Medical Therapy Algorithm With Telehealth Reduces Procedures and Transfers for Peritonsillar Abscess
Aviv Spillinger, Erin Dimon, Anna Schmidt, Joshua Gauger, Hani I. Kuttab, David O. Francis, Sandra Y. Lin

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
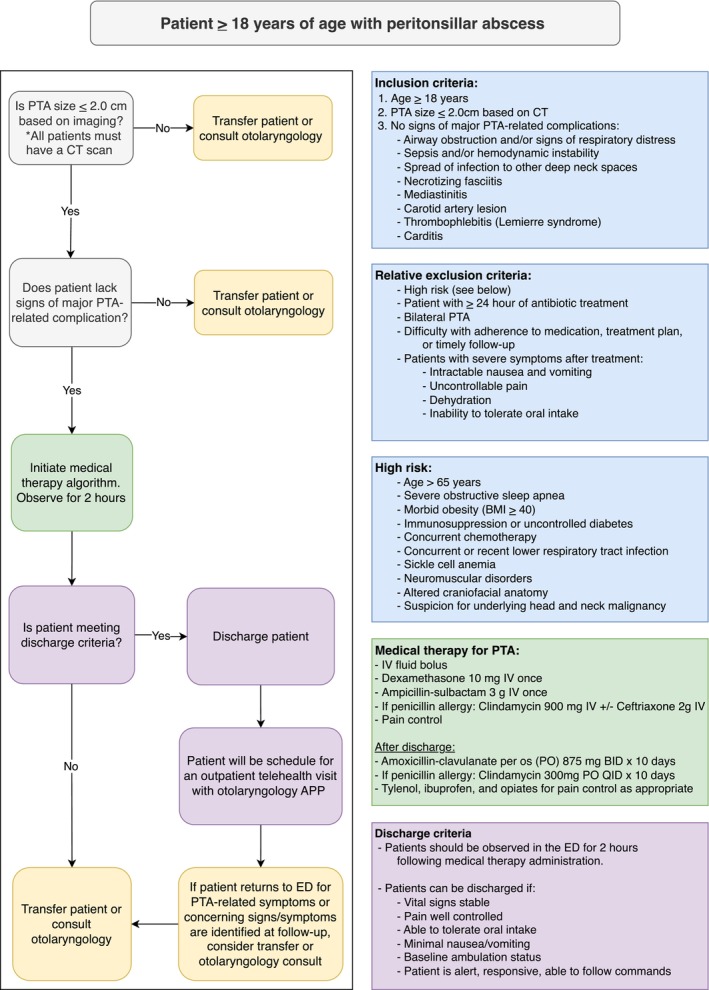 FIGURE 1
FIGURE 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOtolaryngology and Infectious Diseases
Introduction
1
Peritonsillar abscess (PTA) is the most common deep neck space infection with ~45,000 annual cases in the United States and treatment costs exceeding $150 million USD [1]. Standard management typically involves surgical drainage by needle aspiration or incision and drainage [2]. However, emerging evidence suggests that many uncomplicated PTAs can be managed successfully with medical therapy alone [1, 3, 4, 5, 6, 7, 8, 9]. Several centers have adopted primary medical treatment algorithms, demonstrating reduced costs and minimizing overtreatment [1, 3]. This report presents preliminary findings from a quality improvement project evaluating whether a medical therapy algorithm, combined with close telehealth follow‐up, can safely reduce unnecessary procedures and inter‐hospital transfers for patients with small, uncomplicated PTAs.
Methods
2
This study was designated a quality improvement project by the Institutional Review Board (ID: 2023‐0874). A PTA medical therapy algorithm was developed by a multidisciplinary workgroup of emergency medicine physicians, otolaryngologists, and pharmacists based on evidence from prior publications [1, 4, 10] and implemented at a tertiary academic referral center beginning February 2024. Eligible patients presenting to an affiliated emergency department (ED) or requesting transfer from non‐affiliated hospitals were managed according to this algorithm. At affiliated hospitals, the algorithm was embedded in the electronic record, allowing ED providers to initiate medical management without otolaryngology consultation. All transfer requests from non‐affiliated hospitals or from affiliated hospitals without otolaryngology services were reviewed by the on‐call attending otolaryngologists at the tertiary center for potential enrollment.
The algorithm (Figure 1) applied to otherwise healthy adults with new‐onset (i.e., not previously treated) PTA presenting with mild to moderate symptoms and abscess size ≤ 2.0 cm on computed tomography (CT) imaging. A 2 cm cutoff was selected based on prior literature [5, 7] and was agreed upon by the multidisciplinary workgroup as a pragmatic balance between patient safety—by restricting eligibility to lower risk, smaller abscesses—and provider acceptance, by choosing a threshold comfortable for clinicians accustomed to managing nearly all PTAs surgically.
PTA medical therapy algorithm. * is to emphasize that this is an important inclusion criterea. All patients must have a CT scan to be eligble for inclusion. APP, advanced practice provider; BMI, body mass index; CT, computed tomography; IV, intravenous; PO, per os; PTA, peritonsillar abscess. [Color figure can be viewed in the online issue, which is available at www.laryngoscope.com]
Discharged patients were scheduled for a phone or video telehealth follow‐up appointment with an otolaryngology Advanced Practice Provider at the tertiary referral center, ideally within 48 h. Patients also received standardized discharge instructions outlining return precautions and clinic contact information. Outcomes were assessed through follow‐up documentation or, if unavailable, by chart review. Treatment failure was defined as undergoing a salvage procedure (e.g., needle aspiration, incision and drainage) or developing a major PTA‐related complication (e.g., airway obstruction, mediastinitis) within 30 days of initial presentation.
Results
3
Forty‐eight patients were managed according to the algorithm (median age: 35 years; interquartile range: 26–49.5; 50% female). Thirty‐seven patients (77.1%) presented to affiliated hospitals and 11 (22.9%) to non‐affiliated hospitals. Notably, 27 patients (56.3%) presented to hospitals without otolaryngology services, which—prior to the algorithm's implementation—would have traditionally necessitated transfer for surgical drainage. The average distance from non‐affiliated hospitals to the tertiary center was 48.4 miles (range: 22.3–85.2 miles).
Medical therapy alone was successful for 43 (89.6%) patients. No major PTA‐related complications occurred. Five patients (10.4%) experienced treatment failures: four underwent salvage incision and drainage within 48 h of initial presentation, and two required transfers from hospitals without otolaryngology services. Therefore, 25 of 27 patients (92.6%) presenting to hospitals without otolaryngology services were successfully medically managed locally without requiring transfer. Telehealth follow‐up was completed for 28 patients (58.3%), with 16 (33.3%) patients completing follow‐up within 48 h.
Discussion
4
Consistent with prior studies, this report suggests that surgical drainage can often be safely avoided for small (≤ 2 cm), uncomplicated PTAs, potentially reducing morbidity and healthcare costs of inter‐hospital transfers [1, 3, 4, 5, 6, 7]. Southern California Kaiser Permanente Medical Group reported thousands of medically managed PTA cases, citing an 8.1% treatment failure rate [1]. In the present study, the medical treatment failure rate was 10.4%, and inter‐hospital transfers were avoided for 92.6% of patients presenting to hospitals without otolaryngology services. Prior to implementation, our institution typically accepted most transfer requests from hospitals without otolaryngology coverage for surgical drainage of PTAs, including those with small (< 2 cm) abscesses. Although historical transfer rates for small PTAs were not captured and cannot be quantified retrospectively, our findings suggest that the algorithm enabled many of these patients to be safely managed locally without transfer.
To the authors' knowledge, this is the first PTA medical therapy algorithm to incorporate telehealth follow‐up. Telehealth appointments were used to evaluate treatment response, provide further education, and counsel patients on return precautions and signs of treatment failure (e.g., worsening throat or neck pain, worsening trismus, respiratory distress). Additional advantages of telehealth included improved clinic resource utilization and increased convenience for patients, particularly those referred from non‐local hospitals. Although standardized discharge instructions were provided to all patients, scheduled telehealth follow‐up served as an added safeguard by enabling timely reassessment and early recognition of treatment failure.
This report describes preliminary findings from an ongoing prospective quality improvement study, with several limitations. Although standardized inclusion criteria were established, there was variability in decision‐making across providers, and patients from outside non‐affiliated centers were eligible only if the on‐call otolaryngology attending was contacted. Data on transfer calls, excluded patients, and reasons for non‐enrollment were not systematically available.
Conclusion
5
A medical therapy algorithm with close telehealth follow‐up may safely reduce unnecessary procedures and inter‐hospital transfers for small, uncomplicated PTAs. Further patient enrollment will be important to confirm the safety and efficacy of the PTA medical therapy algorithm.
Disclosure
The authors have nothing to report.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A. Battaglia , R. Burchette , J. Hussman , M. A. Silver , P. Martin , and P. Bernstein , “Comparison of Medical Therapy Alone to Medical Therapy With Surgical Treatment of Peritonsillar Abscess,” Otolaryngology—Head and Neck Surgery: Official Journal of American Academy of Otolaryngology‐Head and Neck Surgery 158, no. 2 (2018): 280–286, 10.1177/0194599817739277.29110574 · doi ↗ · pubmed ↗
- 2B. A. Chang , A. Thamboo , M. J. Burton , C. Diamond , and D. A. Nunez , “Needle Aspiration Versus Incision and Drainage for the Treatment of Peritonsillar Abscess,” Cochrane Database of Systematic Reviews 12, no. 12 (2016): CD 006287, 10.1002/14651858.CD 006287.pub 4.28009937 PMC 6463807 · doi ↗ · pubmed ↗
- 3R. H. Lamkin and J. Portt , “An Outpatient Medical Treatment Protocol for Peritonsillar Abscess,” Ear, Nose, & Throat Journal 85, no. 10 (2006): 658–660.17124937 · pubmed ↗
- 4R. F. Johnson , “Emergency Department Visits, Hospitalizations, and Readmissions of Patients With a Peritonsillar Abscess,” Laryngoscope 127, no. Suppl 5 (2017): S 1–S 9, 10.1002/lary.26777.28782104 · doi ↗ · pubmed ↗
- 5M. J. Urban , J. Masliah , C. Heyd , T. R. Patel , and T. Nielsen , “Peritonsillar Abscess Size as a Predictor of Medical Therapy Success,” Annals of Otology, Rhinology and Laryngology 131, no. 2 (2021): 34894211015590, 10.1177/00034894211015590.33980073 · doi ↗ · pubmed ↗
- 6D. Forner , D. E. Curry , K. Hancock , et al., “Medical Intervention Alone vs Surgical Drainage for Treatment of Peritonsillar Abscess: A Systematic Review and Meta‐Analysis,” Otolaryngology‐Head and Neck Surgery 163 (2020): 915–922, 10.1177/0194599820927328.32482146 · doi ↗ · pubmed ↗
- 7D. L. S. Souza , D. Cabrera , W. I. Gilani , et al., “Comparison of Medical Versus Surgical Management of Peritonsillar Abscess: A Retrospective Observational Study,” Laryngoscope 126, no. 7 (2016): 1529–1534, 10.1002/lary.25960.27010228 · doi ↗ · pubmed ↗
- 8Y. P. Wang , M. C. Wang , H. C. Lin , and P. Chou , “The Impact of Prior Tonsillitis and Treatment Modality on the Recurrence of Peritonsillar Abscess: A Nationwide Cohort Study,” P Lo S One 9, no. 10 (2014): e 109887, 10.1371/journal.pone.0109887.25291179 PMC 4188615 · doi ↗ · pubmed ↗