A Novel Intensity-Modulated Radiation Therapy Approach to Reduce Tongue Radiation Dose Using the BinkieRT Intraoral Device: A Case Report
Kanta Shiojima, Seiya Isozaki, Toshiaki Matsui, Takumi Kodama, Shigehiro Kudo

TL;DR
A new device called BinkieRT helps reduce radiation dose to the tongue during oral cancer treatment, potentially improving patient quality of life.
Contribution
The BinkieRT intraoral device is introduced as a novel, practical solution to reduce tongue radiation dose during IMRT for oral cancer.
Findings
BinkieRT displaced the tongue and reduced radiation dose to the tongue and oral mucosa without affecting target coverage.
BinkieRT offers advantages over handmade spacers in terms of ease of use, hygiene, and reproducibility.
The device's design is noninvasive and suitable for various clinical scenarios, including elderly patients and re-irradiation cases.
Abstract
Radiation therapy plays a pivotal role in the management of oral cancer. However, radiation-induced mucositis and dysgeusia frequently impair patients’ quality of life. To mitigate these risks, intraoral positioning devices have been introduced to minimize radiation exposure to the oral organs at risk. We report a case of recurrent buccal mucosa cancer treated with intensity-modulated radiation therapy (IMRT) using a commercial intraoral device, BinkieRT (Paprica Lab., Seoul, Republic of Korea). The device displaced the tongue contralaterally and separated the oral cavity from the target volume, leading to a reduction in radiation dose to the tongue and oral mucosa without compromising target coverage. Compared with handmade spacers or bite blocks, BinkieRT offers distinct advantages in terms of ease of use, hygiene, and reproducibility. The observed immediate dosimetric improvement…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
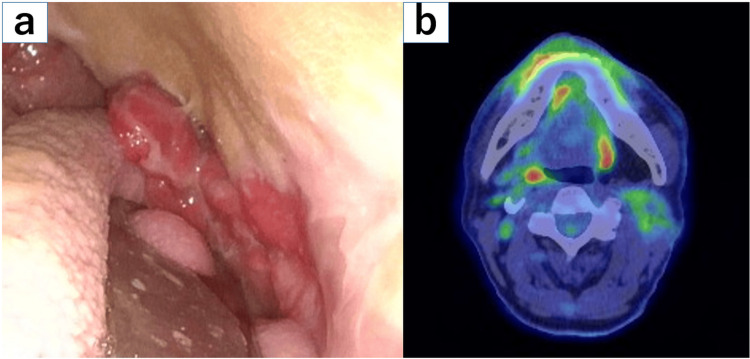 Figure 1
Figure 1 Figure 2
Figure 2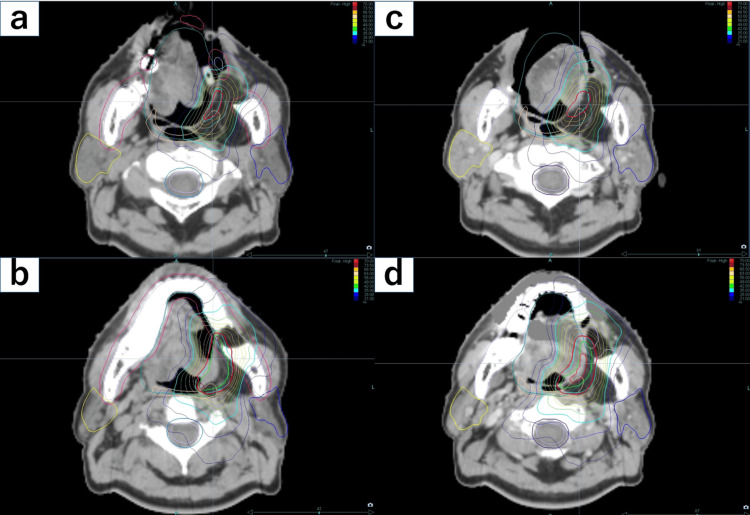 Figure 3
Figure 3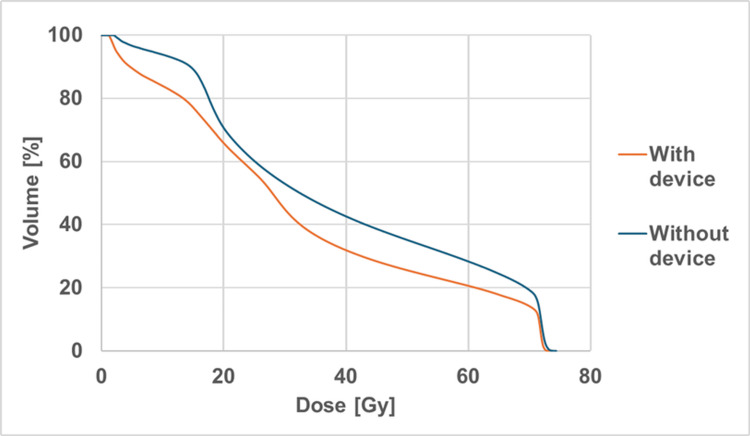 Figure 4
Figure 4 Figure 5
Figure 5| Parameters | With device | Without device |
| V15Gy(%) | 72.9 | 88.2 |
| V30Gy(%) | 38.8 | 52.5 |
| V45Gy(%) | 26.8 | 38.4 |
| V60Gy(%) | 20.0 | 28.3 |
| V70Gy(%) | 14.3 | 19.5 |
| Dmax(Gy) | 73.89 | 74.83 |
| Dmean(Gy) | 31.38 | 38.79 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOral health in cancer treatment · Head and Neck Cancer Studies · Effects of Radiation Exposure
Introduction
Radiation therapy (RT) plays an important role in the management of head and neck cancers, including oral cancer. However, radiation-related adverse events (e.g., oral mucositis, dysphagia, dysgeusia, and xerostomia) remain major clinical concerns. Studies have shown that increased radiation dose to the oral cavity, including the tongue, is associated with the incidence and severity of these adverse events [1-3]. To mitigate these risks, several intraoral devices have been developed to reposition the tongue and spare surrounding healthy tissues [4-6]. This case report describes the dosimetric benefits of using the commercial intraoral positioning device BinkieRT (Paprica Lab., Seoul, Republic of Korea) during intensity-modulated radiation therapy (IMRT) in a patient with recurrent buccal mucosa cancer. We compared dose-volume histograms (DVHs) of the tongue obtained with and without the device to verify reductions in radiation exposure to critical structures. To the best of our knowledge, no previous studies have compared tongue-body DVHs with and without the use of BinkieRT.
Case presentation
The patient was a 67-year-old man with no remarkable medical or family history. He had a 25-year history of smoking 40 cigarettes per day. Two years prior, he had undergone surgery for left buccal mucosal squamous cell carcinoma (cT3N0M0, stage III). At one year and 11 months after surgery, local recurrence was identified in the caudal portion of the reconstructive skin flap, and he was referred to our department for cisplatin-based chemoradiation therapy. At the time of the presentation, his performance status was 0, and he was asymptomatic with a generally good condition. Imaging studies revealed that the recurrent lesion was confined to the caudal portion of the left buccal mucosal flap. Following deliberation with the surgical team, the decision was taken that prophylactic neck irradiation was not required, given the prior neck dissection and the fact that this represented a purely local recurrence 1 year and 11 months after surgery. Because the radiation field was limited to this area, he was considered a suitable candidate for intraoral device therapy using BinkieRT (Figure 1).
Local recurrence at the inferior margin of the flap after surgery for left buccal mucosa carcinoma.(a) A flexible nasopharyngeal laryngoscopic view showing an irregular elevated lesion at the flap margin. (b) FDG-PET image demonstrating focal uptake corresponding to the recurrent lesion.
This study was reviewed and approved by the ethics review board of our institution (Approval Number: 2171). Written informed consent was obtained from the patient for publication of this report and the accompanying images.
A C-type BinkieRT was used to displace the tongue toward the right, opposite the left buccal mucosa (Figure 2).
A tongue positioning device (BinkieRT Type C) featuring a C-shaped paddle blade. (width 26 mm, depth 87.8 mm).Permission to reproduce this image was obtained from Paprica Lab [7].
Planning CT scans were acquired both with and without the device, with thermoplastic mask immobilization in each case. Target contouring was performed using the Monaco® version 5.11.03 treatment planning system (Elekta AB, Stockholm, Sweden). The gross tumor volume (GTV) was delineated based on flexible nasopharyngeal laryngoscopy, MRI, and FDG-PET findings. The clinical target volume (CTV) was defined as the GTV plus a margin of 5-10 mm, excluding anatomical barriers. The device was positioned between the buccal mucosa and the tongue, allowing clearer delineation of these structures and improved CTV definition. Irradiation was confined to the local site with daily CBCT-based image guidance. Furthermore, the BinkieRT device ensured consistent compression and stabilization of the buccal mucosa, thereby minimizing intra-fractional internal motion. Consequently, the planning target volume (PTV) margin was reduced from 3 mm (without the device) to 2 mm (with the device). The tongue was delineated as an organ at risk (OAR), with its inferior border defined at the level of the superior margin of the hyoid bone. Although tongue morphology differed between the two CT sets, the total contoured tongue volumes were approximately equivalent. An IMRT plan was created using the Precision® version 3.3.1.3 planning system (Accuray Inc., Sunnyvale, CA, USA). The prescribed dose was 70 Gy in 35 fractions. The plan ensured that 95% of the PTV received 100% of the prescribed dose (D95%) while minimizing the tongue OAR dose, and that the PTV volume receiving ≥105% of the prescribed dose did not exceed 1 cm³. Treatment was delivered using TomoTherapy® (Accuray Inc.) with 6 MV X-rays.
Dose distributions with and without the device are shown in Figure 3.
Axial dose distributions (a)(b) with and (c)(d) without the BinkieRT device.Use of the BinkieRT device effectively reduced the tongue dose by displacing the tongue away from the target volume.
DVH parameters for the tongue OAR, including the percentage of volume receiving 15, 30, 45, 60, and 70 Gy (V15-V70), maximum dose (Dmax), and mean dose (Dmean), are summarized in Table 1 and Figure 4.
A comparison of DVH parameters of the tongue in IMRT plans with and without the BinkieRT device.
DVH analysis demonstrated reductions in V15-V70 and Dmean with the device, whereas Dmax was comparable between the two plans. The observed dose reduction was likely attributable to tongue displacement away from the irradiation field, improved visualization of the buccal mucosa-tongue interface, and a smaller PTV margin due to enhanced setup accuracy.
The actual treatment was administered using a plan created with the BinkieRT device in place. According to the Common Terminology Criteria for Adverse Events (CTCAE) v6.0, grade 1 oral mucositis developed on day 21 at a cumulative dose of 28 Gy, followed by grade 2 dysgeusia and grade 1 xerostomia on day 42 at a cumulative dose of 58 Gy. Although the patient reported mild pain associated with mucositis, he continued to tolerate the intraoral device without difficulty, and radiotherapy was completed as planned without interruption. Two months after treatment completion, mucositis had fully resolved. Despite the persistence of mild dysgeusia and xerostomia, he was able to maintain oral intake comparable to his pretreatment level. Flexible nasopharyngeal laryngoscopy at that time confirmed a near-complete macroscopic response of the tumor (Figure 5).
Flexible nasopharyngeal laryngoscopy at two months post-treatment showing a near-complete response of the tumor.
Discussion
This case demonstrates that the tongue positioning device BinkieRT can substantially reduce radiation dose to the tongue and oral cavity during IMRT for oral cancer. Dose reduction to oral OARs is clinically important because radiation-induced toxicities such as mucositis, dysphagia, and dysgeusia occur in a dose-dependent manner [1-3]. Therefore, minimizing the dose to these structures may contribute to preserving patients’ quality of life.
Several prior studies have reported the benefits of tongue positioning for OAR sparing. Kil et al. showed significant reductions in tongue dose with a “stick-out tongue” position [8], and Ikawa et al. demonstrated that a tongue depressor-equipped mouthpiece helped prevent lingual mucositis [5]. Hong et al. further described a semi-custom intraoral device fabricated using a 3D printer [6]. Compared to these devices, BinkieRT is highly practical due to its ease of use and its capacity to effectively reduce radiation exposure to the tongue and oral cavity.
While X-ray-based IMRT has limitations in reducing doses to OARs and cannot achieve the superior dose sparing of intensity-modulated proton therapy (IMPT) [9,10], the clinical availability of IMPT remains limited due to the small number of facilities capable of delivering it. The combination of X-ray-based IMRT with a simple intraoral device such as BinkieRT may provide a more accessible, cost-effective, and practical means of dose reduction.
Previous reports have described intraoral devices that require 3D printing or dental intervention, which can be time-consuming and technically demanding [11,12]. In contrast, BinkieRT requires no special preparation and can be implemented immediately in daily clinical practice. Furthermore, its fixation accuracy and reproducibility have already been validated by a Korean group [13], supporting its reliability for routine use.
The limitation of this report includes its single-case nature, which precludes assessment of long-term outcomes or late toxicities. Further accumulation of clinical cases and prospective evaluations is warranted to confirm the efficacy and safety of BinkieRT-assisted RT.
Conclusions
BinkieRT facilitated noninvasive, immediate reduction of radiation dose to the tongue and oral cavity during IMRT for oral cancer. This may help prevent radiation-induced oral toxicities and maintain patients’ quality of life. BinkieRT requires no special skills and can be implemented immediately, thereby possibly serving as a simple and practical adjunctive tool for daily clinical use.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gorham-Stout disease with involvement of the jaws: a systematic review Int J Oral Maxillofac Surg Chrcanovic BR Gomez RS 101510214820193089843010.1016/j.ijom.2019.03.002 · doi ↗ · pubmed ↗
- 2Impact of radiation dose on patient-reported acute taste alteration in a prospective observational study cohort in head and neck squamous cell cancer (HNSCC)Radiol Med Morelli I Desideri I Romei A 1571157912820233764281610.1007/s 11547-023-01707-5PMC 10700473 · doi ↗ · pubmed ↗
- 3Mean oral cavity organ-at-risk dose predicts opioid use and hospitalization during radiotherapy for patients with head and neck tumors Cancers (Basel) Foote RL Harmsen WS Amundson AC 16202410.3390/cancers 16020349 PMC 1081407438254837 · doi ↗ · pubmed ↗
- 43D-printed individualized tooth-borne tissue retraction devices compared to conventional dental splints for head and neck cancer radiotherapy: a randomized controlled trial Radiat Oncol Held T Herpel C Schwindling FS 751620213386540110.1186/s 13014-021-01803-8PMC 8052727 · doi ↗ · pubmed ↗
- 5A custom-made mouthpiece incorporating tongue depressors and elevators to reduce radiation-induced tongue mucositis during carbon-ion radiation therapy for head and neck cancer Pract Radiat Oncol Ikawa H Koto M Ebner DK 0318201810.1016/j.prro.2017.10.00929291964 · doi ↗ · pubmed ↗
- 6Development of a semi-customized tongue displacement device using a 3D printer for head and neck IMRT Radiat Oncol Hong CS Oh D Ju SG 791420193108847210.1186/s 13014-019-1289-x PMC 6515618 · doi ↗ · pubmed ↗
- 7Paprica Lab: Binkie RT 12 2025 2025 https://papricalab.com/en/tongue-positioning-device/
- 8Decreased radiation doses to tongue with "stick-out" tongue position over neutral tongue position in head and neck cancer patients who refused or could not tolerate an intraoral device (bite-block, tongue blade, or mouthpiece) due to trismus, gag reflex, or discomfort during intensity-modulated radiation therapy Oncotarget Kil WJ Kulasekere C Derrwaldt R Bugno J Hatch C 5302953036720162744797310.18632/oncotarget.10621 PMC 5288166 · doi ↗ · pubmed ↗