as undertriaged. Conversely, if a patient had a minor injury and presented to a trauma center, they were categorized as overtriaged.
Understanding that patients with high-risk injuries who did not meet severe injury criteria could initially be managed at either a trauma or nontrauma center, all patients with high-risk injuries who survived more than 24 hours and had an ISS less than 16 were classified as appropriately triaged regardless of center of presentation. This decision was made to bias our study in favor of the EMS practitioner making the triage decision.
Statistical Analysis
Baseline characteristics were summarized using descriptive statistics and compared between patients injured before and after the implementation of FTT.^43^ To evaluate temporal trends in triage we calculated the unadjusted estimated annual percentage change (EAPC) for the rate of each outcome of interest using modified Poisson regression.^44^ Modified Poisson regression was also used to calculate the risk of each outcome in fiscal year 2019 relative to 2009.
To estimate the independent association between the update to FTT and a patient’s risk of presenting to a trauma center, we performed an interrupted time series analysis using modified Poisson regression with an autoregressive correlation structure.^45^ To account for changes in population characteristics during the study, models were adjusted for patient age; sex; comorbid status; frailty; long-term home care use; nursing home residence; rural location; socioeconomic status; MOI; ISS; presence of a severe head, chest, or abdominal injury; and time of injury. To facilitate estimation of both the instantaneous association between FTT and the risk of presentation to a trauma center as well as the association between FTT and secular trends in trauma center presentation, unique variables were included in the model to represent the exposure period (preimplementation, peri-implementation, or postimplementation) as well as the time after each exposure interval.^45^ Consequently, the final model included 3 unique segments.^46^ To account for seasonality, the model was also adjusted for the season in which the injury occurred. Likewise, given that observations that occur closer together in time tend to be more similar than those that are further apart (ie, 2 patients injured in 2010 are more likely to have similar triage decisions than a patient injured in 2010 and another injured in 2018), we used autocorrelation function plots to evaluate the correlation between observations and various lag points. Based on this evaluation, a first order autoregressive correlation structure was used for the model. Similar models were used to estimate the risk of undertriage, restricted to severely injured patients, and overtriage, restricted to patients with minor injuries. Covariates related to presence of severe injuries were excluded from the model examining overtriage. After undergoing peer review, an additional post hoc analysis was performed. For this analysis, overtriage was examined from the perspective of the trauma center. We therefore evaluated the rate at which patients with minor injuries presented to a provincially designated lead trauma hospital relative to all patients that presented to these centers. Given that covariates related to presence of severe injuries and a patient’s ISS were part of the definition of the outcome, they were excluded from this model.
To examine the robustness of our results, we performed 5 sensitivity analyses (eAppendix 2 in Supplement 1). These analyses evaluated the effect of trauma center proximity, definition of implementation period, and definition of undertriage, on the association between FTT and triage patterns.
All analysis were performed using complete cases. Data were missing for socioeconomic status in 3417 encounters (1.2%), rural location in 123 encounters (<0.1%), MOI in 912 encounters (0.3%), and triage acuity in 115 encounters (<0.1%). The ISS could not be calculated in 11 995 encounters (4.3%) of cases.
Statistical analysis was performed using SAS software version 9.4 (SAS Institute). Standardized differences greater than 0.10 and 2-sided P < .05 were considered significant.^43^ Statistical analysis was conducted from October 2023 to October 2025.
Results
During the 11-year study period, we identified 281 268 patients (mean [SD] age, 62.4 [22.5] years; 141 450 [50.3%] female; median [IQR] ISS, 4 [4-9]), including 37 174 (13.2%) with a severe injury. Most baseline characteristics were similar between patients injured before and after the implementation of new FTT guidelines (Table 2; eAppendix 3 in Supplement 1). However, patients injured after implementation were older than those injured prior to implementation.
Throughout the study, most patients initially presented to a nontrauma center (227 398 patients [80.9%]). Among 37 174 patients with a severe injury, 13 577 (36.5%) presented to a trauma center, while among 232 295 patients with a minor injury without high-risk features, 203 801 (87.7%) presented to a nontrauma center. Consequently, overall rates of undertriage and overtriage were 63.5% and 12.3%, respectively. Among 53 870 patients who presented directly to a trauma center, 28 494 (52.9%) had a minor injury without high-risk features.
Temporal Trends in Trauma Triage
Overall, the crude rate of trauma center presentation decreased by 0.4% (95% CI, 0.2%-0.7%) per year, with a patient’s likelihood of presenting to a trauma center being 7.5% lower in 2019 compared to 2009 (rate ratio [RR], 0.93; 95% CI, 0.89-0.96), (Figure 1). Likewise, rates of undertriage increased by 0.3% (95% CI, 0.1%-0.6%) per year, while rates of overtriage decreased by 0.9% (95% CI, 0.6%-1.2%) per year. Consequently, severely injured patients were 7.5% less likely and patients with minor injuries were 11.0% less likely to be transported to a trauma center in 2019 vs 2009 (severely injured: RR 0.93; 95% CI, 0.89-0.96; minor injury: RR, 0.89; 95% CI, 0.84-0.94). The rate at which patients with minor injuries presented directly to a trauma center also decreased throughout the study period (annual rate of decrease 0.7%; 95% CI, 0.5%-1.0%).
Temporal Trends in Unadjusted Rates of Transport to a Trauma Center, Undertriage, and OvertriageEAPC indicates estimated annual percent change.aRates of undertriage are relative to patients with severe injuries, rates of overtriage are relative to those with minor injuries, rates of patients with minor injuries presenting to trauma centers are relative to patients who presented to trauma centers.
Independent Association Between Updated FTT Criteria and Triage Rates
Interrupted time series analyses were used to evaluate the independent association between updated FTT guidelines and triage trends (Figure 2; eAppendix 4 in Supplement 1). Case mix–adjusted analyses demonstrated that during the 5 years prior to the implementation of FTT, the rate of patients presenting to a trauma center was constant (adjusted EAPC, 0.1%; 95% CI, −0.6% to 0.9%). Neither the announcement of FTT, the implementation period, or the final rollout were associated with a patient’s likelihood of presenting to a trauma center (Table 3). However, during the postimplementation period, the rate at which patients presented to a trauma center decreased relative to the baseline period (RR, 0.89; 95% CI, 0.81-0.98). Therefore, during the postimplementation period, case mix–adjusted rates of presentation to a trauma center decreased by 4.2% (95% CI, 3.4%-4.9%) per year.
Case-Mix Adjusted Trends in Rates of Transport to a Trauma Center, Undertriage, and OvertriageFTT indicates field trauma triageaRates of undertriage are relative to patients with severe injuries, rates of overtriage are relative to those with minor injuries, rates of patients with minor injuries presenting to trauma centers are relative to patients who presented to trauma centers.
Given that decreases in the rate at which patients presented to trauma centers could reflect either increases in undertriage or decreases in overtriage, we examined the association between updated FTT guidelines and both undertriage and overtriage. Prior to the implementation of FTT, rates of undertriage were increasing by 1.0% (95% CI, 0.2%-1.8%) per year. Again, neither the announcement of FTT nor the implementation period were associated with a patient’s risk of undertriage (Table 3). However, the final rollout of FTT was associated with an instantaneous decrease in undertriage of 15.2% (RR, 0.85; 95% CI, 0.77 to 0.94). While the implementation of FTT was associated with a significant instantaneous drop in undertriage, after this drop, the annual increase in undertriage rates observed in the baseline period resumed during the postimplementation period. Consequently, even after the implementation of FTT guidelines, case mix–adjusted rates of undertriage continued to increase by 2.4% (95% CI, 1.7% to 3.2%) per year.
Among patients with minor injuries, prior to the implementation of FTT, rates of overtriage were increasing by 1.5% (95% CI, 0.5%-2.5%) per year. Unlike the association between the announcement of FTT guidelines and rates of trauma center transport or undertriage, the announcement was associated with an instantaneous reduction in overtriage of 10.8% (RR, 0.89; 95% CI, 0.82-0.97). The instantaneous outcome after the announcement was not sustained, and the implementation period was associated with an increase in overtriage rates relative to the baseline period. While the final rollout of FTT was not associated with an instantaneous change in the risk of overtriage, the postimplementation period had a significant decrease in overtriage rates relative to the baseline period (RR, 0.80; 95% CI, 0.70-0.93). Consequently, after FTT implementation case mix–adjusted rates of overtriage decreased by 3.8% (95% CI, 2.7%-5.0%) per year.
Examination of overtriage from the perspective of trauma centers demonstrated that prior to the implementation of FTT the rate at which patients with minor injuries presented directly to trauma centers was stable (adjusted EAPC, 0.4%; 95% CI, −0.3% to 1.2%). Similar to the association between the announcement of updated FTT guidelines and population-level rates of overtriage, the announcement was associated with an instantaneous reduction in the risk of patients with minor injuries presenting directly to trauma centers (RR, 0.92; 95% CI, 0.87-0.99). Likewise, the instantaneous effect of the announcement was not sustained, and the implementation period was associated with an increase in trauma center–level overtriage rates relative to the baseline period. However, the final rollout of the updated FTT guidelines was associated both with an instantaneous decrease in the likelihood that a patient with a minor injury would present directly to a trauma center (RR, 0.86; 95% CI, 0.77 to 0.95) and a decrease in the annual rate at which patients with minor injuries presented to trauma centers (RR, 0.88; 95% CI, 0.79 to 0.98). Despite these associations, given underlying temporal trends, after the instantaneous drop in the rate at which patients with minor injuries presented to trauma centers, the overall annual case mix–adjusted rate of trauma center–level overtriage remained stable during the postimplementation phase (adjusted EAPC, −0.3%; 95% CI, −1.2% to 0.5%).
Sensitivity Analysis
Sensitivity analyses demonstrated that the association between updated FTT guidelines and triage rates was consistent regardless of trauma center proximity, definition of implementation period, or definition of undertriage (eAppendix 5 in Supplement 1). Specifically, FTT was associated with an instantaneous decrease in undertriage, and during the years after implementation, rates of overtriage decreased while rates of undertriage increased. Evaluation of the components of the expanded definition of undertriage suggested that the implementation of FTT guidelines had minimal association with undertriage rates among patients with specific clinical presentations, including those who required emergency ventilation or died early.
Discussion
In this population-based study of the implementation of the 2015 update to Ontario FTT guidelines, we found that their implementation was associated with an instantaneous decrease in the rate of undertriage of 15% without a commensurate increase in overtriage. However, this reduction was not sustained. During the 5 years after the rollout of FTT, rates of undertriage increased by 2% annually. These findings suggest that while FTT was associated with decreasing undertriage without increasing overtriage, ongoing monitoring of triage practices is essential to ensure the benefits associated with FTT are maintained.
Our findings are consistent with the literature demonstrating that FTT can identify a significant proportion of severely injured patients.^7,8^ Moreover, our results address the concern that the implementation of FTT will result in unsustainable increases in overtriage.^47,48^ Contrary to these concerns, we demonstrated that updates to FTT guidelines were associated with decreasing rates of overtriage. However, we also found that despite an initial decrease in rates of undertriage, underlying trends in triage of severely injured patients remained unchanged. Consequently, rates of undertriage increased during the years after the implementation of FTT.
Current initiatives to reduce undertriage focus on refining FTT criteria.^6^ Our findings suggest that the ability of FTT criteria to identify severe injuries is not the primary driver of ongoing high rates of undertriage. While we did not have access to paramedic documentation to determine specific drivers of undertriage (ie, inappropriate application of FTT guidelines vs criteria not identifying patients with severe injuries), given the initial decrease it undertriage associated with the update to FTT, it is unlikely that failure of the guidelines to identify severely injured patients was the primary driver of subsequent increases in undertriage during the years after implementation. Rather, this finding highlights an alternative target for interventions to reduce undertriage: longitudinal feedback aimed at sustaining reductions in undertriage. It is possible that the structured training related to the implementation of FTT played a substantial role in the initial decrease in undertriage associated with these guidelines. Conversely, as clinicians became further removed from these sessions they may have returned to their previous triage practices, practices based on heuristics and pattern recognition.^17,49^ In other words, while clinicians still knew to transport severely injured patients to trauma centers, they reverted to the practice of transporting patients they perceived as severely injured rather than those flagged by guidelines. The challenge in translating clinical guidelines to the bedside is not unique to prehospital medicine. Evaluation of implementation strategies in cardiac care have demonstrated the key role of implementation sciences and benefit of audit and feedback mechanisms.^50,51^
Limitations
There are important limitations to consider when interpreting the results of this study. First, due to data limitations, we could not determine method of transportation to hospital. It is likely that a portion of patients included in this study self-presented; therefore, FTT guidelines would have no effect on their hospital of presentation. As it is unlikely that methods of transport to hospital systematically varied during the study period, the associations demonstrated in study are likely robust to this limitation. Second, the identification of injury severity was based on administrative data. While the algorithm used in this study has been validated and is highly accurate, it is biased to underestimate injury severity.^36^ It is therefore likely that we underestimated the rate of undertriage. However, the same algorithm was applied across the study making it unlikely that underestimation of injury severity biased our results. Likewise, to limit the potential of inappropriately classifying patients with minor injuries as having severe injuries, we excluded all patients discharged home from the ED of the initial nontrauma center regardless of calculated ISS. We therefore biased our study in favor of the decision made by the treating clinicians and minimized estimated undertriage rates. Third, it is possible that residual confounding related to triage decisions remained. Administrative data does not include details related to hemodynamic status or level of consciousness. It is possible that some patients identified as overtriaged met physiologic criteria for trauma center presentation. To overcome this limitation, we extracted data related to ventilation and blood transfusion. These variables were used as surrogates for clinical status and used to limit the identification of patients as overtriaged. Consequently, it is unlikely that misclassification existed to a significant enough extent to alter the findings of our analysis. A fourth limitation is the inclusion of all injured patients regardless of location. Given the size of Ontario, 10% of the population does not have ready access to a provincially designated lead trauma hospital.^22^ FTT cannot alter the rate at which these patients are transported to a trauma center. To ensure inclusion of remote patients did not obscure the impact of FTT, we performed a sensitivity analysis restricted to patients whose destination hospital could most easily be impacted by EMS personnel. The results of this analysis remained consistent with the primary analysis. A fifth limitation is the scope of our study. We focused our analysis on the association between the update to FTT guidelines and triage accuracy. While our findings suggest that longitudinal audit and feedback mechanisms may be essential in maintaining improvements in triage accuracy associated with updates to FTT guidelines, guideline adherence is only a small piece of the puzzle. Rather, there are numerous potential causes of undertriage, including geographic barriers, implicit bias, and reliance on pattern recognition.^12,13,14,15,16,17^ Future research is essential in identifying strategies to ensure that all patients have optimal access to resources commensurate with their illness severity. Sixth, our analysis focused on the association between a 2015 update to the FTT guidelines based on recommendations from the 2011 National Expert Panel. In 2021, FTT guidelines were further updated with a focus on reducing undertriage.^6^ While ideally the implementation of these guidelines has further reduced undertriage within trauma systems, it is likely that the findings of our study still apply. That is, undertriage rates are likely to drop with initial implementation, but over time clinicians may revert to their baseline triage practices. Finally, because this study was centered around FTT guidelines, this study focuses only on primary triage (ie, triage by EMS in the field). This study does not assess the proportion of patients who eventually receive trauma center treatment thanks to interfacility transfer.
Conclusions
The findings of this cohort study suggest that updates to FTT guidelines were associated with a transient decrease in undertriage without a commensurate increase in overtriage. However, their implementation was not associated with a difference in underlying trends related to the triage of severely injured patients. Consequently, during the years after implementation, undertriage rates gradually increased. These findings support the use of FTT to improve access to trauma care and highlight the need for ongoing monitoring of triage practices to ensure the benefits of novel interventions are preserved.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Haas B, Stukel TA, Gomez D, . The mortality benefit of direct trauma center transport in a regional trauma system: a population-based analysis. J Trauma Acute Care Surg. 2012;72(6):1510-1515. doi:10.1097/TA.0b 013e 318252510 a 22695414 · doi ↗ · pubmed ↗
- 2Xiang H, Wheeler KK, Groner JI, Shi J, Haley KJ. Undertriage of major trauma patients in the US emergency departments. Am J Emerg Med. 2014;32(9):997-1004. doi:10.1016/j.ajem.2014.05.03824993680 · doi ↗ · pubmed ↗
- 3Voskens FJ, van Rein EAJ, van der Sluijs R, . Accuracy of prehospital triage in selecting severely injured trauma patients. JAMA Surg. 2018;153(4):322-327. doi:10.1001/jamasurg.2017.447229094144 PMC 5933379 · doi ↗ · pubmed ↗
- 4Mac Kenzie EJ, Rivara FP, Jurkovich GJ, . A national evaluation of the effect of trauma-center care on mortality. N Engl J Med. 2006;354(4):366-378. doi:10.1056/NEJ Msa 05204916436768 · doi ↗ · pubmed ↗
- 5Sasser SM, Hunt RC, Faul M, ; Centers for Disease Control and Prevention (CDC). Guidelines for field triage of injured patients: recommendations of the National Expert Panel on Field Triage, 2011. MMWR Recomm Rep. 2012;61(RR-1):1-20.22237112 · pubmed ↗
- 6Newgard CD, Fischer PE, Gestring M, ; Writing Group for the 2021 National Expert Panel on Field Triage. National guideline for the field triage of injured patients: Recommendations of the National Expert Panel on Field Triage, 2021. J Trauma Acute Care Surg. 2022;93(2):e 49-e 60. doi:10.1097/TA.000000000000362735475939 PMC 9323557 · doi ↗ · pubmed ↗
- 7Newgard CD, Rudser K, Hedges JR, ; ROC Investigators. A critical assessment of the out-of-hospital trauma triage guidelines for physiologic abnormality. J Trauma. 2010;68(2):452-462. doi:10.1097/TA.0b 013e 3181 ae 20c 920154558 PMC 3785297 · doi ↗ · pubmed ↗
- 8Newgard CD, Hsia RY, Mann NC, ; Western Emergency Services Translational Research Network (WESTRN) Investigators. The trade-offs in field trauma triage: a multiregion assessment of accuracy metrics and volume shifts associated with different triage strategies. J Trauma Acute Care Surg. 2013;74(5):1298-1306. doi:10.1097/TA.0b 013e 31828 b 784823609282 PMC 3726266 · doi ↗ · pubmed ↗