Aortopulmonary fistula as a rare complication of bioprosthetic aortic valve endocarditis: a case report
Thomas Saliba, David Rotzinger, Mariama Touray, Guillaume Fahrni

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
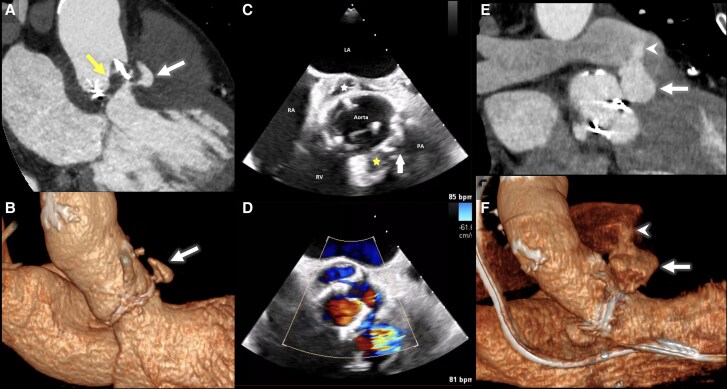 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Aortic and Vascular Conditions · Infective Endocarditis Diagnosis and Management · Aortic Disease and Treatment Approaches
Case description
A 67-year-old man presented for the management of a Staphylococcus lugdunensis bioprosthetic valve endocarditis (PVE).
An ECG-gated cardiac CT angiography (CTA) revealed prosthetic valve degeneration with hypoattenuated leaflet thickening (HALT), complicated by a pseudoaneurysm of the left cusp (Figure 1A and B), resulting in its emergent surgical replacement.
Imaging of prosthetic valve endocarditis complicated by pseudoaneurysm and aortopulmonary fistula. Contrast-enhanced CT scan (CT angiography) (A) and 3D virtual reconstruction (3D VR) (B) showing hypoattenuated leaflet thickening (yellow arrow) and a contained pseudoaneurysm (white arrow) upon admission. Cardiac transoesophageal echocardiogram in B-mode (C) and Doppler mode (D) of the aortic valve acquired post-operatively, revealing pseudoaneurysm (yellow star) with evidence of fistulization to the pulmonary trunk (white arrow). A second, smaller pseudoaneurysm is also visible on the opposite side of the valve (white star). Postoperative CT angiography (E) and 3D virtual reconstruction (F) showing rapid progression in size of the pseudoaneurysm (white arrow) with new-onset fistula to the pulmonary trunk (white arrowhead). LA = left atrium, PA = pulmonary artery, RA = right atrium, RV = right ventricle.
The surgeons discovered vegetations on both the aortic and ventricular surfaces of the prosthetic valve, alongside an annular abscess extending towards the non-coronary commissure, creating a 1-cm cavity between the left and right commissures. The patient underwent debridement of the abscess with resection and repair of the pseudoaneurysm alongside the valvular replacement.
A post-operative transoesophageal echocardiogram (TEE) revealed a pseudoaneurysm of the prosthetic valve, raising suspicion of a fistula between the pseudoaneurysm and the pulmonary artery (Figure 1C and D).
A cardiac CTA was performed the following day, 14 days after the aortic valve replacement, revealing rapid progression of the pseudoaneurysm of the new prosthetic valve and confirmed the presence of a newly formed fistula between the aortic valve and the pulmonary trunk (Figure 1E and F).
The patient passed away 3 days later, following complications of sepsis and strokes.
Aortopulmonary fistula is a rare but life-threatening complication of prosthetic valve endocarditis, associated with high mortality. When PVE occurs, it may lead to the formation of pseudoaneurysms, which are best detected with CTA or TEE.^1^ If a fistula is suspected, invasive coronary angiography should be avoided due to increased risks of adverse events.^2^
Once pseudoaneurysms develop, they can be further complicated by the formation of fistulas, which are perforations caused by erosion between two cavities.^1^ In such cases, TEE is more accurate than CTA due to its superior temporal resolution.^1^
This case underscores the importance of early multimodality imaging in PVE with persistent sepsis as complications such as aorto-pulmonary fistula may develop rapidly despite surgical intervention.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hutt E, Canosa FJM, Unai S, Jaber WA. Manifestations of prosthetic valve endocarditis: lessons from multimodality imaging and pathological correlation. Circ Cardiovasc Imaging 2024;17:e 016435.38626096 10.1161/CIRCIMAGING.123.016435 · doi ↗ · pubmed ↗
- 2Sanchez-Nadales A, Celis-Barreto V, Khan A, Anampa-Guzman A, Olanipekun O. Aorto-cavitary fistula to the left ventricle with severe aortic regurgitation as a complication of prosthetic valve infective endocarditis: a novel report. Oxf Med Case Reports 2020;2020:433–436.