Streptococcus equi Subspecies zooepidemicus Infective Endocarditis: A Case Report of a Rare Bacterium and Review of the Literature
Sara Jochumsen, Julie KK Vishram-Nielsen, Bettina B Pump, Marie B Seibæk, Niels E Bruun

TL;DR
A rare case of infective endocarditis caused by Streptococcus equi subspecies zooepidemicus is reported, highlighting its unusual occurrence in humans.
Contribution
This paper presents a rare clinical case and literature review of S. zooepidemicus infective endocarditis in humans.
Findings
S. zooepidemicus caused infective endocarditis in a patient with a prosthetic heart valve.
The infection was complicated by meningitis and myocardial infarction.
Literature review identified only 13 reported human cases of S. zooepidemicus IE.
Abstract
Infective endocarditis (IE) is a dreaded disease with a high mortality rate. In Denmark, IE is most often caused by Staphylococcus aureus or Streptococcus species. We present a rare case of a 50-year-old woman with a history of a dual-chamber pacemaker due to third-degree atrioventricular block and a mechanical mitral valve inserted due to mitral stenosis. The patient was admitted to the hospital after she was found lying on the floor in her home. The patient was diagnosed with Streptococcus equisubspecies zooepidemicus (S. zooepidemicus) prosthetic heart valve IE, which was complicated with meningitis, myocardial infarction, and an increasing vegetation load despite antibiotic treatment. The patient underwent heart valve surgery with insertion of a biological mitral valve, and S. zooepidemicus was identified in the excised valve tissue. S. zooepidemicus is a rare zoonotic pathogen in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
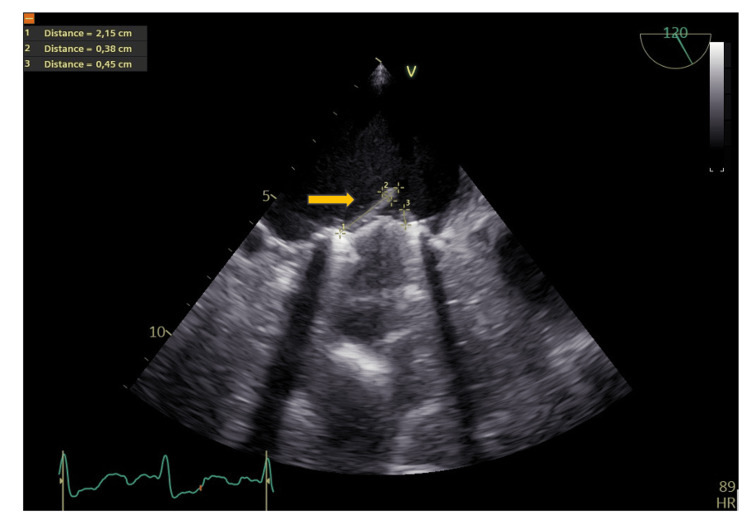 Figure 1
Figure 1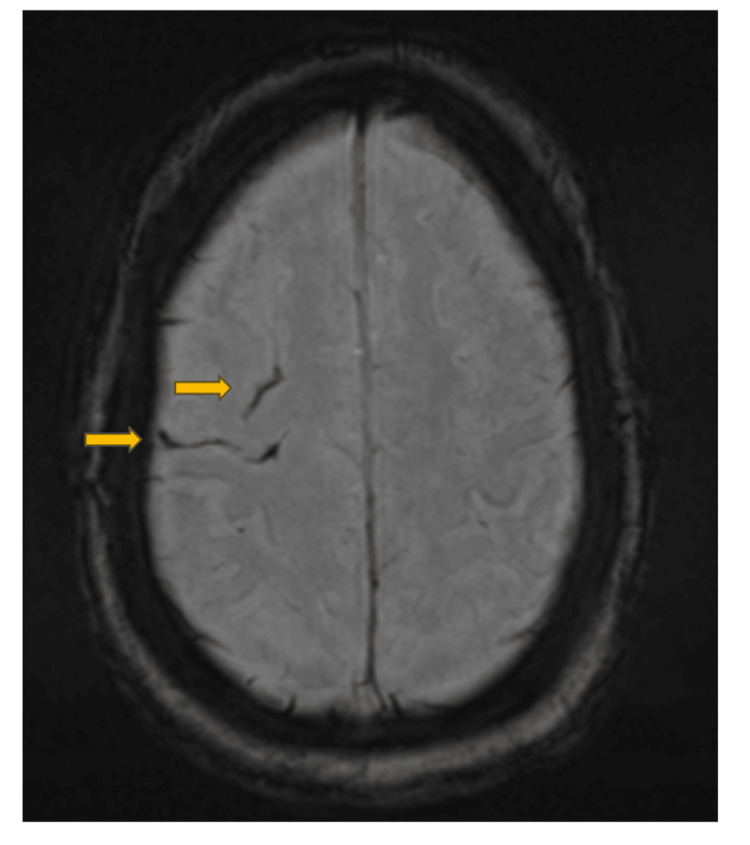 Figure 2
Figure 2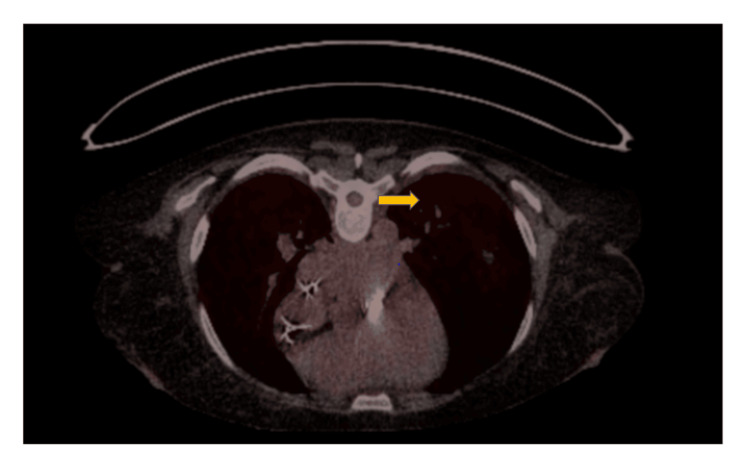 Figure 3
Figure 3 Figure 4
Figure 4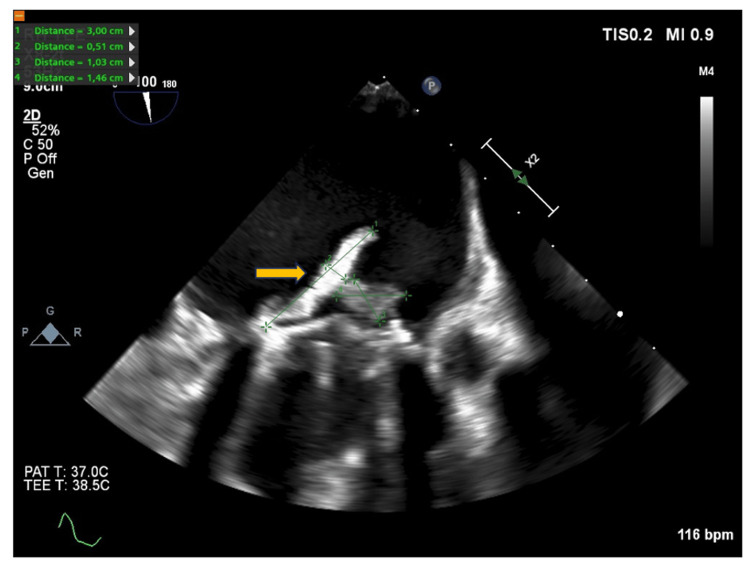 Figure 5
Figure 5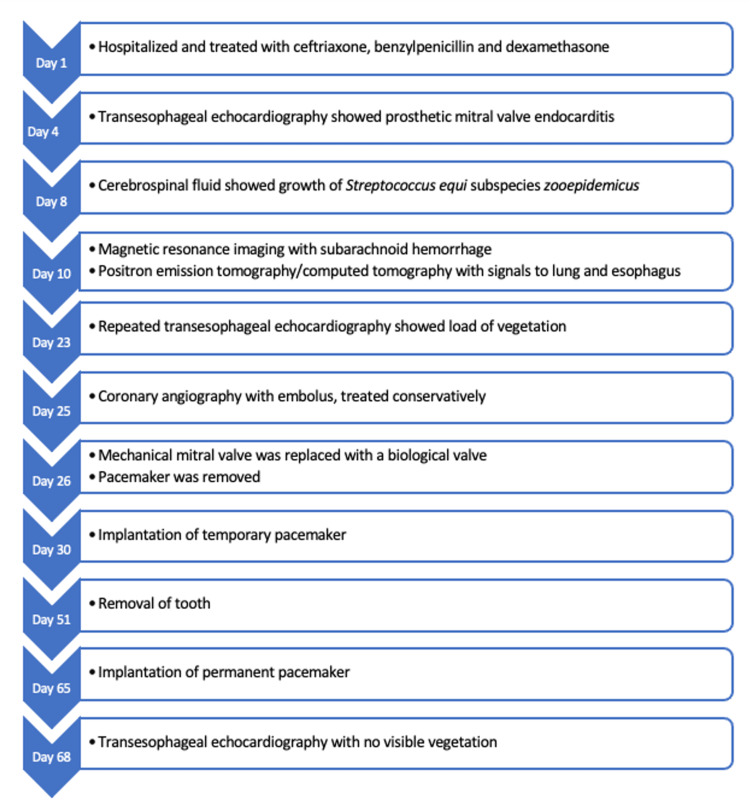 Figure 6
Figure 6| Patient’s result | Reference | |
| C-reactive protein | 340 mg/L | <8 mg/L |
| Leukocytes | 7.10 x109/L | 3.50-8.80x109/L |
| Thrombocytes | 210 x109/L | 145-390x109/L |
| Haemoglobin | 6.50 mmol/L | 7.30-9.50 mmol/L |
| Estimated glomerular filtration rate | 65 mL/min/1.73 m2 | >60 mL/min/1.73 m2 |
| Saturation | 98% | 95-100% |
| Year of Publication | Author | Study | Country | Sex and Age | Suspected Source of Contamination | Comorbidities | Symptoms | Implicated Valve | Treatment |
| 2024 | Franceschi et al. [ | Review and case report | Italy | Male, 62 years | Horse | Hypertension and hypercholesterolemia | Intermittent high fever, cough, memory deficits, and confusion | Aortic valve | Aortic valve replacement with a biological prosthesis and intravenous cefotaxime and gentamicin |
| 2018 | Høyer- Nielsen et al. [ | Case report | Faroe Islands | Male, 82 years | Horse | Ischemic heart disease, atrial fibrillation, low malignant prostate cancer, gout, type 2 diabetes, and removal of all teeth in the upper mouth six months prior | Dyspnea, hemoptysis, impaired general condition, and shoulder pain | Aortic valve | Intravenous cefuroxime and benzylpenicillin, oral amoxicillin and rifampicin |
| 2015 | Villamil et al. [ | Case report | Spain | Male, 73 years | Horse | Hypertension, dyslipidemia, diverticulosis, metallic aortic valve prosthesis, dilatation of the ascending aorta with a valved tube | Fever, poor general condition | Aortic valve prosthesis | Intravenous penicillin and gentamicin |
| 2013 | Pelkonen et al. [ | Case report | Finland | Male, 57 years | Horse | Aortic valve insufficiency | Unconscious, febrile | Bicuspid aortic valve | Resection of the aortic valve and intravenous high-dose penicillin and gentamicin |
| 2009 | Poulin et al. [ | Case report | Canada | Female, 59 years | Horse | Hypertension, type 2 diabetes, dyslipidemia, myocardial infarction, chronic renal failure, obesity, left ophthalmic vein thrombosis, atrial septal defect, hypothyroidism, primary hyperparathyroidism | Generalized weakness, lightheadedness when standing up, fever, more dyspneic, vomiting, resting tremors, clear rhinorrhea, cough | Posterior leaflet of the mitral valve | Valve replacement and intravenous ceftriaxone and rifampin |
| 2006 | Bordes-Benítez et al. [ | Clinical and epidemiological study | Spain | Female, 70 years | Inadequately pasteurized cheese | None | Joint pain, gastrointestinal symptoms | Unknown | Beta-lactam agent |
| 2004 | Lee et al. [ | Case report | England | Male, 79 years | Unknown | None | Right-leg pain, fever, severe headache, deteriorating conscious state | Aortic valve | Intravenous penicillin |
| 1990 | Yuen et al. [ | Case report | China | Female, 58 years | Unknown | Unknown | Unknown | Mitral valve | Intravenous benzylpenicillin |
| 1988 | Edwards et al. [ | Case reports | England | Male, 73 and 79 years, female, 52 years | Unpasteurized cow milk | Unknown | Fever, confusion, flu-like illness | Unknown | Cephalosporins, ampicillin, metronidazole, penicillin |
| 1982 | Martinez-Luengas et al. [ | Case report | Spain | Male, 51 years | Animals | Rheumatic heart disease with mitral and aortic valve involvement, occasional pulmonary edema | Fever, malaise | Mitral valve | Intravenous penicillin and intramuscular streptomycin |
| 1980 | Ghoneim et al. [ | Case report | England | Male, 81 years | Animals | Chronic rheumatic heart disease | Retrosternal chest pain, lethargy, malaise, fever, mildly confused | Unknown | Intravenous penicillin, gentamicin, and oral amoxycillin |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Streptococcal Infections and Treatments · Bacterial Identification and Susceptibility Testing
Introduction
Infective endocarditis (IE) is a severe disease, with a largely unchanged mortality rate within the last two decades of 15-30% in-hospital and a mortality rate of 30-40% during the first year after diagnosis [1]. The symptoms are highly variable. Some cases develop acutely with a picture of severe illness with sepsis, rapidly progressive heart failure and unstable hemodynamics due to valve destruction. However, most cases have an insidious course that develops from weeks to months. These patients have diverse and diffuse complaints with low fever, weight loss, musculoskeletal pain, varying degrees of dyspnea, headache, neurological symptoms, and fatigue. Such symptoms are also found in several other chronic conditions, and it is not uncommon for IE patients to have undergone an evaluation for chronic inflammatory disorders or cancer, just as they may have received one or more courses of antibiotics for suspected respiratory or other infections. In addition, approximately 10-20% of IE patients have signs of embolization at the time of diagnosis [1]. In Denmark, Streptococci are implicated in a little more than 30% of IE cases [2]. Streptococci are a heterogeneous group of bacteria with more than 50 different species [3], and certain species have been documented to be more strongly associated with IE than others [3,4]. Previous studies have identified Streptococcus mitis/oralis and Streptococcus gallolyticus (belonging to the Bovis group) among the streptococcal species with the highest IE prevalence and the highest associated IE risk after adjusting for known IE risk factors [4,5]. S. zooepidemicus is classified as a gram-positive, β-hemolytic streptococcus, belonging to Lancefield group C. S. zooepidemicus is a normal commensal of the oral cavity, pharynx, and respiratory tract of horses and may cause respiratory diseases as an opportunistic pathogen [6]. In a few cases, the bacterium has been isolated in humans as a zoonotic pathogen, although infections are very rare [7]. But severe human infections, including sepsis, meningitis, septic arthritis, or IE, have been described [7].
Here, we present a complicated case of IE with S. zooepidemicus in a Danish female patient with repetitive episodes of fever, as well as a literature review of previously described human cases of S. zooepidemicus IE.
Case presentation
A 50-year-old Caucasian woman with a medical history of a mechanical mitral valve due to mitral stenosis, dual-chamber pacemaker due to third-degree atrioventricular block, anxiety, depression, and chronic joint and muscle pain was admitted to the hospital after being found lying with cognitive impairment on the floor at home.
Three days prior to her current hospital admission, the patient had experienced fever, chills, headache, malaise and increasing discomfort due to non-productive cough. The patient had consulted her General Practitioner who suspected that she had the flu. A few months prior to the current hospital admission, the patient had been admitted twice with fever, muscle pain, malaise, and dyspnea and had received treatment for pneumonia with various antibiotic treatments including penicillin.
Interestingly, the patient owned two horses, which she visited daily for approximately four hours. Additionally, she attended riding lessons at a riding club once a week from August 2024. The club housed around 10-20 horses.
At the time of the current admission, the patient was noticed to have cognitive impairment and after a lumbar puncture she received treatment for meningitis with penicillin and ceftriaxone. The spinal fluid was clear with 332 cells, of which 195 were mononuclear leukocytes and 137 were polynuclear leukocytes. Additionally, lactate in the spinal fluid was 4.00 mmol/L protein 1.40 g/L and S. zooepidemicus DNA was identified by 16S PCR.
Blood cultures were drawn at the time of admission and showed three out of three bottles positive for S. zooepidemicus. Two bottles were aerobic, and one was anaerobic. Each bottle contained 10 mL of blood. The bacteria were sensitive to penicillin with a minimum inhibitory concentration (MIC) value of 0.032 mg/L and to moxifloxacin, gentamycin, ampicillin and rifampicin with MIC values of 0.250, 32.000, 0.064 and 0.032 mg/L, respectively. Blood cultures were repeated 14 days later and showed no microbial growth. Blood cultures were repeated on three additional instances, and all were without microbial growth. C-reactive protein (CRP) value was increased, whereas leukocytes and thrombocytes were normal, and hemoglobin was low. Furthermore, oxygen saturation and estimated glomerular filtration rate (eGFR) were normal and blood pressure was 104/58 mmHg (see Table 2). There was no audible heart murmur apart from the murmur produced by the mechanical mitral valve. Transesophageal echocardiography (TEE) was performed on suspicion of IE, and showed a 2.15x0.38 cm vegetation on the posterior leaflet of the mitral valve and there was a suspicion of a small vegetation on the anterior leaflet of the mitral valve of 0.45 cm (Figure 1). There were no vegetations on the aortic valve or on the right-sided heart valves. Moreover, the left ventricle was of normal dimension but with reduced ejection fraction of 35%. The patient was known for having a reduced LVEF after the previous mitral valve operation.
A transesophageal echocardiography (TEE) of the prosthetic mitral valve with visualization of the vegetation three days after hospital admissionArrow shows vegetation with measurements
A magnetic resonance imaging (MRI) of the cerebrum demonstrated a minor subarachnoid hemorrhage in the right frontal lobe and a microbleed in the left frontal lobe, but no abscesses or infarcts (Figure 2). On the same day, a positron emission tomography/computed tomography (PET/CT) scan showed positive fluorine-18-fluorodeoxyglucose (F18-FDG) signals in the left lung, indicating pneumonia, and in the esophagus (Figure 3). There was no F-18-FDG activity suggesting infection in the gastrointestinal channel, on the pacemaker generator, or on the electrodes. The patient was referred for further examination of the esophagus, but the F18-FDG signal in the esophagus was considered of no significance.
Magnetic resonance imaging (MRI) of the cerebrumArrows show subarachnoid hemorrhages in two sulci in the right frontal lobe
Positron emission tomography/computed tomography (PET/CT) of lungs Arrow indicates pneumonia in left lung
A dental examination of the patient revealed paradontitis apicalis in one tooth, and the patient was scheduled for extraction of the tooth, which was performed during hospitalization. The tooth was not definitively identified as the cause of IE.
On Day 25 after admission, the patient experienced central chest pain. An electrocardiogram (ECG) showed paced rhythm, and troponin T (TnT) level was elevated to 41 ng/L. On suspicion of acute coronary syndrome, a coronary angiography was performed, demonstrating an occlusion, most likely an embolus, in the distal part of an obtuse marginal artery, which was treated conservatively. An overview of the patient’s clinical symptoms is presented in Figure 4.
Timeline of clinical symptoms from index admission to end of hospitalization The diagram should be read from left to right.
Despite continuous treatment with penicillin and moxifloxacin, CRP stagnated around 150 mg/L, and the patient experienced worsening of fever from 38.1 °C to 39.6 °C. High CRP levels during treatment may indicate progression of IE, although it can also represent a reaction to antibiotics, other inflammatory stimuli or infection with additional pathogens. Thorough clinical evaluation and often repeat TEE is required to assess possible complications, including intracardiac progression. Consequently, a new TEE was performed, which showed an increasing vegetation load (Figure 5). The patient was referred to the department of Cardiothoracic Surgery, where she underwent heart valve surgery involving the replacement of the mechanical mitral valve with a biological valve. Cultures from the mitral valve tissue were negative, but S. zooepidemicus DNA was identified by 16S polymerase chain reaction (PCR). The dual-chamber pacemaker was removed and replaced with a temporary transvenous pace lead. There was no growth of bacteria from the pacemaker leads. The post-surgical period was without further complications.
A transesophageal echocardiography (TEE) of the prosthetic mitral valve with visualization of the progression 23 day after hospital admission and prior to surgery Arrow shows vegetation with measurements
The ejection fraction remained around 35% and the temporary pacemaker showed a 100% pace rhythm with a base rate of 50 beats per minute due to third-degree AV node block. Therefore, a biventricular pacemaker was implanted. A TEE was conducted shortly before the patient was discharged from the hospital. The bioprosthetic valve was functioning well with no paravalvular leaks (see Figure 6 for timeline).
Timeline of investigations, diagnosis, and treatments
Discussion
Herein, we discuss a Danish female patient with IE caused by S. zooepidemicus, a rare bacterium in humans. The patient had several comorbidities and was predisposed to IE due to the presence of a mechanical mitral valve and a dual-chamber pacemaker. She was admitted to the hospital after being found lying confused on the floor at home. Three out of three blood culture bottles were positive for S. zooepidemicus, and the patient was diagnosed with definite IE with two major Duke-International Society for Cardiovascular Infectious Diseases (ISCVD) IE criteria: (1) imaging major criteria with a TEE showing a large vegetation on the posterior leaflet of the mitral valve, and (2) surgical major criteria with evidence of IE by direct inspection during the heart valve surgery [8]. Since *S. zooepidemicus *rarely causes IE and was not isolated in repeated blood cultures, a major microbiological criterion was not fulfilled. However, the IE diagnosis was further supported after surgical removal of the mechanical mitral valve, which showed S. zooepidemicus DNA by 16S PCR. The patient was treated with penicillin, to which the bacteria were sensitive, with a low minimum inhibitory concentration (MIC) value. After the heart valve surgery, moxifloxacin was prescribed at the discretion of the microbiologists.
*S. zooepidemicus *was isolated for the first time in 1933 by P. R. Edwards, and the bacterium was named animal pyogens A [9]. The United States witnessed the first documented outbreak of S. zooepidemicus in humans in 1983. A total of patients had S. zooepidemicus isolated from the bloodstream and presented with symptoms such as fever and chills. The source of infection was identified as cheese made from raw milk by cows who had mastitis due to S. zooepidemicus [10].
Streptococci can be classified into eight main groups [3]. *Streptococcus equi *belongs to the group of “Other Streptococci” and can be further divided into the following three subspecies: *Streptococcus equi *subspecies equi, *Streptococcus equi *subspecies zooepidemicus, and *Streptococcus equi *subspecies ruminatorum [11]. *S. zooepidemicus’ *genome shares over 92% similarity with the genome of Streptococcus equi [6].
Human infections with *S. zooepidemicus *are very rare; however, the colonization of this bacterium in humans mostly leads to severe infections. A study from Finland in 2013 reported three unrelated cases of *S. zooepidemicus *infections among three men, all of whom were working closely with horses. Sepsis occurred in two out of the three men, with one of them also developing meningitis and endocarditis, while the third person experienced purulent arthritis and a psoas abscess. All cases required prolonged antibiotic treatment, surgery, and rehabilitation [7]. These findings are in line with our Danish patient, who had ongoing and close contact with horses and developed a severe infection with several complications, which required prolonged treatment. Both contact with animals and consumption of dairy products have been proposed as entry pathways in previous studies of S. zooepidemicus. Five of these studies suspect close contact with horses [7, 11-14], which is consistent with our patient’s weekly interactions with horses. Nine of the 13 cases included in this report survived [7, 11-18], four died [19-20], and three had to undergo surgical treatment of the implicated valve [7, 11, 14]. This aligns with an overall in-hospital mortality rate of up to about 30%, and a rate for heart valve surgery of about 20-25% in IE patients.
With a MIC value of 0.032mg/l, S. zooepidemicus in our present case was very sensitive to penicillin. According to guidelines, IE on native valves with streptococci with low MIC values can be treated with penicillin in monotherapy [1]. However, due to the severity of the infection, the microbiologists decided to treat the patient with a combination of two antibiotics.
Our patient was diagnosed with pneumonia, meningitis, and IE. These three conditions together constitute a triad that resembles the Austrian syndrome [21]. Austrian syndrome was first described in 1862, prior to the identification of pathogens [22]. The syndrome was later linked to Streptococcus pneumonia in 1975 by Robert Austrian [23]. It has been suggested that the pathophysiology of the syndrome involves septic microemboli, and it is reported that pneumonia often is the first manifestation [21], which aligns with our Danish patient.
A potential underlying mechanism could be the same as indicated by the Austrian syndrome [21], which is that *S. zooepidemicus *colonizes the heart valve by hematogenous spread from the lung. In our case, the patient had prolonged symptoms with coughing and had been treated on the suspicion of a respiratory infection by the general practitioner prior to hospitalization. Furthermore, a PET/CT scan showed F-18-FDG signals in the lungs. A primary focus in the lung could therefore be consistent with hematogenous spread from pneumonia; however, the transmission remains uncertain. A previous study, which investigated 88 cases of Group C streptococci bacteremia, found no specific entry of the bacteria in 34 of the cases but suggests the gastrointestinal tract to be the source of entry in 16 patients, whereas 10 were directly linked to ingestion of contaminated milk, which supports the view of multiple possible entry pathways [24].
Herein, we also present a review of 11 previously described studies of 13 cases of S. zooepidemicus IE (Table 2).
Conclusions
Many different bacteria can cause IE, and Streptococci are often implicated. This case demonstrates that if blood cultures show a zoonotic bacterium, the bacterium’s taxonomic group, followed by determination of the species and the relationship with IE in humans, should be considered to help assess the IE risk. In the present instance, S. zooepidemicus is a hemolytic streptococcus from Lancefield group C known to be associated with horses, but transmission to humans, causing severe infections, including IE, may seldom occur. Therefore, in case of growth of S. zooepidemicus in blood cultures, increased awareness of IE is recommended. In such cases, early echocardiography with extended antibiotic therapy should be considered, especially if there are risk factors of IE such as a prosthetic heart valve or a cardiac implantable electronic device.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 12023 ESC Guidelines for the management of endocarditis Eur Heart J Delgado V Ajmone Marsan N de Waha S 394840424420233762265610.1093/eurheartj/ehad 193 · doi ↗ · pubmed ↗
- 2Temporal changes, patient characteristics, and mortality, according to microbiological cause of infective endocarditis: a nationwide study J Am Heart Assoc Østergaard L Voldstedlund M Bruun NE 011202210.1161/JAHA.122.025801 PMC 949629835946455 · doi ↗ · pubmed ↗
- 3Prevalence of infective endocarditis in streptococcal bloodstream infections is dependent on streptococcal species Circulation Chamat-Hedemand S Dahl A Østergaard L 72073014220203258057210.1161/CIRCULATIONAHA.120.046723 · doi ↗ · pubmed ↗
- 4Distribution of streptococcal groups causing infective endocarditis: a descriptive study Diagn Microbiol Infect Dis Kim SL Gordon SM Shrestha NK 2692729120182956712610.1016/j.diagmicrobio.2018.02.015 · doi ↗ · pubmed ↗
- 5Streptococcal infective endocarditis: clinical features and outcomes according to species Infection Chamat-Hedemand S Dahl A Hassager C 8698795120233615222410.1007/s 15010-022-01929-1 · doi ↗ · pubmed ↗
- 6Complete genome sequence of Streptococcus equi subsp. zooepidemicus strain ATCC 35246 J Bacteriol Ma Z Geng J Zhang H 5583558419320112191489010.1128/JB.05700-11PMC 3187426 · doi ↗ · pubmed ↗
- 7Transmission of Streptococcus equi subspecies zooepidemicus infection from horses to humans Emerg Infect Dis Pelkonen S Lindahl SB Suomala P 104110481920132377775210.3201/eid 1907.121365 PMC 3713971 · doi ↗ · pubmed ↗
- 8The 2023 Duke-International Society for Cardiovascular Infectious diseases criteria for infective endocarditis: updating the modified Duke criteria Clin Infect Dis Fowler VG Durack DT Selton-Suty C 5185267720233713844510.1093/cid/ciad 271PMC 10681650 · doi ↗ · pubmed ↗