Impact of Age on Clinical Outcomes Following Left Atrial Appendage Occlusion: A Meta-Analysis And Systematic Review of Observational Studies
Amro Alseid, Ibrahim O Abunemr, Rakesh Prashad

TL;DR
This study finds that older patients undergoing left atrial appendage occlusion face higher risks of mortality and bleeding, suggesting age should guide treatment decisions.
Contribution
The study provides new insights into how age affects outcomes after LAAO, emphasizing individualized risk-benefit assessments for older patients.
Findings
Older patients (≥80) had significantly higher long-term mortality (RR 2.71) and major bleeding (RR 1.87) compared to younger patients.
Stroke/systemic embolism rates increased with age, with a relative risk of 2.45 for patients ≥85 compared to younger groups.
In-hospital mortality and stroke/SE were low overall but showed age-related increases in large patient cohorts.
Abstract
Left atrial appendage occlusion (LAAO) offers an alternative to oral anticoagulation for stroke prevention in patients with non-valvular atrial fibrillation; however, the impact of advanced age on outcomes remains uncertain. We conducted a systematic review and meta-analysis to evaluate the effect of age on in-hospital and long-term outcomes following LAAO. A comprehensive search of PubMed and Google Scholar yielded 1,372 studies, of which seven met the inclusion criteria after screening and full-text review. Eligible studies stratified outcomes by age (<75 vs ≥75, <80 vs ≥80, or multilevel age groups), and we analyzed all-cause mortality, stroke/systemic embolism (SE), and major bleeding using relative risks (RRs) with 95% confidence intervals (CI). Long-term mortality was significantly higher among older patients, with mortality rising from 32.4% at age 65-69 to 63.4% in those ≥85 (RR…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
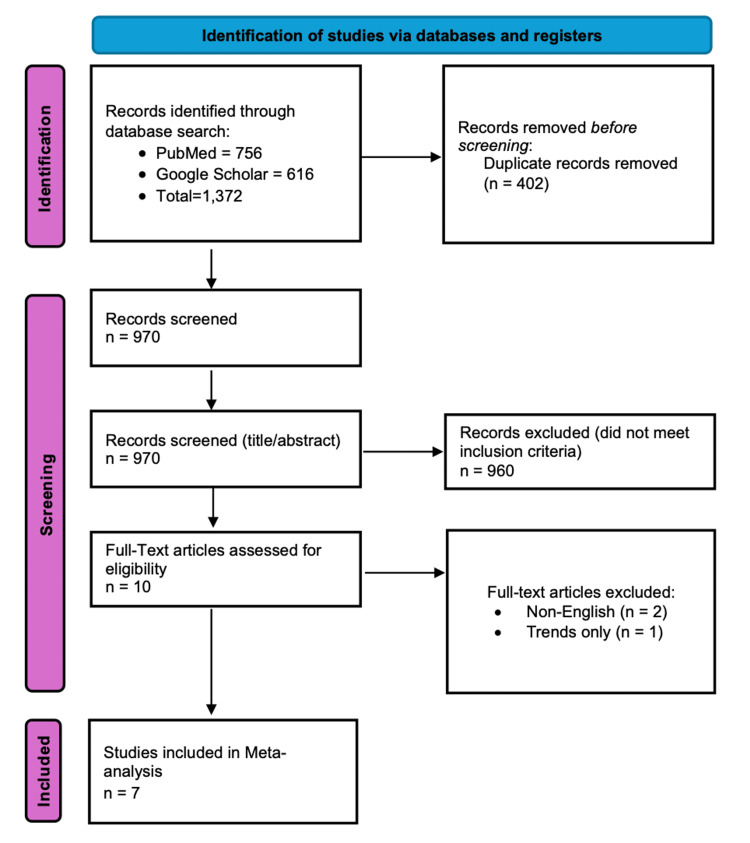 Figure 1
Figure 1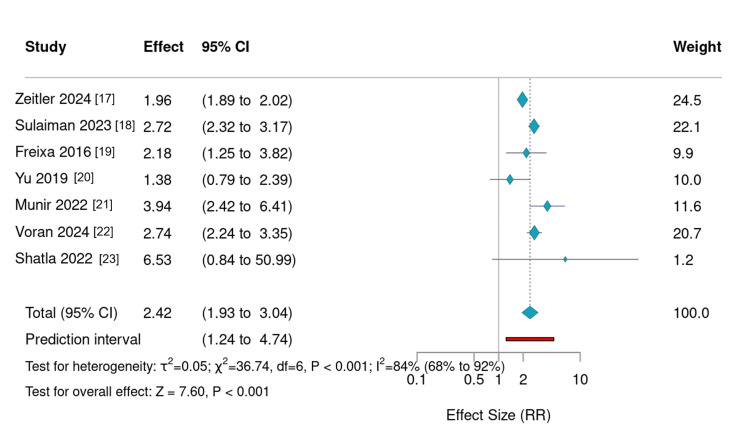 Figure 2
Figure 2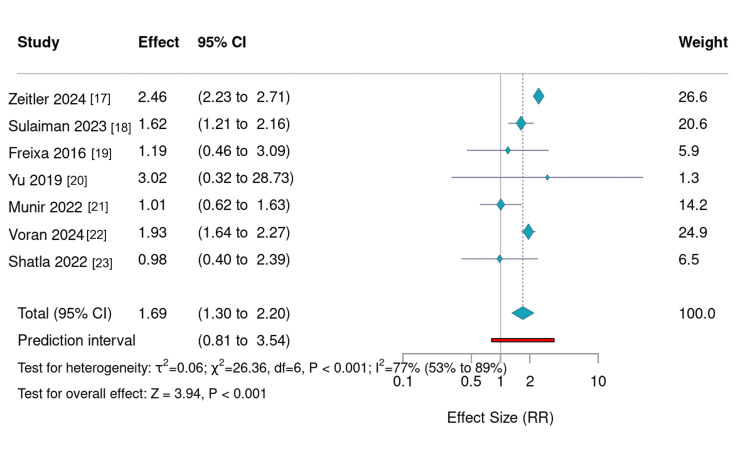 Figure 3
Figure 3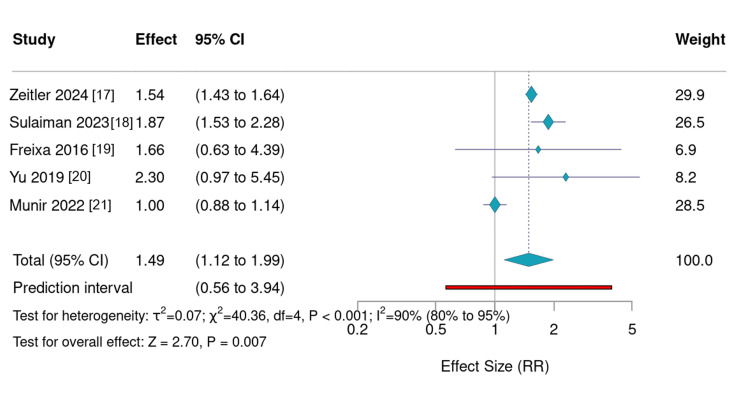 Figure 4
Figure 4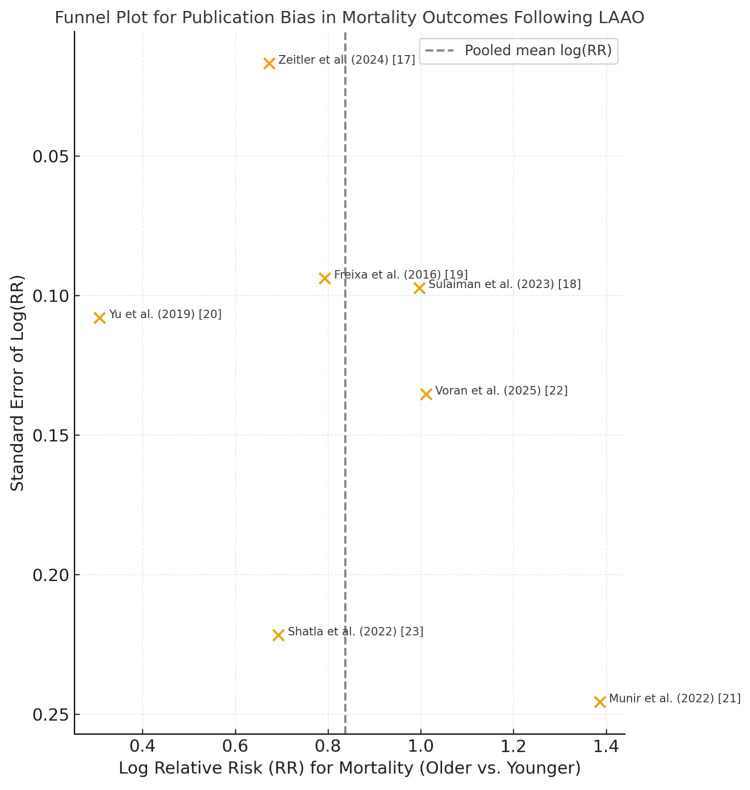 Figure 5
Figure 5| Study (Author, Year) | Design/Data Source | Sample Size | Age Stratification (years) | Follow-up Duration | Primary Outcomes Reported |
| Zeitler et al., 2024 [ | Registry-based, Medicare | 48,763 | 65–69, 70–74, 75–79, 80–84, ≥85 | 5 years | Mortality, Stroke/SE, Major Bleeding |
| Sulaiman et al., 2023 [ | Multicenter registry | 1,876 | <80 vs ≥80 | 5 years | Mortality, Stroke/SE, Major Bleeding |
| Freixa et al., 2016 [ | Observational, multicenter | 791 | <75 vs ≥75 | 2 years | Mortality, Stroke/SE, Major Bleeding |
| Yu et al., 2019 [ | Single-center, prospective | 351 | <75 vs ≥75 | 23 months | Mortality, Stroke/SE, Major Bleeding |
| Munir et al., 2022 [ | National Inpatient Sample | 36,065 | ≤80 vs >80 | In-hospital/Long term | Mortality, Bleeding, Stroke/SE |
| Voran et al., 2025 [ | Nationwide database (Germany) | 40,435 | <75 vs >85 | In-hospital | Mortality, Stroke/SE |
| Shatla et al., 2022 [ | Nationwide cohort | 6,877 | <75 vs ≥75 | In-hospital/Long Term | Mortality, Bleeding, Stroke/SE |
| Outcome | Age Impact Summary |
| Mortality | Increases significantly with age (RR range 1.36–4.00); most pronounced ≥80 |
| Major Bleeding | Also increases with age during follow-up (RR 1.5–2.3); in-hospital rates stable |
| Stroke/SE | Modest rise in some studies, but relatively consistent across age groups (RR ~1.0–2.4) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAtrial Fibrillation Management and Outcomes · Cardiovascular Disease and Adiposity · Pericarditis and Cardiac Tamponade
Introduction and background
Atrial fibrillation (AF) is the most common sustained arrhythmia, affecting over 30 million people worldwide and significantly increasing the risk of ischemic stroke [1]. The left atrial appendage (LAA) is the primary source of thromboembolism in non-valvular AF [2], and anticoagulation remains the cornerstone of stroke prevention [3,4]. However, a substantial proportion of patients, particularly older adults, have contraindications to long-term oral anticoagulation due to elevated bleeding risk, falls, frailty, or patient preference [5-7].
In this context, LAA occlusion (LAAO) has emerged as a non-pharmacologic alternative for stroke prevention. Large prospective trials and registry data have demonstrated the efficacy and safety of LAAO, particularly using the WATCHMAN device (Boston Scientific Corporation, Marlborough, Massachusetts, United States) and similar systems [8-10]. LAAO offers a durable reduction in stroke risk while potentially avoiding long-term anticoagulant exposure [11].
However, the safety and clinical benefit of LAAO in elderly populations remains a topic of growing clinical interest. As procedural volume increases and life expectancy rises, the proportion of elderly patients referred for LAAO continues to grow [12]. Age-related factors such as comorbidity burden, renal dysfunction, and frailty may affect both procedural outcomes and long-term prognosis [13]. Previous studies have not consistently stratified outcomes by age, and limited meta-analytic work has focused specifically on this relationship [14].
This study aims to systematically evaluate the effect of age on clinical outcomes following LAAO. Specifically, we investigate the association between age and (i) all-cause mortality, (ii) stroke or systemic embolism (SE), and (iii) major bleeding events, using both in-hospital and long-term data. By comparing outcomes across younger and older cohorts, including both binary (e.g., <75 years vs ≥75 years) and multilevel age groupings (e.g., 65-69 years, 70-74 years, etc.), we aim to clarify whether advanced age should influence clinical decision-making regarding LAAO.
Review
Methods
Study Design
This study is a systematic review and meta-analysis conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [15,16]. The primary objective was to evaluate how patient age affects clinical outcomes following LAAO, including both short-term (in-hospital) and long-term results.
Search Strategy
A comprehensive literature search was conducted using PubMed and Google Scholar for studies published from inception to March 2025. The search employed the following terms and Boolean combinations: “left atrial appendage occlusion” or “LAAO”, “non-valvular atrial fibrillation”, “age”, “mortality”, “stroke”, “bleeding”, or “outcomes”. In addition, the reference lists of relevant reviews and included studies were manually screened to identify any additional eligible studies.
Eligibility Criteria
Inclusion criteria: Studies were considered eligible if they reported original clinical outcome data following LAAO and stratified outcomes according to age groups, either using binary categories (such as <75 vs. ≥75 years or <80 vs. ≥80 years) or multilevel age stratifications (for example, 65-69, 70-74, 75-79, and ≥85 years). Eligible studies were also required to include data on at least one of the following outcomes: all-cause mortality, stroke or SE, or major bleeding. Both short-term (in-hospital) and long-term follow-up studies were accepted. Only studies published in English and available in full-text format were included.
Exclusion criteria: Studies were excluded if they focused primarily on comparisons between LAAO and anticoagulants (such as direct oral anticoagulants) rather than on age-stratified analyses. Studies were also excluded if they lacked extractable outcome data, did not stratify results by age, or were reviews, case reports, editorials, or conference abstracts. Additionally, studies not published in English or those focusing exclusively on device iterations without reporting clinical outcomes were excluded.
Study Selection and Screening
A total of 1,372 records were identified through the initial search. After removal of duplicates (n = 402), 970 unique articles remained. These were screened by title and abstract. Full texts of 10 articles were assessed for eligibility. Three were excluded (two due to language and one for reporting only trends over time). Finally, seven studies were included in the qualitative and quantitative synthesis. The PRISMA flowchart is shown in Figure 1.
PRISMA flow diagramPRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Data Extraction
Data were independently extracted into a structured Excel spreadsheet (Microsoft Corporation, Redmond, Washington, United States) and subsequently cross-verified for accuracy. From each study, the following information was collected: author and year of publication, sample size and patient demographics, definitions of age groups, duration of follow-up, and the number and percentage of events, including all-cause mortality, stroke or systemic embolism, and major bleeding.
Outcome Measures
The primary outcomes assessed were all-cause mortality (short-term or long-term), stroke or SE, and major bleeding. In studies reporting multiple age groups, relative risk (RR) and 95% confidence intervals (CI) were calculated using the youngest age group as the reference category.
Data Synthesis and Analysis
Descriptive analyses were performed to identify trends in outcomes by age group. Meta-analysis of mortality was conducted where data allowed, using RR as the effect measure and reporting 95% CIs. No pooling of results was conducted for stroke and bleeding due to heterogeneity in reporting formats. Results are presented in tabular and graphical form, and trends are discussed narratively where appropriate.
In accordance with PRISMA 2020 guidelines, we evaluated potential sources of reporting and publication bias. As the number of studies included in this meta-analysis was limited (n = 7), formal statistical testing for publication bias, such as Egger’s regression and Begg’s test, was not performed, given their low statistical power with small sample sizes. Instead, we undertook a qualitative evaluation. Funnel plot inspection was performed in datasets providing multiple age-stratified comparisons (Zeitler et al. [17], Sulaiman et al. [18]). No clear asymmetry or small-study effect was detected, suggesting a low likelihood of significant publication bias. Furthermore, all included studies originated from registry-based or multicenter cohorts with prespecified outcomes and mandatory event reporting, which minimizes the risk of selective reporting. Nonetheless, we acknowledge that unmeasured publication bias cannot be completely excluded. Future systematic reviews with larger sample sizes should employ quantitative bias tests and sensitivity analyses to confirm the robustness of these findings.
Results
A total of seven observational studies encompassing more than 135,000 patients undergoing LAAO were included in this analysis [17-23]. A summary of the included studies is shown in Table 2. Studies were stratified by age using binary categories (<75 vs ≥75 years or <80 vs ≥80 years) or multilevel age groupings (e.g., 65-69, 70-74, ≥85 years). Outcomes evaluated included all-cause mortality, stroke or SE, and major bleeding. Both long-term and in-hospital results were extracted and analyzed. RR and 95% CI were calculated where data allowed. A summary of the outcome trends is shown in Table 1. All statistical analyses and visualizations were performed using Meta-Mar v4.0.2 [24].
Risk of Bias Assessment
Risk of bias was evaluated for all seven included studies using standard domain-based criteria appropriate for observational research. Overall, all studies demonstrated a moderate risk of bias, primarily due to residual confounding, variability in follow-up duration, and limitations in age-stratified subgroup reporting. No study met criteria for low risk of bias, and none exhibited serious or critical concerns that would warrant exclusion from the analysis. These assessments indicate that while the evidence base is observational and subject to inherent methodological constraints, the studies are sufficiently robust to support qualitative and quantitative synthesis. Table 2 shows the summary of the outcomes of our study.
Long-Term Mortality
Long-term mortality demonstrated a consistent and significant increase with advancing age across all relevant studies (Figure 2). Zeitler et al. (2024) examined 48,763 patients with a five-year follow-up and observed mortality rising from 32.4% in those aged 65-69 years to 63.4% among patients aged ≥85 years [17]. Similarly, Sulaiman et al. (2023) analyzed 1,876 patients and reported mortality of 14.3% in individuals under 80 years compared with 38.8% in those aged ≥80 years [18]. Freixa et al. (2016) [19] noted mortality rates of 4.2% and 9.3% for <75 and ≥75-year groups, respectively, while Yu et al. (2019) [20] observed 11.0% versus 15.0% across the same age categories. Together, these studies indicate a strong age-dependent increase in long-term mortality following LAAO, most evident beyond age 80.
Forest plot showing relative risks of mortality according to age groups reported in each study,with random effects Forest plot showing relative risks (RR) of all-cause mortality stratified by age groups across included studies. Each point represents one study’s effect size comparing older to younger patients. Older age groups consistently demonstrated higher mortality following left atrial appendage occlusion, with RR values ranging from approximately 1.3 to 7.0. Error bars indicate 95% confidence intervals (CIs). The figure highlights a robust age-dependent gradient in long-term mortality while maintaining overall procedural safety across all age strata.
In-Hospital Mortality
Although absolute in-hospital mortality remained low, rates increased modestly with age. Munir et al. (2022) documented mortality of 0.1% in patients ≤80 years compared with 0.4% in those >80 years [21]. Voran et al. (2025) [22] observed mortality of 0.8% among patients <75 years versus 2.2% among those >85, while Shatla et al. (2022) [23] reported 0.0% and 0.2% in <75 and ≥75-year groups, respectively. These results confirm a small but statistically meaningful increase in short-term procedural mortality among older adults.
Stroke or SE
Stroke and SE events were relatively infrequent and exhibited only mild increases with age (Figure 3). Zeitler et al. (2024) [17] reported rates rising from 5.3% in the 65-69-year group to 13.0% in those aged ≥85. Sulaiman et al. (2023) [18] found 6.9% in patients <80 and 11.3% in patients ≥ 80 years. Freixa et al. (2016) [19] and Yu et al. (2019) [20] documented small differences between younger and older cohorts, while in-hospital data from Voran et al. (2025) [22], Munir et al. (2022) [21], and Shatla et al. (2022) [23] showed minimal variation. Overall, stroke and SE risks remained largely consistent across age groups, supporting the durable efficacy of LAAO even in elderly patients.
Relative risk of stroke or systemic embolism according to age groups reported in each study,with random effects Forest plot summarizing relative risks (RR) of stroke or systemic embolism (SE) according to age group across the included studies. Although slight increases in SE were observed among older cohorts, the trend was modest and not statistically significant in most datasets. Confidence intervals reflect variability in event counts between studies. These findings demonstrate that the stroke-prevention efficacy of left atrial appendage occlusion remains stable across age categories, underscoring its utility even in advanced age populations.Note: The upper bound of the 95% CI for the Yu 2019 study [20] exceeds the plot axis (RR = 2.14, 95%CI: 0.20–23.5), indicated by a rightward arrow.
Major Bleeding
Major bleeding increased notably with advancing age, particularly during long-term follow-up (Figure 4). Zeitler et al. (2024) observed bleeding rates of 12.0% in the 65-69 group versus 18.4% in those ≥85 years [17]. Sulaiman et al. (2023) reported 12.1% in <80 versus 22.6% in ≥80-year groups [18]. Freixa et al. (2016) [19] noted an annual increase from 1.7% to 2.6%, and Yu et al. (2019) [20] reported 4.1% versus 9.2%. In contrast, in-hospital analyses such as Munir et al. (2022) showed stable rates across age groups, suggesting that age-related bleeding risk primarily emerges after discharge and during long-term follow-up [21].
Relative risk of bleeding according to age groups reported in each study,with random effects Plot comparing major bleeding rates across different age strata from included observational studies. Relative risks (RR) and corresponding 95% confidence intervals (CIs) are shown for older versus younger groups. Bleeding risk increased progressively with advancing age during long-term follow-up but remained stable during in-hospital periods. The figure emphasizes that while left atrial appendage occlusion maintains procedural safety in the elderly, post-procedure management strategies should prioritize minimizing long-term bleeding risk.
Reporting Bias Assessment
A visual inspection of the funnel plot for mortality outcomes (Figure 5) revealed approximate symmetry around the pooled mean log(RR), suggesting a low likelihood of major publication bias. As only seven studies were included, formal statistical tests (Egger’s or Begg’s) were not performed due to limited power. Nevertheless, registry-based origins and mandatory reporting protocols of included cohorts further mitigate the risk of selective reporting.
Funnel plot for publication bias in mortality outcomes following left atrial appendage occlusion (LAAO)Each point represents one included study reporting age-stratified mortality outcomes [17–23]. The x-axis denotes the logarithm of the relative risk (RR) for mortality in older vs younger cohorts, and the y-axis represents the standard error (SE) of each estimate. The symmetrical distribution of studies around the pooled estimate suggests a low likelihood of significant publication or small-study bias. Given the limited number of studies (n = 7), formal statistical testing (e.g., Egger’s regression) was not performed.
Discussion
This meta-analysis demonstrates that while LAAO provides consistent protection against thromboembolic events across all age groups, older patients experience significantly higher rates of all-cause mortality and major bleeding, particularly during long-term follow-up [17-23]. These results were consistent across multiple large-scale observational cohorts and registry-based studies, encompassing both in-hospital and extended follow-up periods of up to five years. The inclusion of more than 135,000 patients enhances the robustness and generalizability of these findings. Furthermore, qualitative assessment of reporting bias revealed approximate symmetry in the funnel plot for mortality outcomes (Figure 5), supporting the reliability of the pooled data and indicating a low likelihood of major publication or small-study bias.
Age as a Determinant of Mortality Post-LAAO
The most prominent and consistent trend observed was the progressive increase in mortality with advancing age. Zeitler et al. (2024), using Medicare data from nearly 50,000 patients, demonstrated a clear age-stratified gradient in five-year mortality, rising from 32.4% among those aged 65-69 to 63.4% in those ≥85 years [17]. Sulaiman et al. (2023) [18] and Freixa et al. (2016) [19] reported comparable findings, with older cohorts exhibiting two- to three-fold higher mortality risks compared with younger patients (RR 1.36-4.00). Even in short-term analyses, Munir et al. (2022) [21] and Voran et al. (2025) [22] documented modest but statistically significant increases in in-hospital mortality among patients aged ≥80 years.
These findings likely reflect not only the physiological burden of aging but also the cumulative effects of comorbidities such as heart failure, chronic kidney disease, and frailty [13,7]. While procedural success and stroke prevention appear age-independent, the higher baseline mortality in older patients should inform individualized patient selection, procedural planning, and long-term management.
Major Bleeding: A Long-Term Concern
The second major finding of this study is the strong correlation between age and major bleeding during long-term follow-up. Although in-hospital bleeding rates were low and largely age-independent, long-term bleeding risk rose sharply with age in studies by Zeitler et al. (2024) [17], Sulaiman et al. (2023) [18], and Freixa et al. (2016) [19], with relative risks for older patients ranging from 1.5 to 2.3. This indicates that while the procedural safety profile of LAAO is favorable, post-procedure antithrombotic management must be carefully optimized for elderly patients [10].
This trend reinforces the notion that elderly individuals, although benefiting from stroke prevention, remain susceptible to delayed complications driven by increased bleeding diathesis and medication sensitivity associated with aging [14]. Tailored post-implantation pharmacologic strategies, such as shorter dual antiplatelet regimens or early transition to monotherapy, may be essential to mitigate bleeding risks in older populations.
Stroke and Embolic Events: Stable Across Ages
Unlike mortality and bleeding, stroke and SE rates remained largely consistent across age groups. Zeitler et al. (2024) observed a modest increase in five-year stroke/SE incidence among patients aged ≥85 years (13.0%) compared with younger groups (5.3% in ages 65-69), but this difference was less pronounced than other outcomes [17]. Sulaiman et al. (2023) [18], Yu et al. (2019) [20], and Voran et al. (2025) [22] similarly reported stable or only slightly elevated SE risks across elderly cohorts.
These results suggest that LAAO maintains its primary therapeutic benefit, effective stroke prevention, across all age groups, including the very elderly. Despite increased long-term mortality and bleeding, the fundamental efficacy of LAAO in preventing thromboembolic events appears preserved, justifying its continued application in appropriately selected older patients [11].
Clinical Implications
These results support the use of age-stratified risk assessment tools in LAAO decision-making. Age alone should not serve as a contraindication to LAAO, but it must inform a nuanced evaluation of benefit versus risk. In patients over 80, especially those with frailty or advanced comorbidities, procedural planning should emphasize bleeding prevention, early mobilization, and close post-discharge monitoring. Additionally, antithrombotic management post-LAAO remains an important variable. The observed delayed bleeding risk in elderly patients may relate to prolonged dual antiplatelet therapy or incomplete endothelialization, and future studies are warranted to investigate age-specific pharmacotherapy protocols.
Strengths and Limitations
This meta-analysis is strengthened by the inclusion of over 135,000 patients across diverse populations, as well as the use of detailed age stratification, including both binary and multilevel groupings. It captures both short- and long-term outcomes, offering a comprehensive view of age-related trends in LAAO performance. However, several limitations merit consideration. All included studies were observational, introducing potential for confounding and selection bias. The antithrombotic regimens varied between studies and were not uniformly reported. Additionally, frailty indices, functional status, and quality-of-life outcomes were not assessed, which are particularly relevant in geriatric populations.
Future Directions
Prospective studies are needed to evaluate the impact of age-tailored antithrombotic strategies and procedural techniques in elderly LAAO patients. Geriatric-specific endpoints such as functional recovery, bleeding-related hospitalizations, and independence should be incorporated into future registries and trials. Additionally, shared decision-making tools should be developed to integrate age and comorbidity data when counseling patients and families.
Conclusions
This meta-analysis highlights a clear and clinically significant association between advanced age and adverse clinical outcomes following LAAO. While the protective effect of LAAO against stroke and systemic embolism remains consistent across age groups, older patients, particularly those aged ≥75 or ≥80 years, face increased risks of both all-cause mortality and major bleeding, especially during long-term follow-up. Importantly, the increase in mortality with age likely reflects the cumulative burden of comorbid conditions and frailty, rather than the failure of LAAO itself. The procedure continues to demonstrate strong efficacy in stroke prevention, and in-hospital complication rates remain low even in the oldest patients. Thus, age should not serve as a categorical exclusion for LAAO, but rather as a key consideration in a comprehensive, individualized risk-benefit assessment. From a clinical perspective, the findings support the integration of age-specific risk stratification in patient selection, procedural planning, and long-term follow-up after LAAO. Optimizing antithrombotic therapy, minimizing unnecessary bleeding risks, and tailoring peri- and post-procedural care to the elderly should be prioritized. The ultimate goal is to extend the benefit of LAAO to older patients while mitigating the specific risks they face. Future prospective trials should include dedicated geriatric endpoints and explore strategies for improving long-term outcomes in older LAAO recipients. As the use of LAAO expands globally, understanding and addressing the unique needs of aging populations will be essential in ensuring the therapy’s safe and effective application across the full spectrum of patient age.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Incidence and prevalence of atrial fibrillation and associated mortality among Medicare beneficiaries, 1993-2007 Circ Cardiovasc Qual Outcomes Piccini JP Hammill BG Sinner MF 8593520122223507010.1161/CIRCOUTCOMES.111.962688 PMC 3332107 · doi ↗ · pubmed ↗
- 2Percutaneous closure of the left atrial appendage versus warfarin therapy for prevention of stroke in patients with atrial fibrillation: a randomised non-inferiority trial Lancet Holmes DR Reddy VY Turi ZG 53454237420091968363910.1016/S 0140-6736(09)61343-X · doi ↗ · pubmed ↗
- 32016 ESC guidelines for the management of atrial fibrillation developed in collaboration with EACTS Eur Heart J Kirchhof P Benussi S Kotecha D 289329623720162756740810.1093/eurheartj/ehw 210 · doi ↗ · pubmed ↗
- 4Left atrial appendage closure versus direct oral anticoagulants in high-risk patients with atrial fibrillation J Am Coll Cardiol Osmancik P Herman D Neuzil P 312231357520203258658510.1016/j.jacc.2020.04.067 · doi ↗ · pubmed ↗
- 5Implant success and safety of left atrial appendage closure with the WATCHMAN device: peri-procedural outcomes from the EWOLUTION registry Eur Heart J Boersma LV Schmidt B Betts TR 246524743720162682291810.1093/eurheartj/ehv 730PMC 4996118 · doi ↗ · pubmed ↗
- 6Left atrial appendage occlusion in patients older than 85 years. Safety and efficacy in the EWOLUTION registry Rev Esp Cardiol (Engl Ed) Cruz-González I Ince H Kische S 21277320203095603410.1016/j.rec.2019.02.008 · doi ↗ · pubmed ↗
- 7Patterns of comorbidities in patients with atrial fibrillation and impact on management and long-term prognosis: an analysis from the Prospective Global GLORIA-AF Registry BMC Med Romiti GF Corica B Mei DA 1512220243858986410.1186/s 12916-024-03373-4PMC 11003021 · doi ↗ · pubmed ↗
- 8Prospective randomized evaluation of the Watchman left atrial appendage closur device in patients with atrial fibrillation versus long-term warfarin therapy: the PREVAIL trial J Am Coll Cardiol Holmes DR Jr Kar S Price MJ 1126420142499812110.1016/j.jacc.2014.04.029 · doi ↗ · pubmed ↗