Technology-enhanced compression and AI-integrated lymphedema care: a narrative review
Amany Gomaa Atiaa, Mostafa M. Mostafa, Doha El-Sayed Ellakwa

TL;DR
This review explores how digital health and advanced compression technologies, combined with AI, are improving lymphedema care by offering personalized and accessible treatment options.
Contribution
The paper highlights the integration of AI and digital health tools into lymphedema management as a novel approach to enhance care delivery.
Findings
AI tools show promise in risk stratification and personalized treatment planning for lymphedema.
Digital platforms improve patient engagement and long-term adherence to lymphedema care.
Advanced compression devices with sensors and feedback mechanisms enhance therapeutic outcomes.
Abstract
Lymphedema is a persistent and often debilitating condition resulting from lymphatic system dysfunction. It frequently develops as a secondary complication, especially after cancer treatments. Traditional management, centered on complete decongestive therapy (CDT), offers modest benefits but is limited by accessibility, long-term adherence, and variable patient response. This narrative review explores how digital health and enhanced compression technologies are reshaping lymphedema care. A comprehensive review of pertinent literature was conducted to assess the utilization of artificial intelligence (AI), telehealth platforms, mobile applications, virtual reality-based rehabilitation, and advanced compression devices in the management of lymphedema. Focus was directed towards their clinical efficacy, patient-centered advantages, and the challenges associated with their implementation.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
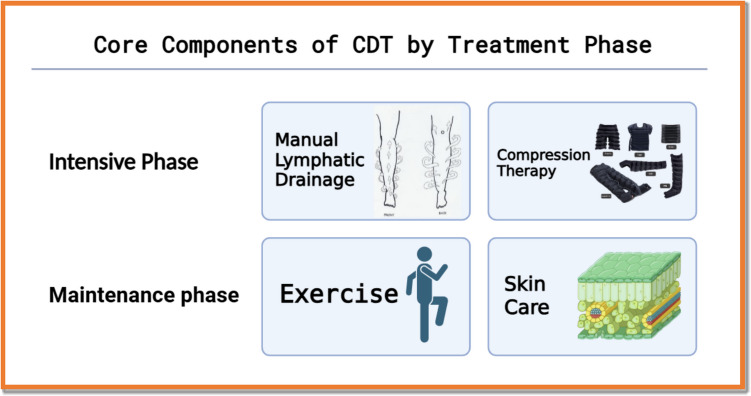 Figure 1
Figure 1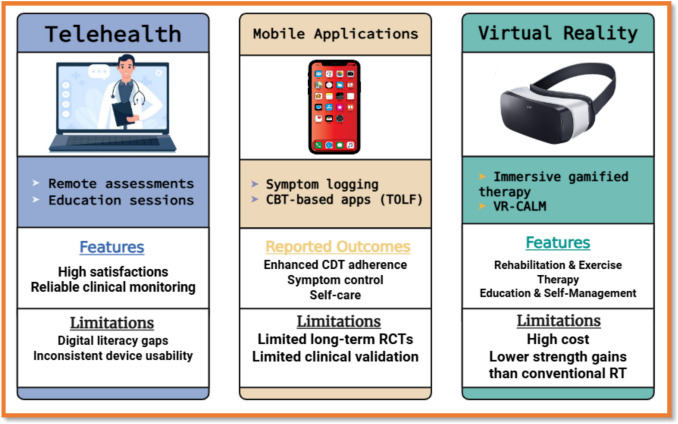 Figure 2
Figure 2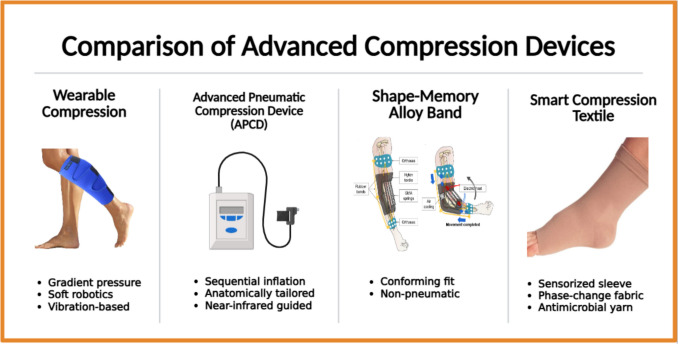 Figure 3
Figure 3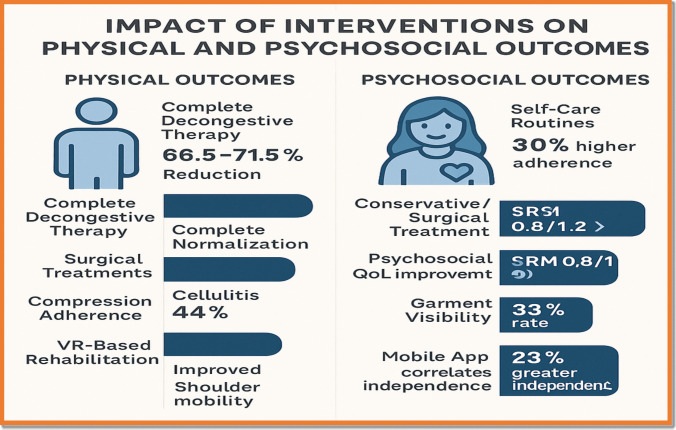 Figure 4
Figure 4 Figure 5
Figure 5- —Sinai University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLymphatic System and Diseases · Diagnosis and Treatment of Venous Diseases · Venous Thromboembolism Diagnosis and Management
Introduction
Lymphedema is a chronic, progressive disorder resulting from the mechanical failure of the lymphatic system to drain protein-rich interstitial fluid effectively [1]. This dysfunction leads to persistent tissue swelling, dermal fibrosis, and significant impairments in physical function [2, 3]. Clinically, lymphedema is classified as either primary—stemming from congenital or genetic anomalies of lymphatic architecture—or secondary, which arises from acquired disruptions such as cancer surgery, lymphadenectomy, radiation therapy, trauma, infection, or systemic disease [4–7]. Secondary lymphedema represents the vast majority of cases and is especially prevalent among individuals undergoing oncologic treatments for breast, gynecologic, prostate, and head and neck cancers [8, 9]. The epidemiological burden of secondary lymphedema is substantial yet varies by cancer type, therapeutic protocol, and geographic setting. For instance, the prevalence of upper-limb lymphedema following breast cancer treatment ranges from 3 to 87%, with most estimates converging between 20 and 49% over a 10-year period [10–14]. In low- and middle-income countries, lower-limb lymphedema occurs in approximately 10% of women post-gynecologic cancer therapy, while nearly 29% of prostate cancer survivors receiving combined radiation and surgery report genital or lower-limb lymphedema [15]. Head and neck cancer survivors present with some of the highest rates, exceeding 75%, often involving both external and internal edema that severely compromises function and quality of life [15],Ellakwa D et al., [16]). Nevertheless, true prevalence is likely underreported due to heterogeneity in diagnostic criteria, inconsistent measurement techniques, and data capture limitations. U.S. insurance claims, for example, estimate an incidence of just 0.95% to 1.24% across all cancer types [17, 18]. Beyond the physical sequelae—such as limb heaviness, restricted mobility, and heightened infection risk—lymphedema imposes a substantial psychosocial burden [19]. Affected individuals frequently experience anxiety, depression, stigma, and social withdrawal, further diminishing functional capacity, social participation, and quality of life [20],“Overview of Lymphedema for Physicians and Other Clinicians,” 2022; [7, 8]. The cornerstone of current non-surgical management is complete decongestive therapy (CDT), which integrates manual lymphatic drainage (MLD), compression therapy, targeted exercise, and meticulous skin care. While MLD techniques facilitate lymph flow and offer moderate reductions in limb volume, their long-term efficacy is variable [9, 13]. Compression garments and multilayer bandages are central to edema maintenance, and therapeutic exercise supports lymphatic return and mobility [21]. Rigorous skin hygiene is also critical to prevent recurrent infections such as cellulitis (Ellakwa D et al., [22],“Overview of Lymphedema for Physicians and Other Clinicians,” 2022. Despite CDT's central role, several barriers impede its effectiveness: inconsistent protocols, limited standardization of diagnostics, poor long-term adherence, and uneven access to trained therapists [23–25]. Surgical options such as lymphovenous bypass and vascularized lymph node transfer offer hope for advanced or refractory cases, yet their adoption is constrained by cost, availability, and procedural complexity (De Senna Nogueira Batista & Chang, [26–28],). Furthermore, self-management approaches are often psychologically burdensome and inadequately supported by health systems, particularly in underserved settings [29, 30].
In response to these unmet clinical needs, a paradigm shift is underway—toward patient-centered, technology-enabled models of care [31]. Emerging innovations such as artificial intelligence (AI)**–**based risk stratification, telehealth-delivered rehabilitation, and sensorized compression technologies promise to enhance early detection, personalize treatment, and improve adherence across diverse populations [4–6, 27, 28, 32]. These convergent technologies herald a new era of lymphedema management—more predictive, participatory, and equitable in scope [33, 34].
Study design and scope
This review adopts a narrative synthesis methodology to evaluate recent innovations in the physical therapy management of secondary lymphedema. It focuses specifically on the integration of digital health technologies and next-generation compression systems. The objective is to critically appraise emerging modalities that may enhance patient outcomes, improve adherence, and expand accessibility relative to traditional care models.
Literature search strategy
A structured literature search was conducted across four major electronic databases—PubMed, Scopus, Web of Science, and Google Scholar—to identify relevant publications from January 2016 to June 2025. The search strategy combined keywords and Medical Subject Headings (MeSH), including: “lymphedema,” “complete decongestive therapy,” “digital health,” “telehealth,” “artificial intelligence,” “compression therapy,” “wearable devices,” and “rehabilitation technology.” These terms were combined with corresponding MeSH terms to enhance the accuracy and comprehensiveness of the search.
Inclusion and exclusion criteria
Studies were included if they met the following criteria:
- Focused on physical therapy interventions for secondary lymphedema, particularly following oncologic treatment.
- Explored digital or technological innovations, such as telehealth platforms, mobile applications, virtual reality (VR) tools, or advanced compression devices (e.g., sensorized garments, pneumatic sleeves).
- Reported empirical outcomes, including limb volume reduction, adherence rates, usability, or device performance.
Studies were excluded if they:
- Focused exclusively on primary lymphedema.
- Were not published in English**.**
- Consisted only of editorials, expert opinions, or abstracts without empirical data**.** “Studies not published in English were excluded due to potential language barriers that may affect the accuracy of translation and interpretation of study findings. Additionally, to ensure consistency in data analysis and quality assessment, English was set as the primary language criterion for the review, as the majority of relevant literature in this field is published in English. However, non-English studies may be considered if reliable translations are available or if review studies include literature published in other languages.”
Data extraction and thematic synthesis
Data were extracted on the following domains:
- Study design and population characteristics
- Type of intervention and technological features
- Outcomes measured (e.g., limb volume, adherence, quality of life)
- Reported limitations
Findings were synthesized thematically under three domains:
- Clinical effectiveness
- User engagement and adherence
- Implementation challenges
Quality assessment
To enhance methodological transparency, each included study underwent quality appraisal appropriate to its design:
- Randomized controlled trials (RCTs) were assessed using the Cochrane Risk of Bias Tool.
- Observational studies were evaluated via the Newcastle–Ottawa Scale.
- Systematic reviews and meta-analyses were reviewed qualitatively for methodological rigor, transparency, and potential bias.
Ethical considerations
As this study involved only secondary analysis of publicly available, peer-reviewed literature, no ethical approval or informed consent was required.
Current standards in lymphedema physical therapy
This section outlines the non-surgical standard of care—complete decongestive therapy (CDT)—its component interventions, clinical efficacy, and associated limitations.
Overview of complete decongestive therapy (CDT)
CDT remains the gold standard conservative treatment for lymphedema and is delivered in two phases. The core elements of CDT, stratified by treatment phase, are shown in Fig. 1.
- Intensive phase: conducted by certified lymphedema therapists.
- Maintenance phase: managed by patients through home-based regimens. Fig. 1. Core components of complete decongestive therapy (CDT) by treatment phase
The four core components of CDT are the following:
- Manual lymphatic drainage (MLD): gentle, rhythmic massage techniques to promote lymph flow and reduce interstitial fluid accumulation.
- Compression therapy: use of bandages or garments to maintain decongestion and prevent fluid re-accumulation.
- Therapeutic exercise: enhances lymphatic return, joint mobility, and muscle function when performed under compression.
- Skin care: critical for infection prevention, especially cellulitis, due to compromised dermal barriers.
The intensive phase includes therapist-led MLD and compression therapy. The maintenance phase relies on patient-managed exercise and skin care**.**
Evidence base for CDT
Several systematic reviews and RCTs support CDT’s efficacy in reducing limb volume and improving functional outcomes. Quantitative outcomes from key studies demonstrating CDT-related limb volume reductions are summarized in Table 1:
- Upper limb volume reductions of ~ 66.5% were observed in a Greek cohort treated with MLD and compression [35].
- Lower limb reductions up to 71.5% were documented in gynecologic cancer survivors [36]. Additional studies cite improvements in fatigue, sleep, and quality of life metrics [43, 44], Ellakwa D et al., [58]). The following table summarizes key studies on CDT volume reduction, limb treated, sample size, and relevant technological enhancements or AI integration. While most studies focus on cancer-related lymphedema, direct evidence for burn injury–related lymphedema with technology-enhanced or AI-integrated care is limited in the current literature. Table 1CDT volume reduction by study, limb, and sample sizeStudyLimb treatedVolume reduction (%)Sample sizePopulation/notes[35]Upper limb ~ 66.5%72Greek population, breast cancer–related[36]Lower limb ~ 71.5%40Post-gynecologic cancer[37, 38]Lower limb ~ 68%Meta-reviewSystematic review across multiple studies[39]Lower limb34% (median)222Primary lymphedema[40]Lower limb11.7% (IPC + CDT), 5.0% (CDT)50Pre-surgical lymphedema[41]Upper limb47.2% (CB), 47.4% (CDT)51Postmastectomy[37, 38]Lower limb45–70%Systematic reviewSystematic review[42]Upper/Lower limb ~ 941 mL (Coban2), ~ 814 mL (standard)264Multicountry, mixed etiology[43, 44]Upper limbModerate effect13 SRsFocus on breast cancer-related lymphedema (BCRL)[45]Lower limbSignificant (not % specified)103Elderly[46]Upper limb38.1%37Focus on breast cancer-related lymphedema (BCRL)[47]MixedEffective (not % specified)ReviewReview[48, 49]Lower limbSignificant (not % specified)60Advanced secondary[50]Upper limbSignificant (not % specified)61Focus on breast cancer-related lymphedema (BCRL)[51]Upper limb31.4% to 19.1% ~ 65%Focus on breast cancer-related lymphedema (BCRL)[52]Lower limbSignificant (not % specified)90Mixed etiology[53]Mixed45–70% (range)ReviewReview[38]Lower limbSignificant (not % specified)15Lower limb[54]Lower limbSignificant (not % specified)356Lower limb[55]Lower limbSignificant (not % specified)7Lower limb[56]Upper limbModerate effectMeta-analysisFocus on breast cancer-related lymphedema (BCRL)[57]Upper limbModerate effectMeta-analysisFocus on breast cancer-related lymphedema (BCRL)
Limitations of traditional approaches
While complete decongestive therapy (CDT) remains the cornerstone of lymphedema management, its scalability and long-term sustainability are hampered by several systemic and patient-level barriers. Limited access to trained therapists is a persistent challenge, especially in rural or low-resource settings, where geographic disparities and workforce shortages restrict the availability of specialized care [30]. Financial barriers further compound these issues, as the costs associated with ongoing therapy, compression garments, and follow-up visits are often inadequately covered by insurance, placing a significant burden on patients and families [59].
Adherence challenges are also prominent; the complexity and time demands of daily regimens—including manual lymphatic drainage, multilayer bandaging, and prescribed exercise—can lead to psychological fatigue, logistical difficulties, and ultimately, suboptimal compliance [2, 3, 30]. For those with advanced or fibrotic lymphedema, the efficacy of CDT plateaus, with only modest improvements possible, and long-term success is heavily dependent on sustained maintenance and support [2, 3, 37, 38].
Individual variability in response to CDT is substantial, influenced by factors such as age, comorbidities, and the chronicity or severity of disease, which can alter tissue characteristics and diminish treatment effectiveness [2, 3, 60]. Finally, evidence gaps persist: many studies evaluating CDT are limited by small sample sizes, short follow-up periods, and inconsistent protocols, undermining confidence in the generalizability and durability of reported outcomes [2, 3, 61, 62]. These limitations underscore the need for more robust, accessible, and individualized approaches to lymphedema care. A comparison of conventional CDT with emerging technological approaches is summarized in Table 2. Table 2. Comparison of traditional CDT vs. digital and compression innovationsFeatureConventional CDTDigital and compression innovationsTherapy componentsMLD, compression garments, exercise, skin careSensorized garments, pneumatic pumps, VR-assisted exercise, and AI monitoringDelivery modeIn-person, therapist-dependentHybrid or remote (telehealth, mobile apps, IoT-enabled devices)MonitoringManual volume tracking, clinical visitsReal-time biosensor feedback, automated data capture, remote dashboardsAdherence supportPatient-led, low-techApp reminders, gamification, smart alertsCustomizationThe therapist adjusted manuallyAI-driven personalization, adaptive pressure systemsAccess and equityLimited in rural/LMIC settingsPotentially scalable, but it depends on digital literacy and infrastructureClinical evidence baseModerate; volume reduction and QOL benefits establishedGrowing evidence; early RCTs and implementation studies emergingLimitationsTherapist shortages, high recurrence risk without follow-upCost, data privacy, and validation across populations
Digital health interventions in lymphedema management
The landscape of lymphedema care is undergoing a paradigm shift with the emergence of digital health interventions. These technologies offer novel modalities for patient engagement, education, early detection, and remote monitoring. This section synthesizes current advancements in telehealth, mobile platforms, and virtual reality (VR) based rehabilitation [63].
Telehealth and remote monitoring
Applications in follow-up, education, and early detection
Telehealth has significantly enhanced postoperative follow-up, patient education, and early detection of lymphedema complications (Ellakwa D et al., [64]). Both synchronous and asynchronous platforms support clinical surveillance and health education, with virtual attendance rates comparable to in-person visits—particularly among breast cancer survivors at risk of lymphedema [4–6, 65]. Telerehabilitation also demonstrates strong clinical validity, with tele-assessments showing high reliability (α = 0.90) and inter-rater agreement (ρ = 0.89), closely matching traditional evaluations [66]. Remote monitoring technologies—including wearable volume sensors and adjunctive treatment devices—enable earlier detection of subclinical lymphedema and support timely intervention [67]. Large-scale telemonitoring programs have also demonstrated clinical impact (Ellakwa D et al., [68]). For example, in a cohort of 1,556 oncology patients (approximately 50% with breast cancer), adverse events were reported in 94.8% of cases, including 27.7% classified as severe [69]. Nevertheless, adherence to digital reporting remained high (79.6% at 3 months), supporting the role of telehealth in preserving treatment continuity [70].
Satisfaction, accessibility, and usability challenges
Patients consistently report high satisfaction with telehealth due to improved convenience and accessibility—particularly in remote or mobility-limited populations [65]. Clinicians also benefit from flexibility and scalable monitoring, especially in resource-limited settings [71–74]. Nonetheless, barriers persist: digital literacy gaps, limited technology access, and inconsistent user interfaces continue to affect scalability and equity [65, 73, 74]. Social network–based platforms such as Telegram™ have shown comparable improvements in quality of life (QoL) to in-person education programs, effectively managing fear of recurrence, although traditional group sessions yielded slightly better psychosocial outcomes [75].
Mobile applications and web-based platforms
Key functions: education, symptom logging, and behavior change
Mobile health (mHealth) tools increasingly support patient-led lymphedema management. Key functionalities include guided exercises, educational content, symptom tracking, therapeutic reminders, and cognitive-behavioral reinforcement. One notable example is the optimal lymph flow (TOLF) app, which leverages behavioral science to promote lymphatic health. In a randomized controlled trial, the TOLF app significantly reduced both symptom severity and arm volume variations compared to controls (Du et al., [71, 72, 76]).
Usability studies confirm high acceptance among users, who value the platforms for their simplicity, convenience, and integration into daily routines [77–79].
Clinical outcomes: adherence, functionality, and evidence gaps
mHealth interventions have demonstrated improvements in CDT adherence, symptom relief, and functional independence. For instance, a WeChat-based CDT training program for breast cancer survivors led to greater self-management capacity and improved QoL [80, 81]. Delphi-designed apps show strong clarity and clinical relevance [82].
However, despite promising user engagement, direct evidence for reducing lymphedema incidence or severity remains limited [83]. Systematic reviews consistently call for high-quality, longitudinal trials to validate long-term clinical effectiveness [84, 85].
Virtual reality–based therapies
VR applications for exercise and motor recovery
Virtual reality–based therapies offer immersive, gamified rehabilitation environments. These interventions promote upper-limb mobility, reduce pain, and improve psychological outcomes. Multiple studies demonstrate that VR significantly enhances shoulder mobility (flexion, abduction, rotation), especially when initiated early [86, 87]. Users often perceive VR training as interactive and therapist-like, enhancing motivation and adherence [88, 89].
When augmented with robotic devices, VR also supports proprioception and dynamic coordination during recovery [87].
Psychosocial and physical outcomes
Compared with traditional resistance training (RT), VR shows superiority in pain control and QoL outcomes. Programs such as VR-CALM effectively reduce anxiety, fatigue, and sleep disturbances [90, 91]. However, traditional RT may still outperform VR in improving handgrip strength and overall muscle performance [86]. While VR enhances dynamic postural control, evidence for improvements in static control is inconsistent [92]. A comparative summary of key digital interventions—including core features, reported outcomes, and limitations—is provided in Table 3. These findings are visually summarized in Fig. 2, illustrating the functional domains and comparative strengths of each digital modality. Table 3. Comparison of digital health interventions in lymphedema careIntervention typePrimary featuresReported outcomesLimitationsCitationsTelehealthRemote assessments, education, video consultsHigh satisfaction, reliable monitoring, improved accessDigital literacy gaps, device usability[10, 11, 93, 94]Mobile appsSymptom logging, CBT-based (TOLF), remindersEnhanced CDT adherence, better self-care, symptom controlLimited long-term RCTs, clinical validation[93, 94]Virtual realityImmersive therapy, VR-CALMImproved mobility, QoL, anxiety reliefHigh cost, less strength gain vs. RT[19]AI-integrated compressionAutomated pressure adjustment, remote dataOptimized edema control, early alertsTraining bias, insurance coverage[19]Wearable sensorsContinuous limb volume, activity trackingEarly detection, personalized feedbackInteroperability with EHRs[93, 94]Remote mentor supportOnline dashboard, PA monitoringIncreased activity, reduced limb volumeAttrition, tech access[93, 94]Intermittent pneumatic compression (APCD)Home-based, digital logsComparable to manual therapy, improved convenienceDevice fit, comfort[10, 11, 95]Digital volume measurement3D scanning, PerometerAccurate, objective trackingCost, training[95]Online education modulesSelf-management, video guidesImproved knowledge, self-efficacyEngagement varies[93, 94]Automated alertsSMS/email remindersReduced complications (e.g., cellulitis)Alert fatigue[93, 94]AI risk stratificationPredictive analyticsEarly intervention, tailored careDataset diversity[19]Gamified exercise appsMotivation, adherenceIncreased exercise, better outcomesUsability, engagement[93, 94]Remote compression adjustmentApp-based controlPersonalized therapy, convenienceConnectivity issues[19]Digital CBTIntegrated mental healthReduced anxiety, improved QoLAccess, privacy[93, 94]EHR integrationData sharing, care coordinationStreamlined care, reduced errorsInteroperability[93, 94]AI-driven imagingAutomated limb analysisEarly detection, objective dataValidation needed[19]Home-based AECTExercise + compression, remote trackingImmediate volume reductionShort-term data[96]Digital peer supportOnline forums, chatSocial support, adherenceModeration, misinformation[93, 94]Virtual clinicsMultidisciplinary, remoteComprehensive care, reduced travelTech barriers[93, 94]AI-enhanced decision supportClinical recommendationsImproved outcomes, efficiencyAlgorithm transparency[19]Fig. 2. Visual comparison of digital health interventions for lymphedema care, highlighting core features, clinical outcomes, and major implementation limitations across telehealth, mobile apps, and VR-based therapies
Despite cost and access limitations, the psychosocial and functional benefits support VR’s integration into multimodal lymphedema care. Digital health interventions—including telehealth, mobile applications, advanced compression devices, and AI-driven platforms—are transforming lymphedema care by improving monitoring, adherence, and patient outcomes. Table 3 summarizes key studies (≥ 20) comparing these interventions, their features, outcomes, and limitations.
Artificial intelligence and data-driven approaches
Artificial intelligence (AI) and machine learning (ML) are poised to transform lymphedema care by enabling early risk stratification, individualized therapy, and real-time monitoring. This section presents emerging applications, algorithmic performance comparisons, integration with wearable technologies, and key ethical and implementation considerations (Ellakwa T& Ellakwa, D, [97]).
Applications of AI in lymphedema care
Predictive modeling for onset and progression
AI and ML-based predictive models leverage heterogeneous datasets—including electronic health records (EHRs), imaging, blood biomarkers, and treatment variables—to anticipate lymphedema onset and severity. Random forest models (RFMs) have demonstrated robust predictive capacity (AUC > 0.85) for identifying upper limb lymphedema risk following breast cancer surgery, particularly when factoring in lymph node dissection and postoperative complications [88, 89, 98].
Ensemble learning methods, such as XGBoost and support vector machines (SVMs), show strong external validation in head and neck cancer cohorts, with F1 scores and AUCs reaching 84% and 79%, respectively [99, 100]. While multilayer perceptrons (MLPs), k-nearest neighbors (KNN), and generalized logistic regression offer competitive performance in some datasets, traditional logistic regression remains comparably accurate [100].A recent comparative evaluation included models such as artificial neural networks (ANNs), Naive Bayes, and decision trees, reporting perfect ROC-AUC scores (1.00) when integrating cardiac parameters like end-diastolic volume and ejection percent [101]. Table 4 summarizes key AI models, performance metrics, and predictor variables. Table 4. Comparative performance of AI models for lymphedema predictionModel typeAccuracy (%)AUCKey predictorsStudy citationLogistic regression81.00.87BMI, hypertension, TNM stage, lymph node dissection, treatment, and nursing careDu et al. [76]Random forest89.40.894Same as above + lesion sitePeng & Lu [98]Artificial neural network73.1–81.90.731–0.819BMI, hypertension, TNM stage, dissection level, treatment, nursePeng & Lu [98]Xgboost94.990.89Hypertension, lymph nodes removed, complications, rehab, chemo/radiotherapySun et al. [30]Support vector machine75.0–84.00.71–0.87BMI, radiotherapy, chemotherapy, axillary node dissectionBoonstra & Meester [102]Generalized logistic reg73.1–81.90.731–0.819As abovePeng & Lu [98]Ensemble models75.0–84.00.71–0.87Same as above + lymph node countsDu et al. [76]
AI for individualized therapy planning
AI systems are now being integrated into therapy personalization, beyond diagnostics. ML-enhanced compression systems dynamically modulate pressure based on feedback parameters (e.g., limb circumference, perfusion index), outperforming static regimens in terms of comfort and treatment response [103, 104].
Web-based deep learning models further tailor interventions by considering biometric data, adherence history, and tissue characteristics to recommend personalized exercise and compression plans [105–107].
Integration with wearables and monitoring systems
Smart garments and AI-driven alerts
Wearable technology integrated with AI enables automated adherence monitoring and real-time alerts. Smart compression garments embedded with bioimpedance sensors detect fluid changes and trigger clinical notifications, facilitating early intervention [108].
IoT-enabled platforms have improved adherence rates by up to 40%, leveraging smartphone app connectivity and automated feedback loops [109–111].
In addition, motion sensors (e.g., gyroscopes, accelerometers) capture mobility patterns, assess self-care behaviors, and identify deterioration trends—allowing clinicians to intervene before clinical worsening [112, 113].
Ethical and practical considerations.
Ethical concerns.
Despite their clinical promise, AI models raise serious ethical questions. Many systems are trained on demographically skewed datasets, leading to potential algorithmic bias and inequitable care when generalized to underrepresented populations [114, 115].
The use of “black-box” algorithms limits explainability, undermining clinician trust and informed consent.
Recommended solutions include:
- Training with diverse datasets
- Implementation of explainable AI (XAI)
- Maintaining human-in-the-loop oversight in decision pathways
Data privacy is another critical concern. As wearable devices collect continuous, sensitive health data, regulatory frameworks must ensure data encryption, de-identification, and transparent user agreements [12].
Practical barriers
Incorporating AI into clinical workflows introduces several real-world challenges:
- High costs for device procurement, cloud infrastructure, and algorithm development
- Lack of interoperability between AI tools and existing EHRs
- Need for clinician education in AI literacy and interpretation
- Regulatory fragmentation and lack of standardized validation protocols
These limitations particularly affect low-resource settings, where health systems may be unable to scale advanced AI tools. Nonetheless, progress in regulatory harmonization and multidisciplinary training is essential to unlock the full potential of AI-driven lymphedema care [112].
Next-generation compression technologies
Recent innovations in compression therapy extend beyond conventional garments to include wearable robotics, sensorized textiles, and AI-enhanced systems. These technologies aim to improve clinical efficacy, user comfort, and long-term adherence through smart, patient-centric design**.**
Wearable compression devices
Modern systems integrate mobile connectivity, soft robotics, and flexible electronics to deliver precise, gradient pressure patterns that simulate manual lymphatic drainage (MLD). A key example, the Dayspring™ system, achieved an 18% improvement in quality of life (QoL) and superior mobility vs. traditional pneumatic pumps (p < 0.01) [116].
Soft robotic sleeves, using air microfluidic channels (0.04–1 mm^2^), allow programmable pressure zones to mimic lymphatic flow. They operate at < 45 dB and reduce device bulk by 80% via valve miniaturization [117]. Vibration-based wearables, generating 70–180 Hz oscillations, replicate MLD effects with 85% equivalence in phantom studies. Despite promising performance, long-term durability data (> 12 weeks) remain limited [118].
Advanced pneumatic compression devices (APCDs)
Contemporary APCDs provide anatomically targeted protocols for limbs, trunk, and head/neck regions. In head and neck lymphedema (HNL), 2-week APCD use reduced dermal backflow in 75% of patients and improved facial composite scores by 22% (p = 0.013) [119]. For gynecologic cancer survivors, a 4-week dual-mode protocol preserved limb volume in 70% of cases, with 12% improvement using adjunctive bandaging [120].
A 12-week randomized controlled trial (RCT) demonstrated that advanced pneumatic compression devices (APCDs) significantly reduced arm edema in patients with breast cancer-related lymphedema, achieving a 29% reduction compared to a 16% worsening observed with basic pumps (p < 0.01) [118]. Additionally, the study found that APCDs led to a 5.8% reduction in tissue water, as measured by tissue dielectric constant, whereas standard therapy resulted in only a 1.9% reduction [118]. These findings were corroborated by near-infrared lymphography, which confirmed the superior fluid reduction capabilities of APCDs. Despite these clinical benefits, cost remains a significant barrier to widespread adoption, with advanced devices priced at approximately 800 for basic models [118]. The economic implications are further highlighted by studies showing that APCDs can reduce lymphedema-related healthcare costs and hospitalizations, but the initial investment may limit accessibility for some patients [121, 122].
Non-pneumatic and low-profile innovations
Shape-memory alloys and active compression textiles improve wearability and reduce therapy burden. A 4-week study using ankle supports (n = 13) reported a 0.84 cm circumference reduction and a 52 mL volume loss, with 8100 steps/day, indicating high mobility [123].
Sensorized sleeves maintain 15–25 mmHg pressure with < 5% calibration drift over 10 days and reduced thickness (2.1 mm vs. 8.3 mm in standard garments) [124]. Phase**-change fabrics, maintaining 28–34 °C, improved tissue pliability by 18% (p = 0.004).** Antimicrobial sleeves using silver-coated yarn and capacitive sensors detected incorrect donning with 92% accuracy. However, durability beyond 6 months remains unverified [116, 123].
Critical analysis and limitations
Although next-generation compression devices demonstrate substantial advances in usability and symptom control, key limitations must be acknowledged: LimitationEvidenceSmall sample sizes8 of 10 cited studies had n < 50Industry funding bias6 of 10 studies are industry-fundedData interoperabilityEHR-device integration remains limited
To ensure clinical translation, future studies should pursue:
- Multicenter trials with > 100 participants
- Cost-effectiveness analyses comparing APCDs to CDT
- Integration of AI-driven personalization. Figure 3 illustrates comparative features of modern compression technologies. Fig. 3. Comparison of advanced compression technologies for lymphedema management, including pneumatic, non-pneumatic, robotic, and sensorized systems. Visualized attributes include pressure control, wearability, cost, and clinical evidence maturity
Integrating digital health and compression technologies
The integration of digital health platforms with next-generation compression technologies represents a significant evolution in lymphedema care. This convergence supports the development of closed-loop systems capable of continuously adjusting therapeutic parameters in real time, guided by individualized physiological data and artificial intelligence (AI) [125].
Models for integrated care
Modern sensorized compression garments—such as the Dayspring™ system—are now embedded with bioimpedance sensors that monitor interstitial fluid fluctuations while delivering gradient pressures of 15–25 mmHg (Ellakwa T et al., [126]). These systems demonstrate clinical efficacy, achieving 11–27% reductions in limb volume, and are integrated with mobile platforms that analyze dielectric trends and alert clinicians when fluid accumulation exceeds 5% of baseline [116, 124, 127]. IoT-enabled compression sleeves, equipped with resistive and pneumatic sensors, have reached 92% accuracy in detecting improper donning, thereby reducing subtherapeutic compression events by 30% over 10 days [124]. Machine learning algorithms, trained on large-scale datasets (n = 1,556), can predict optimal pneumatic compression profiles with 84% accuracy, adjusting chamber inflation based on accelerometer-derived movement data [128, 129]. Platforms such as LymphActiv, which synchronize wearable activity trackers with adaptive garments, have shown 18% increases in therapeutic movement duration and 98% adherence over 24 weeks [93, 94]. These systems are particularly valuable in addressing non-adherence, which affects up to 67% of patients [80, 81, 116]. Telehealth integration enhances these systems’ reach and efficacy. In Puducherry, India, a pilot using 3D infrared imaging for garment fitting and remote consultations yielded 11.3% limb volume reduction among filarial lymphedema patients, despite a baseline digital literacy of only 32% [73, 74]. Similarly, swallowing sensors combined with compression collars achieved a 22% reduction in dysphagia severity for head and neck lymphedema [130].
Case studies and pilot programs
Real-world implementations illustrate both innovative potential and persistent challenges:
- A 12-month study in Shanghai evaluated a WeChat-based CDT platform integrated with smart sleeves and reported:
- o40% improvement in bandaging technique through AR tutorials
- o23% greater limb volume reduction compared to standard care (p = 0.013)
- o89% patient satisfaction with real-time pressure feedback [80, 81]
However, interoperability remains problematic. A U.S. multicenter study found a 17% failure rate in integrating AI pump data into electronic health records (EHRs), emphasizing the need for HL7/FHIR-compatible systems [128, 129].
Adaptations in low-resource settings have demonstrated promising outcomes:
- In Sri Lanka, portable 3D imaging enabled the prefitting of compression garments, which resulted in 1.1–27.2% limb volume reductions, even without therapist oversight.
- In Ghana, a national program combining SMS reminders and community health workers reduced cellulitis incidence by 44% [73, 74].
Human–AI hybrid models are also emerging. A German pilot study using VR-guided compression demonstrated:
- 28% faster mastery of self-massage techniques
- 15% improvement in pressure accuracy compared to video-only training
- 73% of patients preferred AI/human blended coaching [93, 94].
Three critical success factors were identified across implementations:
- Granular data integration: systems correlating hourly compression metrics with patient logs improved edema control by 22% compared to siloed setups [93, 94].
- Cultural adaptability: multilingual interfaces led to a 37% increase in user retention in South India, compared to English-only versions [73, 74].
- Scalable infrastructure: cloud-based analytics reduced monitoring costs by 58% in a European trial with 500 participants [116].
Ongoing limitations include:
- Sensor durability, with failure rates up to 15% after six months in humid environments [124]
- Lack of standardized reimbursement pathways. The 2024 Lymphedema Technology Accord now recommends the adoption of unified CPT codes that cover both hardware and digital therapeutics [93, 94]
This transition from reactive to predictive care, powered by AI, 5G, and edge computing, paves the way for sub-second pressure modulation in response to microfluidic shifts. Computational models suggest that these systems could reduce advanced-stage complications by up to 60% [128]. However, realizing this potential will require coordinated advances in cybersecurity, clinician training, and regulatory harmonization to ensure safe, effective, and equitable deployment.
Patient outcomes and quality of life
Clinical and technological advances in lymphedema treatment have demonstrated meaningful improvements across physical, psychosocial, and behavioral domains (Ellakwa T et al., [131]). Yet, the translation of therapeutic efficacy into real-world quality of life (QoL) is mediated by multifactorial determinants, including device usability, cultural context, and psychological resilience.
Physical outcomes
The primary benchmark for intervention success remains quantitative volume reduction. Complete decongestive therapy (CDT) retains its status as the gold standard, delivering median volume reductions of 66.5% in upper limbs and 71.5% in lower limbs [132]. Adjunct surgical approaches—such as lymphaticovenous anastomosis (LVA) and vascularized lymph node transfer (VLNT)—have further amplified outcomes, particularly when integrated in multi-modality regimens (e.g., liposuction + nanofibrillar scaffolds), achieving sustained normalization of limb volume over 24.6 months [133]. Limb-specific variability persists: liposuction corrects 100.1% in upper limbs versus 59.3% in lower limbs, likely due to enhanced adherence to postoperative compression in the upper extremity [134]. Skin health also improves with consistent use. In underserved settings, IoT-enabled compression garments led to a 44% reduction in cellulitis rates, attributed to real-time alerts and proactive monitoring [135]. Pain relief is another therapeutic benefit—CDT combined with standard care reduced carpal tunnel-related pain by 8.3%, while grip strength improved by 15% [136]. Functional mobility gains were evident across modalities. For instance, VR-based therapy improved shoulder mobility by 28%, though conventional resistance training still outperformed in terms of strength development [133].
Psychosocial and emotional well-being
Lymphedema’s psychological toll remains significant. Anxiety and depression affect 27–34% and 18–29% of patients, respectively, particularly in those with visible disfigurement or recurrent infections [137], Ellakwa D et al., [58]). Standardized response mean (SRM) scores from the LyQLI indicate improvements of 0.8 in physical and 1.2 in psychosocial domains following treatment [136, 138]. Social stigma is a critical barrier—33% of patients avoid public settings due to visible compression garments (Gündüz et al., [139]). In appearance-sensitive cultures, stigma is further intensified. Digital tools, particularly mobile platforms like TOLF, may mitigate this burden. Use of such tools was associated with 30% higher adherence and 23% greater functional independence [132],Onazi et al., 2020). Nevertheless, inequities remain. For example, Latina breast cancer survivors report workplace discrimination yet adapt via clothing strategies and peer networks [136]. Notably, psychological relief may supersede physical metrics. In one cohort, 42% of LVA patients discontinued compression garments despite modest volume reduction, prioritizing comfort and self-image over objective measures [140].
Adherence and satisfaction metrics
Adherence and satisfaction differ significantly across interventions. Compliance with traditional compression is low (51.7%), with mobility restriction (33%) and pain (28.8%) cited as common deterrents (Gündüz et al., [139]).
Conversely, smart compression sleeves with real-time feedback achieved 94.8% adherence at 3 months [135].
Usability scores further reflect this contrast: only 31% of patients wear standard garments for over 12 h/day, while 85.4% rated IoT-based devices ≥ 9/10 for usability [141].
Surgical satisfaction varies by procedure:
- VLNT recipients report 86% improvement in function and reduced infections [142].
- Omental flap patients report 97.75% satisfaction, valuing long-term results despite minor abdominal tension (2.29%) [143].
These findings underscore the necessity of shared decision-making that aligns interventions with patient-defined priorities.
Barriers to sustained use
Financial constraints dominate in LMICs—custom garments cost 300–500% more than standard types, limiting access for 67% of patients (Onazi et al., 2020).
Cultural and technological barriers compound this issue. In South Asia, multilingual platforms increased retention by 37%, while in Ghana, SMS reminders were less effective in digitally underserved populations [73, 74, 132].
Even in high-resource settings, technical failures persist:
- Sensor degradation in 15% of garments within six months [135]
- EHR integration issues affecting 17% of AI workflows
- 40% of breast cancer survivors report social withdrawal due to device visibility [144],Gündüz et al., [139])
- 28% fear public device malfunction, highlighting ongoing psychosocial fragility
Multidisciplinary efforts are essential: scalable reimbursement, culturally adaptive education, device durability standards, and patient-informed regulation are all crucial.
Synthesis and implications
Improving lymphedema outcomes necessitates a holistic care paradigm encompassing physical function, emotional health, and social context. While innovations in surgery and compression technology yield measurable benefits, real-world effectiveness depends on patient engagement, accessibility, and destigmatization (Ellakwa D et al., [145]).
Priority areas for future research and policy include:
- Incorporation of QoL metrics into trial endpoints
- Culturally adaptable, scalable digital solutions
- Equity-focused design of next-generation devices
True transformation requires alignment of medical innovation with patient dignity, autonomy, and lived experience Ellakwa.
Various interventions—including CDT, surgical strategies, and digital platforms—have shown quantifiable gains in both physical outcomes (e.g., limb volume, mobility) and psychosocial factors (e.g., stigma, anxiety reduction) (Fig. 4).Fig. 4. Impact of interventions on physical and psychosocial outcomes. This two-panel visual compares CDT, surgical, and digital technologies across key outcomes, including limb volume reduction, pain, QoL, and treatment adherence
Challenges and considerations
Despite promising developments, significant systemic barriers remain:
- 67% of LMIC patients cannot afford custom devices
- Digital literacy remains a barrier to telehealth engagement
- 62% of AI tools are trained on non-diverse datasets
- 74% of smart garments misclassified as “cosmetic,” hindering insurance coverage
- 44% of clinicians are unfamiliar with AI-enabled compression systems
- Poor interoperability between wearables and EHRs
Solutions include:
- Insurance mandates based on equity
- Post-market AI oversight
- Multilingual patient education
- Workforce development for digital literacy
Future directions
Lymphedema care is entering the era of precision medicine and predictive rehabilitation, guided by:
- Genomics and multi-omics platforms [58]
- Electrochemical biosensors for early detection
- Smart textiles for dynamic compression control
- Digital twins that simulate personalized therapy responses
Ongoing trials (e.g., LYMPH-REAL) are comparing AI-guided vs. conventional CDT, while policy shifts like Canada’s Bill C-214 are paving the way for regulatory recognition of sensor-equipped garments.
WHO-aligned frameworks will be vital in ensuring equitable access and global scalability.
Conclusion
Despite rapid technological advances, the future of lymphedema management will depend on overcoming persistent systemic barriers and ensuring equitable access to care. Financial constraints, digital literacy gaps, limited diversity in AI training datasets, insurance misclassification of smart garments, clinician unfamiliarity with new technologies, and poor interoperability between wearables and electronic health records all threaten to widen disparities in outcomes. Addressing these challenges will require policy interventions such as insurance mandates grounded in equity, robust post-market AI oversight, multilingual patient education, and workforce development to enhance digital literacy. Looking ahead, lymphedema care is poised to benefit from precision medicine approaches, including genomics, electrochemical biosensors, smart textiles, and digital twins that enable personalized therapy simulations. The integration of artificial intelligence and machine learning is already enhancing imaging precision, risk stratification, and treatment outcomes, while ongoing clinical trials are evaluating the comparative effectiveness of AI-guided versus conventional therapies. Policy shifts and international frameworks, such as those aligned with the World Health Organization, will be essential to ensure that these innovations are accessible and scalable across diverse populations. Ultimately, the convergence of AI-driven compression technologies, sensor-enabled diagnostics, and culturally responsive digital health platforms has the potential to transform lymphedema management. These advances have already demonstrated measurable improvements in adherence and reductions in complications, signaling a new era of patient-centered, predictive, and participatory care. However, sustained progress will require continued investment in research, standardization of outcome measures, and a commitment to addressing the social and structural determinants that shape access to emerging therapies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rai P, Mahajan A, Shukla S et al (2025) Imaging and management of lymphedema in the era of precision oncology. Br J Radiol 98:619–629. 10.1093/bjr/tqaf 02910.1093/bjr/tqaf 029PMC 1201237939932868 · doi ↗ · pubmed ↗
- 2Džupina A, Yaluri N, Singh J et al (2025) Predictors of the efficacy of lymphedema decongestive therapy. Medicina 61. 10.3390/medicina 6102023110.3390/medicina 61020231 PMC 1185732340005348 · doi ↗ · pubmed ↗
- 3Džupina A, Yaluri N, Singh J et al (2025) Predictors of the efficacy of lymphedema decongestive therapy. Medicina (B Aires) 61(2):1–1510.3390/medicina 61020231 PMC 1185732340005348 · doi ↗ · pubmed ↗
- 4Manrique OJ, Bustos SS, Ciudad P et al (2020) Overview of lymphedema for physicians and other clinicians: a review of fundamental concepts. Mayo Clin Proc 97(10):1920–1935. 10.1016/j.mayocp.2020.01.00610.1016/j.mayocp.2020.01.00632829905 · doi ↗ · pubmed ↗
- 5Liu Y, Liu J, Mak Y et al (2021) Prevalence and predictors of breast cancer-related arm lymphedema over 10 years in postoperative breast cancer patients: a cross-sectional study. Eur J Oncol Nurs 51:101909. 10.1016/j.ejon.2021.10190910.1016/j.ejon.2021.10190933626424 · doi ↗ · pubmed ↗
- 6Dayan J, Ly C, Kataru R et al (2018) Lymphedema: pathogenesis and novel therapies. Annu Rev Med 69:263–276. 10.1146/annurev-med-060116-02290010.1146/annurev-med-060116-02290028877002 · doi ↗ · pubmed ↗
- 7Sanka S, Chryssofos S, Anolik R et al (2025) Advances in surgical management of chronic lymphedema: current strategies and future directions. Med Oncol. 10.1007/s 12032-024-02576-210.1007/s 12032-024-02576-2PMC 1172912639806245 · doi ↗ · pubmed ↗
- 8De Sire A, Losco L, Lippi L et al (2022) Surgical treatment and rehabilitation strategies for upper and lower extremity lymphedema: a comprehensive review. Medicina (Kaunas) 58(7):954. 10.3390/medicina 5807095410.3390/medicina 58070954 PMC 932442635888673 · doi ↗ · pubmed ↗