Variation in Attitudes to Native Kidney Biopsy Practice in the United States
Michael P. Toal, Christopher J. Hill, Michael P. Quinn, Emily P. McQuarrie, Charuhas V. Thakar, Ciaran O’Neill, Alexander P. Maxwell

TL;DR
A survey of US kidney specialists found significant variation in attitudes toward kidney biopsies, influenced by factors like age, gender, and state characteristics.
Contribution
The study identifies clinician and geographic factors influencing kidney biopsy recommendations in the US using a nationwide survey.
Findings
Higher biopsy propensity scores were found in male, younger, and more experienced clinicians.
US states with higher nephrologist density and lower deprivation had higher biopsy recommendation scores.
There was significant variation in biopsy attitudes between US states, with scores ranging from 20.3 to 29.2.
Abstract
There is substantial variation in kidney biopsy practices within and between countries; however, the reasons for this are unclear due to limited research among large diverse populations. The aim of this study was to explore variations in attitude to the indications and contraindications for native kidney biopsy in the United States (US). A case-vignette questionnaire was developed. A propensity-to-biopsy score (0-44) was generated from responses to indications and contraindications, with a higher score indicating an increased likelihood to recommend biopsy. Dissemination of the questionnaire occurred by email, social media, and the National Kidney Foundation. A total of 295 nephrologists/fellows from 43 states within the US participated. All participants completed an identical questionnaire on kidney biopsy practice. Responses were collected on indications, contraindications, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
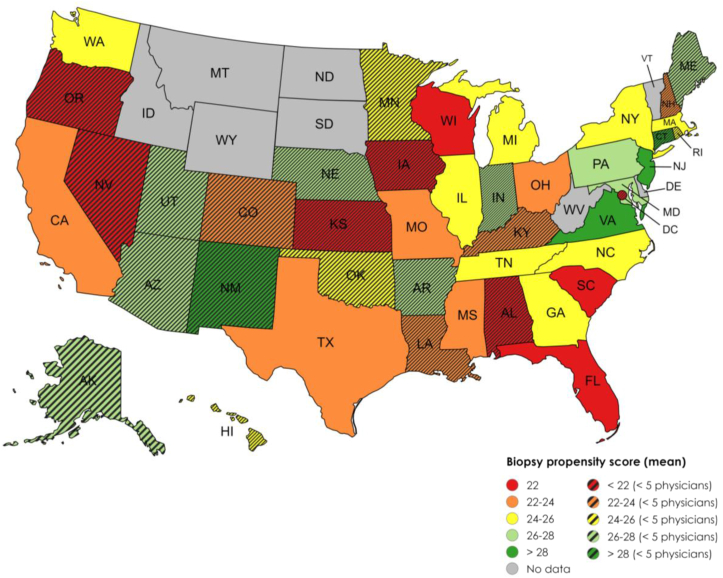 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChronic Kidney Disease and Diabetes · Renal Diseases and Glomerulopathies · Dialysis and Renal Disease Management
Kidney biopsy has been used in nephrology since the 1950s for the diagnosis of kidney disease and to inform management.1^,^2 Despite it being accepted as the gold standard diagnostic test, widespread variation in kidney biopsy practices is recognized both across centers and between countries.3 There is limited understanding of the causes and effects of these variations within the currently available literature, with studies restricted to clinician surveys of single countries with limited participant numbers.4^,^5
Advances in precision medicine are improving our understanding of the pathogenesis of kidney disease at the molecular level. Initiatives like the Kidney Precision Medicine Project use biopsy samples for advanced proteomic and genomic analysis to identify novel markers of risk.6 Multiple new treatments for biopsy-proven kidney disease have been evaluated through randomized controlled trials, and these novel therapies are entering clinical practice.7, 8, 9, 10 This requires a more consistent standard of when diagnostic tools such as kidney biopsy should be applied so that patients can access effective treatment in a timely manner.
The practice of kidney biopsy varies internationally and is traditionally under the remit of nephrology and interventional radiology. In the United States (US), nephrologists are increasingly referring to radiologists rather than performing this procedure themselves, and fellows are not required to be competent in performing kidney biopsy for certification.11^,^12 This could lead to a cultural distancing of nephrologists in the practice and value of a kidney biopsy.
One of the reasons nephrologists may be cautious about kidney biopsy is the recognized small risk of complications. Serious complications can arise, particularly relating to bleeding.1 Persistent hemorrhage may require radiological embolization in around 1 in 300 biopsy procedures, and death linked to kidney biopsy has been reported in around 1 in 2000 procedures.13, 14, 15, 16
The decision to perform a kidney biopsy remains subjective and dependent on multiple factors unique to each patient. Each clinician across the US and internationally operates within a different context of resources, therefore decisions may be subject to these constraints.4^,^5
Objective
This study examines the hypothesis that attitudes to kidney biopsy vary among nephrologists in the US.
Methods
Findings are described in line with the checklist for reporting results of internet e-surveys.17 A detailed explanation of methods have been described in a previous paper18 but are briefly summarized below.
Questionnaire Design
The study was part of a larger international study of attitudes to kidney biopsy.18 Clinicians who were eligible for inclusion here were physicians practicing in the US who specialized in adult nephrology. A case-vignette online questionnaire was designed to explore the reasoning behind clinical practice variation, which is detailed in the supplementary material (Item S1). The first section focused on collecting anonymized demographic details of the individual and their institution. The second section focused on decisions and attitudes. Seven scenarios of case vignettes were presented for the physician to decide if a kidney biopsy was required for each patient on a 5-point scale from definitely yes to definitely no. For contraindications, respondents were asked to define the tolerable limits of laboratory results, clinical observations, and prescribed drugs that may contraindicate biopsy. Attitudes and previously cited barriers were explored in the final part of the questionnaire.19
Propensity-to-Biopsy Score
Responses to 11 questions in the indications and contraindications section were coded from 0-4. For the case vignettes, if the respondent selected definitely yes, this was scored as 4 points, with decreasing values for each option to definitely no, which scored 0 points. For contraindications, the closest option to a normal value (eg, platelet count = 150 × 10^9^) was scored as 0, whereas the selected option of proceeding to biopsy regardless of the value (eg, no minimum level) was scored as 4.
This scoring system generated a total propensity-to-biopsy score from 0-44 for each clinician who completed the entire questionnaire, with a higher score signifying the clinician was more likely to recommend biopsy.
Patient and Public Engagement Summary
Ethical approval for this project was granted by the research ethics committee of Queen’s University Belfast and all participants indicated their consent and eligibility before entering the questionnaire. The questionnaire was co-designed with patient participation from 10 patients who had underwent a total of 23 kidney biopsies from across the United Kingdom (UK). This study explored the barriers and experience of kidney biopsy from a patient’s perspective,20 which facilitated further study of the physician’s perspective.
Questionnaire Administration
The survey was piloted first within the research team and then in one UK region before wider international dissemination. Participants in the US were recruited through an anonymized open web address, which was shared through email lists of nephrology societies, including the National Kidney Foundation, and on social media.
The questionnaire was hosted on Qualtrics XM, which collected anonymized IP addresses for state-level analysis, based on the assumption that the questionnaire was completed in the participant’s state of clinical practice. This software prevented multiple entries and used a completely automated public Turing test to tell computers and humans apart feature to safeguard against automated entries. International recruitment occurred from August 29, 2023, to January 14, 2024. Because of the nature of US distribution through social media and the National Kidney Foundation, it is difficult to estimate response rates. Within regions of the UK and Ireland where the survey was also undertaken, over 50% of eligible clinicians participated.
Analysis
All clinicians who met the inclusion criteria and answered one or more questions were contained in the final dataset; however, the propensity-to-biopsy score was only counted if all relevant questions were answered.
To help contextualize responses, data were obtained on nephrologist density per 100,000 adults by state.21 The US Census data were used to arrange states by deprivation,22 which were grouped into quintiles with similar numbers of clinicians. Analysis by state focused on states with 5 or more participants. For international context, US responses were compared with the country with the second highest national participation, the UK.
The complete dataset was analyzed in Stata 17 (StataCorp). Aggregate results were expressed as means if normally distributed or medians if skewed. Discrete variables were reported by frequency. An unpaired t test was used to compare continuous variables between 2 groups and ANOVA with Bonferroni adjustment in the setting of 3 or more groups. A severe complication was defined as one that required an intervention of embolization, surgery or that resulted in death. An adjusted multiple linear regression model was applied to ordinal or continuous demographic categories to assess the impact on propensity score. Significance levels were tested at the 5% level (P < 0.05).
Results
National Demographics
A total of 295 US clinicians participated in the study. Findings from the entire international cohort are detailed in another article.18 The US clinician and institutional demographics are summarized in Table 1. The entire questionnaire was completed by 92.2% of US participants. A broad range of age groups were represented; however, only 26% of respondents identified as female, which is consistent with the current US workforce.23 About 64.7% of the US clinicians had performed at least one kidney biopsy in the previous year; however, for 66.8% of participating clinicians, the usual operator in their institution was a radiology specialist. About 46.2% of clinicians reported that the most significant biopsy complication they had ever encountered was one requiring an invasive intervention or causing death, classed as a severe complication in this study.Table 1. Individual and Institutional Demographic Details of CliniciansVariableFrequency%Questionnaire completed Yes27292.2 No237.8Route of completion Email link13545.8 Social media16054.2Sex Male21172.3 Female7626.0 Prefer not to say41.4 Nonbinary/third gender10.3Age, y 20-2920.7 30-3910234.6 40-497224.4 50-596722.7 60 or over5217.6Current job title Trainee/fellow186.1 Associate specialist/specialty doctor113.8 Consultant/attending physician23580.2 Clinical director or professor289.6 Other10.3Estimated No. of biopsies performed in last year 010435.3 1-55418.3 5-2010334.9 20-50248.1 50 or more103.4Most significant complication encountered Nonsevere15654.8 None3612.4 Macroscopic hematuria6422.1 Hematoma41.4 Blood transfusion5017.2 Nonrenal organ injury10.3 Other10.3 Severe13446.2 Radiological embolization9934.1 Emergency surgery20.7 Nephrectomy113.8 Death227.6Health care system Public7927.2 Private13446.2 Public and private6723.1 Not sure103.5Main place of work Independent clinic217.3 Rural or district general hospital165.5 Suburban hospital8128.0 University/Urban/Military hospital17058.8 Other10.4Typical time from referral to biopsy by radiologist Same day103.5 Within 1 week17159.0 Within 1 month8429.0 Beyond 1 month20.7 Unsure237.9Most frequent performer of kidney biopsy at institution Nephrologist7124.6 Radiologist18764.7 Nephrology trainee/fellow248.3 Radiology trainee/fellow62.1 Not sure10.4Observation time after kidney biopsy Less than 4 h4917.0 4-8 h17359.9 8-24 h5820.1 Beyond 24 h51.7 Unsure41.4
State-Level Comparison
Forty-three US states were represented in this study and in 18 states, 5 or more clinicians contributed (Table 2). For comparisons, only US states with at least 5 clinicians were included in statistical analysis. To investigate the social and economic influences on attitudes to practice, data were obtained on the relative deprivation of each state,22 which was then divided into quintiles to provide similar sized groups for each quintile of deprivation (55-63 clinicians each).Table 2US State-Level Data on ParticipantsUS StateNo. of ParticipantsMean Propensity-to-Biopsy ScoreDeprivation QuintileNephrologists/100,000 AdultsAlabama22213Alaska12730.8Arizona427.522.9Arkansas12712.3California2623.533.1Colorado323.752.6Connecticut13044.6Delaware0N/AN/A4Florida1121.423Georgia62523.3Hawaii32542.2Idaho0N/AN/A1.6Illinois2225.743.1Indiana12833.2Iowa22242Kansas11742.6Kentucky222.512.8Louisiana423.314Maine12842.5Maryland62844.4Massachusetts1125.955.3Michigan824.533.2Minnesota324.353.5Mississippi522.313.1Missouri62433.2Montana0N/AN/A1Nebraska22752.3Nevada32122.3New Hampshire12451.8New Jersey629.254New Mexico12912.1New York2525.524.7North Carolina924.323.4North Dakota0N/AN/A2.7Ohio122433Oklahoma22512.2Oregon22242.2Pennsylvania1226.844Rhode Island12644.2South Carolina720.413.1South Dakota0N/AN/A3.6Tennessee825.433.4Texas2923.313.3Utah12851.7Vermont0N/AN/A2Virginia629.243Washington2724.252.7West Virginia0N/AN/A2.7Wisconsin720.352.5Wyoming0N/AN/A0.9District of Columbia220.51N/ANote: Missing data reported as N/A. Deprivation quintiles: 1 = most deprived, 5 = least deprived.
In states with at least 5 participants, the highest propensity-to-biopsy score was observed in clinicians from New Jersey and Virginia (29.2), and the lowest was in Wisconsin (20.3). A breakdown of the mean propensity score by state is represented in Fig 1. The state with the highest nephrologist density per 100,000 adults was Massachusetts at 5.3 per 100,000 adults, and the lowest nephrologist density was Alaska at 0.8 per 100,000 adults.Figure 1. Mean propensity-to-biopsy score divided into the state where clinicians completed the questionnaire. A dark green color is associated with the highest propensity score and red with the lowest. Striped states had less than 5 participants and were not included in statistical analysis. Graphic courtesy of mapchart.net.
Analyzing Attitudes to Practice
A multiple linear regression model was used to investigate the association between individual, institutional, and state characteristics and how this impacted on propensity-to-biopsy scores. All variables were included in the first model, and then regression with backward elimination was used to sequentially remove nonsignificant variables. The variables that remained significant after adjustment are described in Table 3.Table 3. Adjusted Multiple Linear Regression Table of the Effect of Demographic Variables on Propensity-to-Biopsy ScoreVariableCoefficientSESignificance95%CI·Lower95% CI UpperSex (=female)−1.2400.6240.048−2.469−0.012Age (by increasing age group)−0.5960.2460.016−1.080−0.111Biopsy frequency (by increasing group)+0.5550.2470.026+0.068+1.042Deprivation quintile+0.5320.1910.006+0.155+0.909Nephrologist density/100,000 population+1.1460.3480.001+0.460+1.832Note: n = 257, F = 6.50. Adjusted R^2^ = 0.097.
A number of variables were significantly associated with increased propensity-to-biopsy scores. Male physicians, those of younger age, and more regular performers of kidney biopsy were all significantly associated with increased biopsy propensity scores, after adjustment for other factors (P = 0.05). These variables demonstrated a similar association in the full international cohort.
Nephrologists from less deprived states reported a greater willingness to biopsy, as did those from states with higher numbers of nephrologists per head of the adult population. While the overall regression was significant as evidenced by the F-statistic, collectively the explanatory variables used only accounted for 10% of the variation in scores; therefore, 90% of the variation in scores remains unexplained by the variables in this model.
Comparing US Practice to the UK
To examine US practice in a global context, US responses were compared to the second largest national group in this study, the UK (n = 213). Although these countries are aligned in many geopolitical and social issues, their health care systems differ in terms of funding (a lower proportion of Gross Domestic Product is spent on health care in the UK), population, and provision of care (the UK health care is free at the point of need). Among respondents to this survey, only 27.2% of US clinicians worked in a solely publicly funded service, in contrast to 98% of UK clinicians. We hypothesized that economic factors for clinicians would differ between clinicians in these 2 nations and might influence attitudes. Additionally, there are significant differences in clinical practice. 88% of UK participants indicated that the usual biopsy operator was a nephrologist or nephrology fellow at their institution, compared to only 33% of US clinicians, in which most procedures were performed by a radiologist (P < 0.001).
The mean propensity-to-biopsy score was significantly higher in the US (24.5) compared with the UK (23.5) (P = 0.01). The most significant barriers to biopsy access differed between respondents in the 2 countries (Table 4). The most significant barrier for US clinicians was time constraints, whereas this was deemed to be the least significant factor in the UK. By contrast, the least significant barrier reported by US clinicians was the risk of complications, which was deemed to be the most significant barrier by UK clinicians (P < 0.001). Therefore, in this study it appeared that perceptions on barriers to access were highly contingent on what the typical practice was in that country. US clinicians rated the barriers to biopsy access as more significant than respondents from the UK (P < 0.001).Table 4. Comparison of Perceived Barriers to Kidney Biopsy Between US and UK CliniciansUnited StatesUnited Kingdom1. Time constraints1. Risk of complications2. Staff availability2. Staff availability3. Room and equipment availability3. Room and equipment availability4. Risk of complications4. Time constraintsNote: Respondents were asked to rate the significance of each factor from 1 (least significant) to 5 (most significant). The potential barriers are ranked for each country in order from most to least significant.
Discussion
General Interpretation
This study suggests that there are variations in attitudes to kidney biopsy practice across the US. Males, younger physicians, and more frequent biopsy operators were found to have an increased propensity to recommend kidney biopsy, as were individuals working in states with higher nephrologist coverage and economic affluence. While the significance of practitioner density and deprivation are interesting, caution is warranted given the potential for ecological fallacy, that is, that inferences are made about an individual based on their membership of a group. Therefore, we cannot assume that a nephrologist in Massachusetts would make a different decision to their colleague in Oklahoma in a given clinical scenario, particularly as the variables in the regression model could only account for 10% of the variation in scores.
It is difficult to explain the variations in biopsy rates between states, but it may be that where there is a higher density of nephrologists, there is a higher capacity to provide services such as a kidney biopsy. However, these inferences are speculative and require investigation beyond the scope of this study.
This study also revealed some interesting findings around postbiopsy observation periods, where again there were variations in practice; however, most centers observed patients for 8 hours or less postprocedure. This has economic consequences for health care delivery, as patients will not need an overnight admission to hospital for observation after a routine kidney biopsy.
It is notable that US clinicians report different barriers to kidney biopsy than their UK colleagues. US-based nephrologists reported that time constraints were the most significant barrier to biopsy, whereas UK clinicians reported the risk of complications as the predominant limitation. There are relevant differences in health care systems and clinical practice that have been outlined. Potential explanations for these disparities could be that US clinicians who bill for each service may feel the time taken to organize and perform a biopsy may not be a cost-effective use of time compared with other clinical activities. Alternatively, as US nephrologists often delegate this procedure to radiologist colleagues rather than performing biopsies themselves, the responsibility of exposing patients to the potential risks is shared with the operator performing the procedure rather than being borne solely by the nephrologist. However, a circumspect approach is best applied in this instance, as these inferences are beyond the scope of this study.
A Scottish study demonstrated that greater socioeconomic deprivation was associated with higher kidney biopsy rates24; however, in the UK, health care is free at the point of access for all citizens in a nationalized public health system, therefore, these findings may not be directly translatable to the US. The privatized US health care system and greater cultural and racial diversity could indeed widen these gaps in health care attainment, fortifying the importance of understanding the barriers to achieving equitable health care delivery. Not all Americans have health insurance, which may affect access to a kidney biopsy. One of the limitations of a questionnaire is that although the differences are statistically significant, it is unclear whether they truly reflect clinically significant practice variations resulting in higher or lower rates of biopsies in the future. There may be differences in how someone might answer this survey based on their location, which may not be reflective of actual clinical practice.
Amodou et al25 interviewed 20 nephrologists to understand their attitudes to practice. In this study, nephrologists who performed their own biopsies reported that they believed this heuristic lowered their threshold to order this procedure, which is consistent with our findings.
Limitations
This study has potential limitations. This is an opt-in online questionnaire to investigate attitudes to practice and is more likely to appeal to clinicians with an interest in kidney biopsy, who may be disproportionately represented in a small sample size relative to the total eligible population. The use of social media resulted in a relatively young study population, which may not be generalizable to the entire profession.
The area-based characteristics investigated are reliant on previously collected records, which may not be entirely accurate or contemporaneous and will not reflect the granularity of population or practice within each state. The clinical vignettes are insufficient in detail to reflect all of the considerations, which may be required to make a decision on kidney biopsy. The vignettes are condensed clinical scenarios to promote participant engagement to help in determining the predominant driving and limiting factors of practice.
Strengths
The study also has significant strengths. In addition to being the largest international study of kidney biopsy practice, the high uptake from US clinicians at various stages of their careers, from fellowship to extended independent practice, has also made it the largest study of US attitudes that the authors are aware of. Additionally, the representation from 43 states increases generalizability at a national level. Furthermore, the opportunity to compare the findings internationally strengthens the evaluation.
Implications for Practice
This study demonstrates that there is variation in attitudes to kidney biopsy practice when nephrologists are confronted with identical clinical scenarios. Most of the variation demonstrated remains unexplained by demographics of either the individual participant or their working environment. Additionally, it also remains unclear if the variation in attitudes reported translates into measurable differences in clinical practice, which could have implications for patient access. Such studies can be used as a feedback mechanism to inform practitioners, providing insight into the real and perceived variations that can in turn facilitate standardization of practices.
Conclusion
Attitudes to kidney biopsy practice were found to be variable across the US and were associated with individual and area-based factors. Strikingly, only 10% of the variation in propensity-to-biopsy scores could be explained in terms of observable characteristics. We propose that a study such as ours will inform physicians of key parameters that could be overcome in reducing variations in practice. Further prospective monitoring would be required to understand if such efforts affect uniformity in practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hogan J.J.Mocanu M.Berns J.S.The native kidney biopsy: update and evidence for best practice Clin J Am Soc Nephrol 112201635436210.2215/CJN.0575051526339068 PMC 4741037 · doi ↗ · pubmed ↗
- 2Rovin B.H.Adler S.G.Barratt J.KDIGO 2021 clinical practice guideline for the management of glomerular diseases Kidney Int 10042021 S 1S 27610.1016/j.kint.2021.05.02134556256 · doi ↗ · pubmed ↗
- 3Mc Quarrie E.P.Mac Kinnon B.Young B.Centre variation in incidence, indication and diagnosis of adult native renal biopsy in Scotland Nephrol Dial Transplant 24520091524152810.1093/ndt/gfn 67719074409 · doi ↗ · pubmed ↗
- 4Kawaguchi T.Nagasawsa T.Tsuruya K.A nationwide survey on clinical practice patterns and bleeding complications of percutaneous native kidney biopsy in Japan Clin Exp Nephrol 245202038940110.1007/s 10157-020-01869-w 32189101 PMC 7174253 · doi ↗ · pubmed ↗
- 5Burke J.P.Pham T.May S.Kidney biopsy practice amongst Australasian nephrologists BMC Nephrol 221202129110.1186/s 12882-021-02505-934445981 PMC 8390249 · doi ↗ · pubmed ↗
- 6de Boer I.H.Alpers C.E.Azeloglu E.U.Rationale and design of the Kidney Precision Medicine Project Kidney Int 993202149851010.1016/j.kint.2020.08.03933637194 PMC 8330551 · doi ↗ · pubmed ↗
- 7Barratt J.Lafayette R.Kristensen J.Results from part A of the multi-center, double-blind, randomized, placebo-controlled Nef Ig Ard trial, which evaluated targeted-release formulation of budesonide for the treatment of primary immunoglobulin A nephropathy Kidney Int 1032202339140210.1016/j.kint.2022.09.01736270561 · doi ↗ · pubmed ↗
- 8Heerspink H.J.L.Radhakrishnan J.Alpers C.E.Sparsentan in patients with Ig A nephropathy: a prespecified interim analysis from a randomised, double-blind, active-controlled clinical trial Lancet 401103882023 May 131584159410.1016/S 0140-6736(23)00569-X 37015244 · doi ↗ · pubmed ↗