Telehealth vs In-Person Outpatient Mental Health Service Use and Spending Among Medicare Beneficiaries From 2019 to 2023
Ryan K. McBain, Jonathan Cantor, Rose Kerber, Cheryl L. Damberg, Christopher M. Whaley

TL;DR
The study compares telehealth and in-person mental health service use and spending for several conditions among Medicare beneficiaries from 2019 to 2023.
Contribution
The study provides new insights into how telehealth use and spending changed for mental health conditions during and after the pandemic.
Findings
Telehealth utilization increased during the pandemic for mental health conditions.
Spending patterns shifted toward telehealth services during the pandemic.
Post-pandemic trends show a partial return to in-person services.
Abstract
This cross-sectional study identifies patterns of telehealth utilization and spending for anxiety, depression, bipolar disorder, schizophrenia, and posttraumatic stress disorder before, during, and after the COVID-19 pandemic among Medicare fee-for-service beneficiaries.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure
Figure| Diagnostic category | Prepandemic period | Pandemic periodb | Postpandemic periodb | |||
|---|---|---|---|---|---|---|
| β-Coefficient (95% CI) | β-Coefficient (95% CI) | β-Coefficient (95% CI) | ||||
|
| ||||||
| Depression | ||||||
| In-person | 3354.5 (3488.4 to 3580.6) | <.001 | −1672.6 (−1848.4 to −1496.9) | <.001 | 241.7 (65.4 to 417.9) | .008 |
| Telehealth | 81.5 (79.2 to 83.7) | <.001 | 2179.1 (2005.4 to 2352.7) | <.001 | −734.7 (−997.3 to −472.1) | <.001 |
| Anxiety | ||||||
| In-person | 2361.1 (2343.5 to 2378.8) | <.001 | −824.1 (−887.4 to −760.8) | <.001 | 205.1 (98.9 to 311.4) | <.001 |
| Telehealth | 31.6 (29.5 to 33.8) | <.001 | 1369.2 (1205.0 to 1533.5) | <.001 | −439.4 (−630.0 to −248.8) | <.001 |
| Bipolar disorder | ||||||
| In-person | 1174.5 (1138.0 to 1211.0) | <.001 | −650.2 (−751.9 to −548.6) | <.001 | −1.2 (−75.4 to 73.0) | .97 |
| Telehealth | 36.7 (36.2 to 37.2) | <.001 | 839.0 (779.2 to 898.8) | <.001 | −309.0 (−423.6 to −194.4) | <.001 |
| Schizophrenia | ||||||
| In person | 511.2 (500.4 to 521.9) | <.001 | −254.3 (−294.1 to −214.5) | <.001 | 16.4 (−14.6 to 47.4) | .30 |
| Telehealth | 25.3 (25.1 to 25.6) | <.001 | 329.7 (305.3 to 354.0) | <.001 | −138.3 (−188.7 to −88.0) | <.001 |
| PTSD | ||||||
| In person | 1257.9 (1243.1 to 1272.7) | <.001 | −674.4 (−740.3 to −608.5) | <.001 | 135.6 (42.8 to 228.4) | .005 |
| Telehealth | 18.4 (16.5 to 20.3) | <.001 | 967.8 (911.9 to 1023.6) | <.001 | −222.5 (−296.5 to −148.6) | <.001 |
| Total | ||||||
| In person | 8839.2 (8736.7 to 8941.7) | <.001 | −4075.7 (−4511.7 to −3639.6) | <.001 | 597.6 (155.3 to 1039.8) | .009 |
| Telehealth | 193.5 (186.8 to 200.3) | <.001 | 5684.7 (5220.2 to 6149.2) | <.001 | −1844.0 (−2515.8 to −1172.2) | <.001 |
|
| ||||||
| Depression | ||||||
| In person | 28 777.5 (27 038.0 to 30 517.1) | <.001 | 1252.1 (−485.6 to 2989.9) | .16 | 331.5 (−826.5 to 1489.6) | .57 |
| Telehealth | 424.4 (395.7 to 453.0) | <.001 | 5692.2 (5126.9 to 6257.5) | <.001 | −1462.4 (−2055.7 to −869.1) | <.001 |
| Anxiety | ||||||
| In person | 18 265.2 (16 891.4 to 19 369.0) | <.001 | 3022.4 (1428.7 to 4616.1) | <.001 | 805.2 (−511.9 to 2122.3) | .23 |
| Telehealth | 179.2 (167.8 to 190.7) | <.001 | 2909.5 (2621.7 to 3197.2) | <.001 | −364.8 (−697.2 to −32.4) | .03 |
| Bipolar disorder | ||||||
| In person | 8421.1 (7858.8 to 8983.3) | <.001 | 64.3 (−510.9 to 639.6) | .83 | −993.6 (−1534.6 to −452.7) | <.001 |
| Telehealth | 161.6 (149.2 to 174.0) | <.001 | 2108.8 (1908.7 to 2309.0) | <.001 | −646.5 (−875.5 to −417.5) | <.001 |
| Schizophrenia | ||||||
| In person | 3179.5 (2950.3 to 3408.7) | <.001 | −11.3 (−238.7 to −216.2) | <.001 | −264.6 (−423.6 to −105.6) | .002 |
| Telehealth | 109.5 (100.2 to 118.8) | <.001 | 801.0 (730.5 to 871.5) | <.001 | −286.4 (−375.5 to −197.4) | <.001 |
| PTSD | ||||||
| In-person | 11 493.5 (10 772.8 to 12 214.1) | <.001 | 865.9 (175.0 to 1566.9) | .02 | 168.5 (−334.8 to 671.7) | .51 |
| Telehealth | 97.8 (85.1 to 110.6) | <.001 | 3188.5 (2948.0 to 3428.9) | <.001 | −497.4 (−769.0 to −225.7) | <.001 |
| Total | ||||||
| In person | 70 136.8 (65 588.7 to 74 684.9) | <.001 | 5193.5 (607.8 to 9779.3) | .03 | 47.0 (−2788.7 to 2882.7) | .97 |
| Telehealth | 972.5 (901.6 to 1043.5) | <.001 | 14 700.0 (13 343.4 to 16 056.6) | <.001 | −3257.5 (−4670.7 to −1844.2) | <.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTelemedicine and Telehealth Implementation · COVID-19 and Mental Health · Digital Mental Health Interventions
Introduction
During the COVID-19 pandemic, the Centers for Medicare & Medicaid Services relaxed restrictions on telehealth services, leading to rapid expansion of telehealth use for mental health care.^1^ Although postpandemic patterns are documented for commercially insured populations,^2^ little is known about Medicare fee-for-service (FFS) beneficiaries,^3^ who represent a substantial share of mental health care users. To fill the gap, we examined monthly telehealth and in-person outpatient mental health service utilization and spending rates among FFS beneficiaries. We focused on 5 major diagnostic categories representing approximately 75% of assigned diagnoses for individuals meeting criteria for any mental disorder.^4^
Methods
We conducted a retrospective analysis of all Medicare FFS beneficiaries with any mental health–related outpatient visits from any clinician between January 1, 2019, and December 31, 2023. Data were drawn from FFS carrier claims and restricted by using outpatient and telehealth place-of-service codes 02, 10, 11, 22, 23. The Brown University IRB deemed this cross-sectional study exempt from review and waived informed consent because deidentified, secondary data were used. We followed the STROBE reporting guideline.
Diagnoses were defined using International Statistical Classification of Diseases and Related Health Problems, Tenth Revision codes for anxiety disorders (F41), depressive disorders (F32, F33), bipolar spectrum disorders (F31), schizophrenia spectrum disorders (F25), and posttraumatic stress disorder (F43). Claims were included if a relevant diagnosis appeared as the primary or secondary; when both diagnoses were eligible, the primary was assigned. Data were segmented into (COVID-19) prepandemic (January 2019-February 2020), acute pandemic (March-December 2020; before vaccine access), and postpandemic (January 2021-December 2023) periods.
We estimated condition-specific trends using segmented ordinary least squares linear regression. Primary specification regressed outcomes (monthly claims rates per 100 000 beneficiaries; monthly spend rates [2023 dollars] per 10 000 beneficiaries) on indicators for pandemic and postpandemic periods, with intercepts representing prepandemic monthly rates. To accommodate serial correlation, we used Newey-West SEs with a 12-month bandwidth. In the sensitivity analysis, we adjusted for seasonality using month-of-year fixed effects.
Two-sided P < .05 indicated statistical significance. Analyses were completed in Stata 18 (StataCorp).
Results
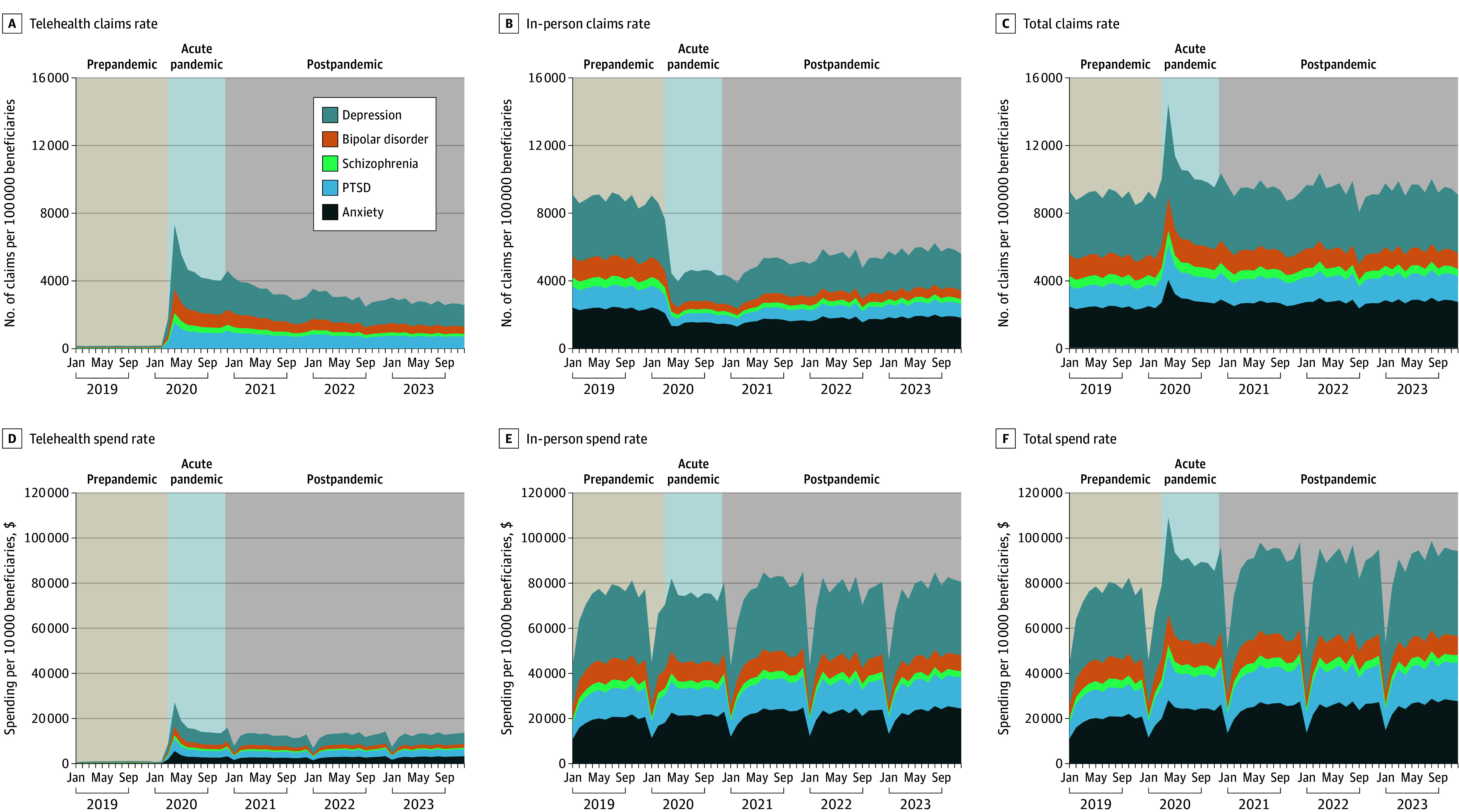
We included 9 548 926 beneficiaries (6 388 231 females [66.9%]), representing $8.1 billion in spending. Before the pandemic, telehealth comprised 2.1% of outpatient mental health claims. This rate increased to 54.4% (P < .001) during the pandemic then declined to 42.9% (P < .001) after the pandemic. The pattern was consistent across diagnostic categories (eg, for depression, telehealth represented 2.4% of claims before, 57.3% during, and 44.2% after the pandemic) (Table). Modeled estimates showed total mental health claims remained stable over time, averaging 9033 claims per 100 000 beneficiaries per month during the prepandemic, 10 642 during the pandemic, and 9395 during the postpandemic periods (Figure).
Telehealth and In-Person Outpatient Mental Health Service Claims and Spend Rates Among Medicare Fee-for-Service Beneficiaries From 2019 to 2023Pre–(COVID-19) pandemic period extended from January 2019 to February 2020; acute pandemic extended from March to December 2020, and postpandemic period extended from January 2021 to December 2023. PTSD indicates posttraumatic stress disorder.
Estimates indicated outpatient mental health spending increased during the pandemic from 91 003 per 10 000 beneficiaries per month (P < .001). Spending remained elevated (973 to 12 415 after the pandemic.
Discussion
This study characterized trends in outpatient mental health care among FFS beneficiaries over a 5-year period of unprecedented health care disruptions. Before the pandemic, only 2.1% of services were delivered via telehealth. After the pandemic, this share was 42.9%. Nevertheless, total service utilization remained stable, suggesting telehealth visits have been largely substitutionary.^5^ Meanwhile, spending increased by 11%. Alongside prior studies,^2,6^ these findings indicate mental health telehealth has become a durable care component among beneficiaries.
Study limitations include, first, a Medicare FFS focus. Medicare Advantage enrollees differ in demographic and clinical backgrounds and may exhibit divergent service patterns. Second, we did not assess clinical outcomes or disaggregate findings by older and younger cohorts. Third, alternatively defined time frames for pandemic analysis could alter reported estimates. Lastly, study inclusion depended on recorded outpatient service and primary or secondary diagnosis in carrier claims.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Centers for Medicare & Medicaid Services. Calendar Year (CY) 2022 Medicare physician fee schedule final rule. November 2, 2021. Accessed May 25, 2025. https://www.cms.gov/newsroom/fact-sheets/calendar-year-cy-2022-medicare-physician-fee-schedule-final-rule
- 2Mc Bain RK, Cantor J, Pera MF, Breslau J, Bravata DM, Whaley CM. Mental health service utilization rates among commercially insured adults in the US during the first year of the COVID-19 pandemic. JAMA Health Forum. 2023;4(1):e 224936. doi:10.1001/jamahealthforum.2022.493636607697 PMC 9857246 · doi ↗ · pubmed ↗
- 3Mehrotra A, Busch AB, Uscher-Pines L, Raja P, Huskamp HA. In-person visits before initiation of telemedicine for mental illness. JAMA Health Forum. 2024;5(4):e 240234. doi:10.1001/jamahealthforum.2024.023438578629 PMC 10998149 · doi ↗ · pubmed ↗
- 4Fan Y, Fan A, Yang Z, Fan D. Global burden of mental disorders in 204 countries and territories, 1990-2021: results from the Global Burden of Disease Study 2021. BMC Psychiatry. 2025;25(1):486. doi:10.1186/s 12888-025-06932-y 40375174 PMC 12080068 · doi ↗ · pubmed ↗
- 5Cao YJ, Chen D, Smith M. Use telehealth as needed: telehealth substitutes in-person primary care and associates with the changes in unplanned events and follow-up visits. BMC Health Serv Res. 2023;23(1):426. doi:10.1186/s 12913-023-09445-037138327 PMC 10154749 · doi ↗ · pubmed ↗
- 6Cantor JH, Mc Bain RK, Ho PC, Bravata DM, Whaley C. Telehealth and in-person mental health service utilization and spending, 2019 to 2022. JAMA Health Forum. 2023;4(8):e 232645. doi:10.1001/jamahealthforum.2023.264537624614 PMC 10457709 · doi ↗ · pubmed ↗