Addressing mental and physical fatigue in major abdominal surgery by incorporating muscle stretches and hydration mini breaks
J Franklyn, V Sharma, SS Reddy, H Kaur, D Wildash, J Bell, SP Dayal, A Tzivanakis, F Mohamed, BJ Moran, T Cecil

TL;DR
This study shows that short hydration and stretch breaks during long abdominal surgeries can reduce fatigue and improve wellbeing for theatre staff.
Contribution
The novel approach of incorporating hydration and muscle stretch breaks during major abdominal surgeries to mitigate fatigue is evaluated for the first time.
Findings
Over half of participants reported surgical discomfort affecting stamina, posture, and concentration.
Participants with breaks reported lower pain scores and improved mental and situational fatigue metrics.
Regular breaks improved work-life balance and reduced stress for theatre personnel.
Abstract
The purpose of this quality improvement project (QIP) was to identify factors contributing to mental and physical fatigue in major abdominal surgery and to attempt to mitigate the same by incorporating mini hydration breaks with targeted muscle stretches at regular intervals. This prospective QIP was conducted in the Peritoneal Malignancy Unit of a national referral centre for peritoneal malignancy-related diseases between February and April 2022. Only procedures lasting longer than four hours were included and all theatre personnel were invited to participate. A baseline survey was conducted to ascertain the impact of mental and physical fatigue. Subsequently, a cross-over study design was utilised; for the first four weeks the procedure was performed with no breaks. This was followed with four weeks of intervention (hydration breaks and muscle stretches). Validated questionnaires…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
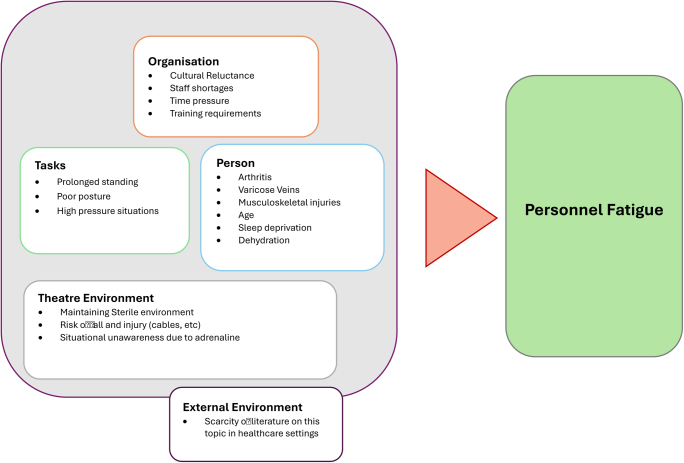 Figure 1
Figure 1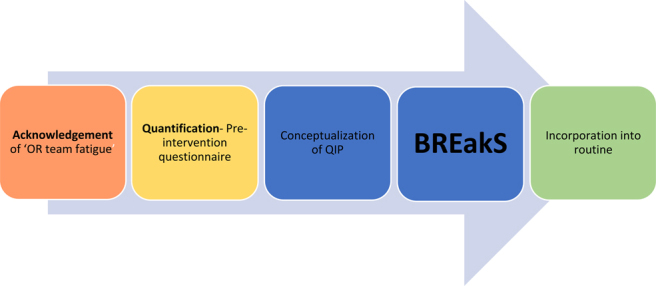 Figure 2
Figure 2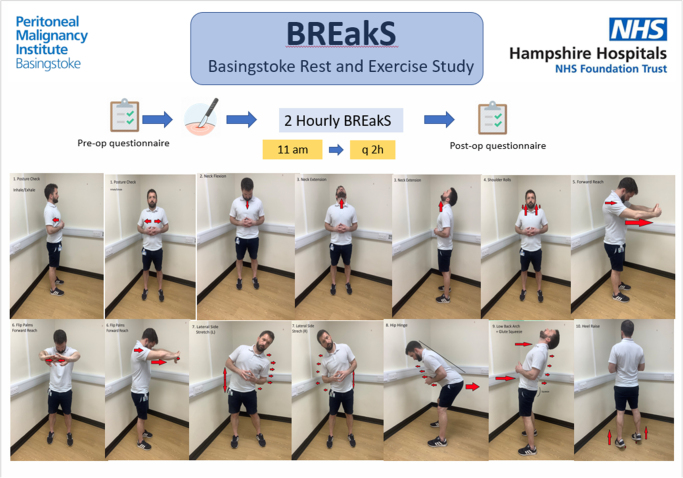 Figure 3
Figure 3| Number (%) | |
|---|---|
| Job title | |
| Consultant surgeon | 8(23.5) |
| Anaesthetic Consultant | 3(8.8) |
| Registrar/Fellow | 11(32.5) |
| Theatre nurse | 8(23.5) |
| SHO | 3(8.8) |
| ODP | 1(2.9) |
| Age | |
| <30 years | 2(5.9) |
| 30–40 years | 14(41.2) |
| 40–50 years | 13(38.2) |
| 50–60 years | 3(8.8) |
| 60+ years | 2(5.9) |
| Theatre experience in years | |
| <5 | 6(17.6) |
| 5–10 | 5(14.7) |
| 10–20 | 15(44.1) |
| 20+ | 8(23.5) |
| Pre-existing MSK problem | |
| Yes | 8(23.5) |
| No | 24(70.6) |
| Prefer not to say | 2(5.9) |
| Has surgical discomfort affected the following | |
| Balance | 6(17.6) |
| Concentration | 12(35.4) |
| Mobility | 8(23.5) |
| Object localisation | 2(5.9) |
| Posture | 20(58.8) |
| Stamina | 11(32.4) |
| Pain | 4(11.8) |
| How do you think operative fatigue affects you? | |
| Adversely affects work/life balance | 15(44.1) |
| Alters sleeping pattern | 6(17.6) |
| I have considered shortening/changing career | 4(11.8) |
| Pain | 3(8.8) |
| How often do you have muscle/joint pain at the end of the procedure? | |
| Every time I operate | 3(8.8) |
| Once a month | 17(50) |
| Once a week | 8(23.5) |
| Rarely | 4(11.8) |
| Never | 2(5.9) |
| Do you feel dehydrated and drained at the end of an operating session? | |
| Yes | 16(47.1) |
| No | 4(11.8) |
| Maybe/depends on the case | 14(41.2) |
| How do you deal with operative discomfort? | Taking a break | 10(29.4) |
| Ignore it | 16(47.1) | |
| Change operative/patient position | 9(26.5) | |
| Build general fitness by exercising outside of work | 21(61.8) | |
| Other | 4(11.8) | |
| Do you routinely implement risk reducing strategies in the OT to alleviate musculoskeletal issues? e.g. stretching, taking breaks, etc | Yes | 8(23.5) |
| No | 19(55.9) | |
| Occasionally | 7(20.6) | |
| Do you routinely stretch or exercise muscle groups outside the context of work in a gym or at home? | Yes | 18(52.9) |
| No | 9(26.5) | |
| Rarely | 7(20.6) |
| Body parts | Difference in Mean pain score before breaks (Post op–Pre op=difference) | Mean pain score after breaks (Post op–Pre op=difference) | Improvement |
|---|---|---|---|
| Neck | 2.66–1.48=1.18 | 1.98–1.67=0.31 | 0.87 |
| Shoulder | 2.75–1.67=1.08 | 2.09–1.66=0.43 | 0.65 |
| Upper back | 2.54–1.37=1.17 | 2.42–1.84=0.58 | 0.59 |
| Lower back | 3.24–2.00=1.24 | 2.53–2.01=0.52 | 0.72 |
| Arms | 2.06–1.20=0.86 | 1.65–1.37=0.28 | 0.58 |
| Wrists | 2.15–1.29=0.86 | 1.94–1.55=0.39 | 0.47 |
| Knees | 3.38–1.90=1.48 | 2.27–1.79=0.48 | 1.00 |
| Ankle | 3.13–1.70=1.43 | 2.37–1.62=0.75 | 0.68 |
| Mean pain score | 2.61–1.58=1.03 | 2.16–1.68=0.46 | 0.57 |
| Surgical task load measure (n=88) | Before breaks mean | After breaks mean | Difference |
|---|---|---|---|
| Mental demand | 4.51 | 3.90 | 0.61 |
| Physical demand | 4.76 | 3.90 | 0.86 |
| Temporal demand | 3.70 | 2.94 | 0.76 |
| Task complexity | 5.41 | 4.37 | 1.04 |
| Situational stress | 3.48 | 2.50 | 0.98 |
| Distracted | 3.5 | 2.69 | 0.81 |
| Parameters | Pre-intervention | Post-intervention | Difference | |
|---|---|---|---|---|
| Physical exertion | Palpitations | 0.40 | 0.17 | 0.23 |
| Lack of concern | 0.76 | 0.44 | 0.32 | |
| Sweaty | 0.62 | 1.16 | −0.54 | |
| Physical discomfort | Tense muscles | 1.66 | 1.57 | 0.11 |
| Numbness | 0.91 | 0.45 | 0.46 | |
| Stiff joints | 1.44 | 1.20 | 0.24 | |
| Aching | 2.00 | 1.64 | 0.36 | |
| Sleepiness | Falling asleep | 0.61 | 0.42 | 0.19 |
| Drowsy | 0.83 | 0.42 | 0.41 | |
| Yawning | 1.14 | 0.73 | 0.41 | |
| Lack of motivation | Lack of concern | 0.75 | 0.37 | 0.38 |
| Passive | 0.89 | 0.34 | 0.55 | |
| Uninterested | 0.65 | 0.34 | 0.31 | |
| Lack of energy | Worn out | 1.61 | 1.23 | 0.38 |
| Over-worked | 1.41 | 0.95 | 0.46 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMusculoskeletal pain and rehabilitation · Healthcare professionals’ stress and burnout · Cardiac, Anesthesia and Surgical Outcomes
Introduction
Theatre personnel working long hours without regular breaks are likely to be tired, inattentive, dehydrated and ultimately less vigilant.^1^ In addition, performing long operations without mitigation measures can lead to musculoskeletal injury, adversely affect work–life balance and potentially shorten careers.^2^
Recognition of the importance of workplace fatigue, regular hydration and rest breaks has been enshrined in the work culture of workers in the airline industry and professional lorry drivers with reported beneficial results.^3–5^ There is a growing body of evidence encouraging the adoption of rest breaks in the operating theatre; however, for a plethora of reasons ranging from surgical culture to lack of awareness, rest breaks have not been established in standard operating procedure protocols. A recent multi-centred cohort study has also suggested that performing targeted muscle stretches at periodic intervals intraoperatively can decrease musculoskeletal pain.^6^
Whereas most studies have looked at mandatory operative breaks from either the surgical or anaesthetic perspective, this paper explores the impact of incorporating hydration breaks on a global level for the entire theatre team performing complex abdominal surgery.
The purpose of this quality improvement project (QIP) was to identify the factors contributing to mental and physical fatigue in major abdominal surgery and to attempt to mitigate mental and physical fatigue by incorporating mini hydration breaks with targeted muscle stretches at regular intervals during major surgery.
Methods
Design and setting
This prospective, single-centre QIP was conducted in the Peritoneal Malignancy Unit of a national referral centre for peritoneal malignancy-related diseases between February and April 2022 after obtaining permission from the research and development department. All patients underwent cytoreductive surgery and hyperthermic intra-peritoneal chemotherapy (CRS and HIPEC). Since most procedures last a median of eight hours, two consultant surgeons are assigned for each procedure with a recommended lunch break for all theatre personnel.
Eligible participants included all theatre personnel involved in peritoneal malignancy operative procedures. Unlike earlier studies where the duration of surgery was heterogeneous, in this study only procedures likely to last longer than four hours were included.
A cross-over study design was utilised, wherein, for the first four weeks, the operative procedure was performed with no breaks. This was followed with four weeks of intervention (hydration breaks and muscle stretches). Both control and intervention weeks had pre- and post-procedure validated questionnaires to objectively measure physical and mental fatigue as well as surgical task load.
Initial questionnaire and baseline phase
Theatre personnel completed an initial questionnaire (Appendix 1) via an online form to understand the extent of their physical and mental fatigue, along with suggestions to mitigate fatigue. The results of this questionnaire were analysed and a literature review carried out to find the most suitable intervention (Table 1 and 2). Based on the results of the initial questionnaire and the literature review, a root cause analysis was performed using the system engineered initiative for patient safety (SEIPS) conceptual model and a decision was made to proceed with the QIP (Figures 1 and 2).^7^
SEIPS conceptual model to perform a root cause analysis of theatre personnel fatigue. SIEPS = System engineered initiative for patient safety
Flowchart of study from inception to incorporation into theatre routine BREakS = Basingstoke Rest and Exercise Study; OR = operating room; QIP = quality improvement project
Control month 1—no breaks or exercises
During the first month, all procedures were carried out without any mandatory breaks for water or exercises. Pre- and post-procedure pain scores, the surgical task load index (SURG-TLX) and the Swedish occupational fatigue inventory (SOFI) were used to objectify the results (Table 3).
Intervention month 2—intervention month with breaks for water and exercise twice during the operation
The exercise breaks were designed with the local physiotherapy team and were based on the exercises discussed by Park et al.^15^ The routine was designed to be adequately short, with just over a minute required for the entire sequence and in a manner to ensure sterility of scrubbed theatre personnel, i.e. hands visible always, enough space between people. The routine was simplified and made memorable and not distracting by ensuring the routine went from head down to toes. To avoid slippage on any potentially wet theatre surface, the exercise routine ensured both feet on ground for greater stability of the participants.
A demonstrative video was created and circulated to all theatre personnel before the intervention weeks to allow them to familiarise themselves with the exercises (Supplemental video 1). Numerous posters were also placed on the wall of the theatre to allow staff to follow the routine even without the physiotherapy team leading the break.
After the exercise break, a hydration break was also taken and all theatre personnel were encouraged to drink water from a sealed cup using a straw. The total duration of these short breaks was around two minutes. Breaks were held approximately twice during a surgical procedure, with the first break taken around two hours into the operation. The breaks were coordinated by the consultant and fellow in the theatre and repeated in approximately two hours when patient safety permitted (Figure 3).
Schematic poster showing BREakS exercise sequence BREakS = Basingstoke Rest and Exercise Study
Assessment tools
All theatre personnel participating in these procedures completed pain scores pre- and post-operatively (Appendix 1). The mean difference in pain scores (pre-operative MSK pain and post-procedure MSK pain) was compiled. The mean difference in pain score between the two arms of the study, i.e. control and intervention arm, was analysed.
In addition, all participants completed the following questionnaires post-operatively:
- • SURG-TLX, which assesses the impact of stress on the perceived demands of surgeons and other theatre personnel in completing a surgical task^8^;
- • SOFI, a tool that assesses work-related fatigue under five domains (sleepiness, lack of motivation, physical discomfort, physical exertion and lack of energy), with each of these domains having five questions.^9^ These two questionnaires were filled in only at the end of the operating day and the changes in scores were compared between the two arms (control and intervention).
The forms were made available in print form in the operating room and all theatre staff were encouraged to fill the pre-operative section before the procedure began and the post-operative section at the end. This was reinforced by including a reminder in the World Health Organisation check-in and check-out. All forms were submitted at the end of the day into a confidential box (Appendix 2).
Data analysis
All results were analysed using SPSS (IBM Corp. Released 2016. IBM SPSS Statistics for Windows, Version 24.0. Armonk, NY: IBM Corp.). The average change in pain from pre- to post-operation was calculated for all body parts. As the raw data were normally distributed, an independent t-test was used to calculate whether the difference from control weeks to intervention weeks was statistically significant. Independent t-tests were also used for calculating significance in change in average SOFI scores for each measure as well as for surgical task load measures. For all analysis a p-value less than 0.05 was considered statistically significant.
Results
Baseline survey of theatre personnel
A total of 34 theatre personnel completed the questionnaire that assessed the baseline mental and physical wellbeing. Most participants were in their 40s with at least ten years of operating theatre experience. The physical and mental effect of performing complex surgery along with its effect on work–life balance is outlined in Table 1. The strategies employed by theatre personnel to deal with surgical fatigue are depicted in Table 2.
Impact of hydration breaks and muscle stretches
A total of 41 operations were performed, 20 procedures without breaks and 21 with BREakS (Basingstoke Rest and Exercise Study). The procedures lasted a median of seven hours (range 4.5–11h). The median operative time was similar between the two groups. The results of this project suggest that there were global improvements in musculoskeletal discomfort after structured breaks were introduced. Most practitioners perceived an improvement in their mental focus and felt less distractible as reflected by the improvement in surgical task load index (Table 4).
The SOFI reports a multi-dimensional assessment of procedure-related fatigue. Table 5 represents an improvement in the overall fatigue levels of the theatre personnel.
Discussion
The results of this study bring to attention the levels of stress theatre personnel endure in pursuit of optimal patient care. The baseline questionnaire that was sent out to all theatre personnel revealed that 47% felt dehydrated at the end of the procedure, with musculoskeletal discomfort affecting their posture, stamina and ability to concentrate. Most respondents felt that operative fatigue and musculoskeletal pain affected their work–life balance and sleep pattern, with 11% considering shortening their careers due to these factors. These findings are amplified by the fact that most (55%) theatre personnel do not implement any risk-reducing strategies and 48% of respondents did not stretch or regularly exercise outside of work. Most theatre personnel do not take a break when they have discomfort, and rarely stretch or exercise consciously, due partly due to surgical culture and partly to lack of awareness.^10^
Workplace fatigue has contributed to multiple tragedies ranging from the Chernobyl nuclear disaster to the Spuyten-Duyvil rail derailment.^9,11,12^ Although these may be extreme examples, an exhausted workforce can undoubtedly lead to medical errors.^13^ The findings of the preliminary survey have been echoed by various authors previously.^14,15^ However, most studies have focused on either surgeons or anaesthetists. The results of this study are unique as the focus is on the wellbeing of all theatre personnel, in particular the operating department practitioners and nurses, who are equally affected by fatigue yet underrepresented in studies.^16–18^
With this as the backdrop, a QIP was initiated; after a thorough literature review, we decided to address surgical mental and physical fatigue by incorporating hydration breaks and muscle stretches at pre-determined times during long surgical procedures.
Structured breaks have been shown to be effective in enabling tired and stressed theatre staff to refocus and mentally regroup. This is more important for team members who are assisting or performing passive roles, as research has shown that health professionals who are tired can have ‘micro-sleeps’ lasting a few seconds. A small randomised controlled study reported that introducing ‘micro-pauses’ can improve wellbeing without affecting overall timing of completing a procedure or disrupting flow.^19^ Additionally, there have been renewed efforts to reduce occupational musculoskeletal pain by encouraging desk job workers to perform short stretches, a concept that was incorporated into the operating room by Park et al.^16,20^
There was universal ‘buy in’ for the proposal, with all theatre personnel eager to participate in the project, thus reflecting the appetite for such change in a modern operating theatre. Our results revealed global improvement in pain scores measured after the surgery in the month when breaks were implemented. There was also subjective improvement in the ability to complete a surgical task with less fatigue perceived by the theatre personnel, most of whom felt more awake and energetic at the end of a procedure. Given the subjective nature of the tools used to measure fatigue and the single-centre study design, we chose to avoid overanalysis of the results, but rather present this as a proof-of-concept project.
The strengths of this project are as follows: the exercise routine has been simplified and takes into consideration the need for sterility and space in theatre, thus making it reproducible and feasible. Additionally, to our knowledge, this is probably the first time that premeditated sterile ‘hydration breaks’ have been introduced to prevent dehydration of theatre personnel involved in major surgery. In addition, these measures encourage theatre personnel to be open about work-related fatigue and serve to de-stigmatise this topic. This is very important in the context of major surgery, where surgical commitment and human factors have historically been at loggerheads. Another observation we made was that these breaks acted as a conversation starter, which improved communication and decreased operative room tension.
Despite these positive attributes there are certain limitations. First, we performed a ‘before and after’ analysis; the findings of this paper can be explained quite easily as a regression to the mean. Due to the subjective nature of assessment and the ‘buzz’ generated around the project in coffee rooms, the positive findings in the project could be explained by the Hawthorne effect.
Despite these limitations and the obvious need for the results of this study to be validated in multi-centred studies, the concept can be generalised to most minimally invasive and open major surgery. We have not relied on statistical significance to confer practical relevance for obvious reasons. We have also not discussed the effect that the breaks had on operative time or on ‘disruption of flow’ primarily because the breaks were triggered by the consultant when deemed safe, and the median operation time for peritoneal malignancy treatment is around seven hours, and therefore two-minute breaks were unlikely to be hugely consequential.
Conclusions
Theatre personnel involved in major surgery experience mental and physical stress that adversely affects work–life balance. Short hydration breaks with easy-to-follow muscle stretches can be incorporated into the standard practice of major abdominal surgery, serving to alleviate muscle stiffness and mental fatigue, thereby allowing theatre personnel to focus, regroup and concentrate on the job at hand.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Janhofer DE, Lakhiani C, Song DH. Addressing surgeon fatigue: current understanding and strategies for mitigation. Plast Reconstr Surg 2019; 144: 693e–699e.31568319 10.1097/PRS.0000000000006075 · doi ↗ · pubmed ↗
- 2Wells AC, Kjellman M, Harper SJF et al. Operating hurts: a study of EAES surgeons. Surg Endosc 2019; 33: 933.30456510 10.1007/s 00464-018-6574-5PMC 6394677 · doi ↗ · pubmed ↗
- 3Wright N, Mc Gown A. Vigilance on the civil flight deck: incidence of sleepiness and sleep during long-haul flights and associated changes in physiological parameters. Ergonomics 2001; 44: 82–106.11214900 10.1080/00140130150203893 · doi ↗ · pubmed ↗
- 4Neri DF, Oyung RL, Colletti LM et al. Controlled breaks as a fatigue countermeasure on the flight deck. Aviat Space Environ Med 2002; 73: 654–664.12137101 · pubmed ↗
- 5Chen C, Xie Y. Modeling the safety impacts of driving hours and rest breaks on truck drivers considering time-dependent covariates. J Safety Res 2014; 51: 57–63.25453177 10.1016/j.jsr.2014.09.006 · doi ↗ · pubmed ↗
- 6Hallbeck MS, Lowndes BR, Bingener J et al. The impact of intraoperative microbreaks with exercises on surgeons: a multi-center cohort study. Appl Ergon 2017; 60: 334–341.28166893 10.1016/j.apergo.2016.12.006 · doi ↗ · pubmed ↗
- 7Holden RJ, Carayon P. SEIPS 101 and seven simple SEIPS tools. BMJ Qual Saf 2021; 30: 901–910.10.1136/bmjqs-2020-012538 PMC 854319934039748 · doi ↗ · pubmed ↗
- 8Wilson MR, Poolton JM, Malhotra N et al. Development and validation of a surgical workload measure: the surgery task load index (SURG-TLX). World J Surg 2011; 35: 1961–1969.21597890 10.1007/s 00268-011-1141-4PMC 3152702 · doi ↗ · pubmed ↗