Obstetric and perinatal outcomes from the follow-up of a multicentre randomized controlled trial investigating time-lapse embryo monitoring
D C Kieslinger, C G Vergouw, F von Estorff, L Ramos, B Arends, M H J M Curfs, E Slappendel, E H Kostelijk, M H E C Pieters, D Consten, M O Verhoeven, D E Besselink, F Broekmans, B J Cohlen, J M J Smeenk, S Mastenbroek, C H de Koning, Y M van Kasteren, E Moll, J van Disseldorp

TL;DR
A study found that using time-lapse embryo monitoring with or without machine learning does not increase pregnancy risks compared to traditional methods.
Contribution
This study provides empirical evidence on the safety of time-lapse embryo monitoring in assisted reproduction.
Findings
No significant differences in serious pregnancy complications across groups using time-lapse monitoring versus traditional methods.
Birth weights and gestational ages were similar among all groups, indicating comparable perinatal outcomes.
Abstract
Does uninterrupted culture in a time-lapse incubator with or without a commercially available machine learning embryo selection algorithm result in comparable obstetric and perinatal outcomes as interrupted culture and morphological embryo selection? The application of uninterrupted culture in a time-lapse incubator with and without the use of an embryo selection algorithm is comparable to interrupted embryo culture and morphological embryo selection in terms of obstetric and perinatal results. There is very limited evidence regarding the safety of time-lapse monitoring (TLM) from prospective randomized controlled trials (RCT). Recent RCTs have demonstrated that the application of TLM does not increase (cumulative) live birth rates or shorten the time to pregnancy within 1 year. Although most studies only report pregnancy rates, the safety of this commonly used method is also relevant…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
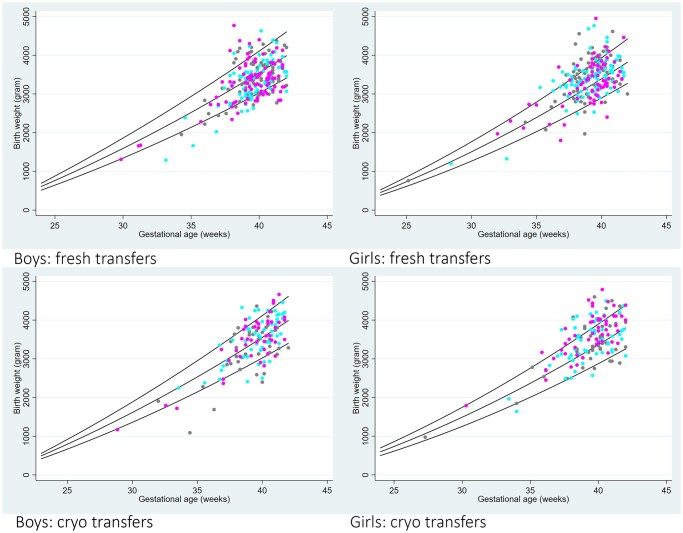 Figure 1
Figure 1|
| TLR group n = 278 | CON group n = 274 | |
|---|---|---|---|
| Female age (years) | 33.5 (4.0) | 33.0 (3.8) | 33.6 (3.9) |
| Female BMI (kg/m2) | 24.2 (4.8) | 24.0 (4.0) | 24.7 (4.7) |
| Smoking behaviour (woman) | |||
| Yes | 27 (9.6%) | 30 (10.6%) | 31 (11.2%) |
| No | 241 (85.8%) | 240 (85.1%) | 236 (85.2%) |
| Unknown | 13 (4.6%) | 12 (4.3%) | 10 (3.6%) |
| Smoking behaviour (male) | |||
| Yes | 51 (18.1%) | 51 (18.1%) | 48 (17.3%) |
| No | 201 (71.5%) | 201 (71.3%) | 207 (74.7%) |
| Unknown | 29 (10.3%) | 30 (10.6%) | 22 (7.9%) |
| Pregnancy history | |||
| Previous ongoing pregnancy | 89 (31.7%) | 73 (25.9%) | 74 (26.7%) |
| Previous miscarriage abortion, EUG | 84 (29.9%) | 71 (25.2%) | 79 (28.5%) |
| Reason for IVF/ICSI | |||
| Male factor | 115 (40.9%) | 122 (43.3%) | 115 (41.5%) |
| Female factor | 70 (24.9%) | 70 (24.8%) | 64 (23.1%) |
| Male and female factor | 15 (5.3%) | 16 (5.7%) | 15 (5.4%) |
| Unexplained | 74 (26.3%) | 70 (24.8%) | 77 (27.8%) |
| Other | 7 (2.5%) | 4 (1.4%) | 6 (2.2%) |
| Duration of infertility (months) | 35.6 (23.4) | 29.4 (18.9) | 33.1 (28.6) |
| Total FSH dose | 1616.8 (2639.0) | 1500.6 (3363.4) | 1597.3 (965.2) |
| Pre-treatment | |||
| Yes (OC or progestative) | 221 (78.6%) | 220 (78.0%) | 221 (79.8%) |
| No | 60 (21.4%) | 62 (22.0%) | 56 (20.2%) |
| Premature LH surge prevention | |||
| GnRH antagonist | 52 (18.6%) | 49 (17.4%) | 46 (16.6%) |
| GnRH agonist | 228 (81.4%) | 233 (82.6%) | 231 (83.4%) |
| Stimulation protocol | |||
| Gonal-F | 255 (90.7%) | 242 (85.8%) | 244 (88.1%) |
| Menopur | 7 (2.5%) | 15 (5.3%) | 6 (2.2%) |
| Puregon | 1 (0.4%) | 0 (0.0%) | 1 (0.4%) |
| Fostimon | 5 (1.8%) | 7 (2.5%) | 6 (2.2%) |
| Other | 13 (4.6%) | 18 (6.4%) | 20 (7.2%) |
| Fertilization method | |||
| IVF | 158 (56.2%) | 140 (49.8%) | 149 (53.8%) |
| ICSI | 118 (42.0%) | 134 (47.7%) | 126 (45.5%) |
| Both | 5 (1.8%) | 7 (2.5%) | 2 (0.7%) |
| Oocyte retrieval number | |||
| Oocyte retrieval 1 | 264 (94.0%) | 266 (94.3%) | 251 (90.6%) |
| Oocyte retrieval 2 | 13 (4.6%) | 13 (4.6%) | 21 (7.6%) |
| Oocyte retrieval 3 | 4 (1.4%) | 3 (1.1%) | 5 (1.8%) |
| TLE group (n = 571) | TLR group (n = 575) | CON group (n = 572) | Overall | TLE vs CON | TLR vs CON | |
|---|---|---|---|---|---|---|
|
|
| |||||
| Live birth | 275/571 (48.2%) | 278/575 (48.3%) | 274/572 (47.9%) | 0.99 | 1.01 (0.82–1.24) | 1.00 (0.81–1.23) |
| Stillbirth/intrauterine death | 3/571 (0.5%) | 3/575 (0.5%) | 2/572 (0.3%) | 1.47 (0.24–8.81) | 1.48 (0.24–8.88) | |
| Late miscarriage | 6/571 (1.1%) | 4/575 (0.7%) | 1/572 (0.2%) | 6.27 (0.75–52.30) | 4.13 (0.46–37.16) | |
| Induced abortion | 3/571 (0.5%) | 9/575 (1.6%) | 7/572 (1.2%) | 0.45 (0.12–1.76) | 1.33 (0.49–3.61) | |
|
| ||||||
| Serious pregnancy complications overall | 55/275 (20.0%) | 60/278 (21.6%) | 58/274 (21.2%) | 0.89 | 0.95 (0.65–1.40) | 1.03 (0.70–1.50) |
| Premature contractions (before 37 weeks pregnancy) | 2/275 (0.7%) | 3/278 (1.1%) | 2/274 (0.7%) | 0.97 (0.14–6.97) | 1.39 (0.23–8.40) | |
| Premature rupture of membranes (before 37 weeks pregnancy) | 6/275 (2.2%) | 4/278 (1.4%) | 4/274 (1.5%) | 1.49 (0.415.35) | 0.98 (0.23–3.92) | |
| Premature placental abruption | 1/275 (0.4%) | 0/278 (0.0%) | 0/274 (0.0%) | NA | NA | |
| Placenta praevia | 1/275 (0.4%) | 6/278 (2.2%) | 4/274 (1.5%) | 0.25 (0.03–2.24) | 1.46 (0.41–5.25.) | |
| High blood pressure (Hypertension) | 19/275 (6.9%) | 24/278 (8.6%) | 17/274 (6.2%) | 1.11 (0.57–2.18) | 1.38 (0.73–2.63) | |
| Pre-eclampsia | 6/275 (2.2%) | 16/278 (5.8%) | 7/274 (2.6%) | 0.85 (0.25–2.54) | 2.19 (0.87–5.38) | |
| Gestational diabetes | 11/275 (4.0%) | 10/278 (3.6%) | 11/274 (4.0%) | 0.99 (0.42–2.33) | 0.89 (0.37–2.12) | |
| Other pregnancy-related health problems | 14/275 (5.1%) | 15/278 (5.4%) | 18/274 (6.6%) | 0.83 (0.42–1.64) | 0.88 (0.45–1.72) | |
| Postpartum bleeding (>1.5 l) | 3/275 (1.1%) | 3/278 (1.1%) | 5/274 (1.8%) | 0.59 (0.14–2.48) | 0.59 (0.14–2.46) | |
| Spontaneous start of delivery | 132/275 (48.0%) | 120/278 (43.2%) | 124/274 (45.3%) | 1.06 (0.79–1.43) | 0.96 (0.71–1.29) | |
| Induced delivery | 48/275 (17.5%) | 76/278 (27.3%) | 61/274 (22.3%) | 0.78 (0.52–1.19) | 1.23 (0.84–1.79) | |
| Ventouse delivery | 21/275 (7.6%) | 29/278 (10.4%) | 26/274 (9.5%) | 0.79 (0.44–1.46) | 1.08 (0.62–1.88) | |
| Caesarean section | 39/275 (14.2%) | 51/278 (18.3%) | 51/274 (18.6%) | 0.76 (0.39–1.49) | 1.06 (0.57–1.98) | |
|
| ||||||
| Term birth (≥37 weeks) | 255/275 (92.7%) | 261/278 (93.9%) | 257/274 (93.5%) | 0.98 (0.78–1.22) | 1.01 (0.80–1.2820) | |
| Preterm birth (<37 weeks) (n = 54) | 20/275 (7.3%) | 17/278 (6.1%) | 17/274 (6.2%) | 1.18 (0.62–2.21) | 0.99 (0.51–1.89) | |
| Fresh ET (n = 497) | 12/162 (7.4%) | 10/161 (6.2%) | 8/174 (4.6%) | |||
| FET (n = 294) | 6/97 (6.2%) | 7/108 (6.5%) | 7/89 (7.9%) | |||
| Natural conception (n = 36) | 2/16 (12.5%) | 0/9 (0.0%) | 2/11 (18.2%) | |||
| Very preterm birth (<32 weeks) | 4/275 (1.5%) | 1/278 (0.4%) | 2/274 (0.7%) | 1.95 (0.35–10.76) | 0.7 (0.04–5.19) | |
| Weight at birth in g as mean (SD) (n = 816) | 3413 (588) | 3412 (588) | 3377 (578) | 0.70 | MD 34 (−62 to 129) | MD 32 (−635 to 128) |
| Low birth weight (<2500 g) | 17/270 (6.3%) | 12/275 (4.4%) | 16/271 (5.5%) | 1.08 (0.53–2.18) | 0.764 (0.35–1.638) | |
| Very low birth weight (<1500 g) | 2/270 (0.7%) | 2/275 (0.7%) | 3/271 (1.1%) | 0.67 (0.11–4.05) | 0.66 (0.10–3.99) | |
| Gestational age at birth as mean (SD) (n = 815) | 39.4 (1.9) | 39.5 (1.5) | 39.3 (1.9) | #MD 0.09 (−0.211 to 0.40) | #MD 0.17 (−0.14 to 0.47) | |
| Fresh ET (n = 494) | 39.4 (1.9) | 39.4 (1.5) | 39.4 (1.7) | |||
| FET (n = 285) | 39.5 (2.0) | 39.7 (1.6) | 39.3 (2.2) | |||
| Natural conception (n = 36) | 39.5 (1.9) | 39.3 (0.8) | 39.0 (2.2) | |||
| Apgar score at 1 min as mean (SD) (n = 469) | 8.67 (1.66) | 8.53 (1.79) | 8.20 (2.35) | MD 0.47 (0.03–0.91) | MD 0.34 (−0.08 to 0.77) | |
| Apgar score at 5 min (n = 456) | 9.59 (1.35) | 9.58 (1.23) | 9.44 (1.34) | MD 0.37 (−0.01 to 0.75) | MD 0.36 (−0.00 to 0.73) | |
| Apgar score <4 at 5 min (n = 456) | 1/137 (0.7%) | 3/160 (1.9%) | 2/159 (1.3%) | |||
| Major congenital malformations | 4/275 (1.5%) | 4/278 (1.4%) | 7/274 (2.5%) | 0.57 (0.17–1.99) | 0.44 (0.11–1.72) | |
| Minor congenital malformations | 5/275 (1.8%) | 3/278 (1.1%) | 5/274 (1.8%) | 0.99 (0.28–3.47) | 0.58 (0.14–2.48) | |
| Health problems directly after birth | 8/275 (2.9%) | 12/278 (4.3%) | 11/274 (4.0%) | 0.76 (0.31–1.88) | 1.04 (0.44–2.45) |
- —Netherlands Organisation for Health Research and Development10.13039/501100001826
- —SelecTIMO study
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOvarian function and disorders · Reproductive Biology and Fertility · Preterm Birth and Chorioamnionitis
Introduction
IVF laboratories try to improve clinical success rates by offering the latest innovations and techniques to their patients. It is of utmost importance to provide the best possible culture environment for the developing embryos and to select the highest quality embryo for transfer to achieve a healthy pregnancy and live birth. Time-lapse monitoring (TLM) is a technique that has been introduced to IVF centres worldwide a decade ago, even though there was insufficient evidence for its effectiveness and safety available at the time. Two reasons were advocated why TLM would optimize IVF procedures and improve clinical results. First, built-in cameras obviate the need to remove embryos from the incubator for morphological assessments, thereby providing very stable culture conditions (Aparicio et al., 2013). Second, TLM generates detailed information on embryo development, which can be used by embryologists, artificial intelligence, or computer software for optimal embryo selection (Wong et al., 2013; Berntsen et al., 2022).
Recent randomized controlled trials (RCT) have demonstrated that the application of TLM does not increase (cumulative) live birth rates or decrease the time to pregnancy within 1 year (Goodman et al., 2016; Ahlstrom et al., 2022; Kieslinger et al., 2023; Bhide et al., 2024; Illingworth et al., 2024). However, most data on the safety of TLM stem from retrospective studies or small RCTs and there is limited evidence from large RCTs.
A retrospective follow-up study of an RCT concluded that there were no differences between time-lapse and conventional incubators regarding the obstetric and perinatal outcomes of singleton ongoing pregnancies (Insua et al., 2017). Another RCT also reported no differences regarding perinatal outcomes (Kovacs et al., 2019). Both studies compared different types of conventional incubators to a time-lapse incubator. A pragmatic multicentre RCT on TLM reported reassuring results regarding major congenital anomalies and adverse events (Bhide et al., 2024).
Recently, 1731 IVF/ICSI patients participated in a three-armed, multicentre, double-blind, RCT (Kieslinger et al., 2023). All embryos were cultured in the same time-lapse incubator (Geri+). The aim of the current study was to compare the safety of uninterrupted embryo culture using TLM (with and without the use of machine learning for embryo selection) and interrupted culture (with morphological embryo selection). To assess the safety, we evaluated the obstetric and perinatal data for all singleton ongoing pregnancies occurring within 1 year after fresh single embryo transfer (SET) and single frozen embryo transfer (FET) associated with the initial oocyte retrieval cycle, as well as natural conceptions.
Materials and methods
Study setting, design, and population
Three groups were compared: (i) TLE (Time-Lapse Eeva^®^): embryo selection based on the Eeva^®^ Test (a Day 3 TLM algorithm based on machine learning, used adjunctively with morphology to predict blastocyst formation without the need for extended culture until Day 5) and uninterrupted culture; (ii) TLR (Time-Lapse Routine): routine morphological embryo selection and uninterrupted culture; and (iii) CON (Control group): routine morphological embryo selection and interrupted culture.
The embryos in all three groups were cultured in a Geri+ time-lapse incubator (Genea Biomedx, Sydney, NSW, Australia) under 5% O_2_ and 5–6% CO_2_.
Patients were recruited at five independent IVF laboratories and 10 associated fertility clinics in the Netherlands between June 2017 and March 2020 (Kieslinger et al., 2023). The trial protocol was first approved on 22 December 2016 by the Central Committee on Research involving Human Subjects (The Hague, The Netherlands) and by the board of directors of each participating clinic. Participating couples provided written informed consent. The study was registered at Trial Search on 8 September 2015 (NTR5423: ICTRP Search Portal (who.int)).
Couples in their first, second, or third IVF or ICSI oocyte retrieval cycle were invited to participate if they were planning to have a fresh SET. Couples could only participate once. Exclusion criteria were: planned double embryo transfer, planned freeze all cycle without a fresh embryo transfer, participation in another scientific study, use of donor gametes, preimplantation genetic testing and the use of thawed oocytes. All women were 42 years or younger, since IVF treatment is covered by Dutch health insurances until this age. Randomization was conducted centrally in Castor (a web-based, online randomization tool) and stratified by laboratory site and oocyte retrieval cycle number.
In the TLE and TLR groups, zygotes were transferred to Geri+ culture dishes after fertilization check on Day 1 and kept in the incubator without disturbances until Day 3, thereby providing uninterrupted culture conditions. In the CON group, the standard dishes of each laboratory were used for embryo culture, which were removed from the incubator two additional times for embryo assessments under a conventional microscope between Day 1 and Day 3, thereby providing interrupted culture conditions. Embryos were cultured in individual medium droplets in the CON group (20–50 µl) and in group culture microwell droplets (80 µl) in the TLE and TLR groups.
Geri+ incubator software version 5.3-6.0, Geri connect software version 1.0-2.0 and Eeva^®^ system version 3.0-3.1 were used in the trial. Images in 11 focal planes were captured for each embryo in the TLE and TLR groups every 5 min with a total light exposure time of ∼125 s per day per embryo. Fresh embryo transfers were conducted on Day 3. Embryo selection in the TLE group was based on the results of the EEVA^®^ Test in combination with morphology. Embryo selection in the TLR and CON groups was based on routine morphology. All embryos were cultured in the Geri+ incubator until the moment of cryopreservation. Embryos with the highest Eeva^®^ Test result (TLE) or best morphology (TLR and CON) were frozen and thawed first. All laboratories adhered to the study protocol, but other than that, used their own laboratory protocols, culture media, and cryopreservation techniques.
Additional details concerning randomization and IVF protocols can be found in our previously published article (Kieslinger et al., 2023).
Data sources
Obstetric and perinatal data were primarily based on medical records and entered by research personnel and fertility doctors of each participating clinic in Castor, a web-based, clinical data management platform. The outcomes of all pregnancies occurring after fresh embryo transfers and FETs associated with the initial oocyte retrieval cycle as well as natural conceptions within 1 year were recorded. Additionally, patients were asked to fill in an online questionnaire about their pregnancy, delivery, and child (Castor). Apgar score results were based on data from questionnaires only. Data entered by research personnel and information reported by patients were cross-checked, harmonized, and subsequently categorized.
Outcome measurements
The following obstetric outcomes (where applicable with or without hospital admission) were recorded separately: premature contractions (before 37 weeks of gestation), premature rupture of membranes (before 37 weeks of gestation), premature placental abruption, placenta praevia, hypertension, pre-eclampsia, gestational diabetes, postpartum bleeding (>1.5 l), and other serious pregnancy-related health problems (hyperemesis gravidarum, pelvic floor disorders, and others). The occurrence of at least one of the above complications including preterm birth before 37 weeks was registered as serious pregnancy complications overall. The following modes of delivery were recorded: spontaneous start of delivery, induced delivery, ventouse delivery, and caesarean section.
Perinatal outcomes were live birth, stillbirth/intrauterine death, term birth after ≥37 weeks, preterm birth (<37 weeks), and very preterm birth (<32 weeks), weight at birth, low birth weight (<2500 g), very low birth weight (<1500 g), gestational age at birth, Apgar score at 1 and 5 min, minor and major congenital malformations, and health problems directly after birth, such as dysmaturity, breathing problems, or neonatal hypoglycaemia. Congenital malformations were defined according to the manual from the World Health Organization published in 2020: Major congenital malformations are structural changes that have significant medical, surgical, social, or cosmetic consequences for the affected individual, and typically require medical intervention. Examples include spina bifida, anencephaly, heart defects, and orofacial clefts. Minor congenital malformations are structural changes that pose little or no significant health problem and tend to have limited social or cosmetic consequences for the affected individual. Examples of minor anomalies include single palmar crease and clinodactyly (mild curvature of a finger) (World Health Organization, 2020).
Sample size considerations
The clinical outcomes of 1731 randomized couples were included in this analysis. The sample size for this study was not aimed at safety outcomes but based on the ability to demonstrate an absolute difference of 7.5% or more in cumulative ongoing pregnancy (Kieslinger et al., 2023). For obstetric outcomes, we considered serious pregnancy complications overall to be our main outcome. As we had at least 274 singleton deliveries in each allocated group, this sample size would allow us enough power to detect a difference of 10% compared to a control proportion of 20%. For perinatal outcomes, we considered the weight of the neonate our main outcome; with at least 274 singletons per group, this would allow us to detect a mean difference of 144 g or more (expected weight of 3400 and SD of 600).
Statistical analysis
In view of the many outcomes and comparisons, we present data descriptively and calculated age-adjusted effect measures with 95% confidence intervals for TLE and TLR compared to CON for singleton pregnancies only. P-values were calculated only for the main safety outcomes. For linear outcomes, we used a generalized linear model adjusted for maternal age to estimate mean differences between TLE and CON and TLR and CON. In case the outcome had a skewed distribution, a gamma with log link model was used. For binary outcomes, a generalized linear model using a negative binomial with log link adjusted for maternal age was applied to estimate adjusted relative risks between TLE and CON and TLR and CON.
Regression analyses of weight percentiles of children born after fresh embryo transfers and FETs were conducted. Z-scores for birth weight by gestational age in weeks were placed in the Dutch reference curves for boys and girls. Percentiles for birth weight by gestational age were analysed for fresh embryo transfers and FETs and gender separately. All outcomes were reported for singleton pregnancies.
Results
Our analysis is based on 873 women who had an ongoing pregnancy during the follow-up period of 1 year. In total, 39 women experienced a late miscarriage, induced abortion, stillbirth, or intrauterine death, or were lost to follow-up after an ongoing pregnancy was confirmed. Of these 39 women, 6 had a live birth after a subsequent treatment cycle within 1 year, bringing the total to 840 women who delivered during the 1-year follow-up period. There were 827 singleton and 13 twin deliveries. One neonatal death occurred following the delivery of a singleton in the CON group.
Baseline characteristics of all patients who had a singleton live birth are presented in Table 1.
Obstetric outcomes
Table 2 reports the cumulative outcomes for all singleton live births. No statistically significant differences between the three groups were observed for the percentage of serious pregnancy complications overall (TLE = 20.0% (55/275), TLR = 21.6% (60/278), CON = 21.2% (58/274); P = 0.89). Comparing TLE and TLR with CON, the age-adjusted RR did not indicate significant differences in premature contractions, premature rupture of membranes, premature placental abruption, placenta praevia, high blood pressure, pre-eclampsia, gestational diabetes, postpartum bleeding, or other pregnancy-related health problems.
Regarding the delivery mode, the number of women who had a spontaneous start of delivery, induced delivery, ventouse delivery, or caesarean section was comparable between the groups.
Perinatal outcomes
Of the 827 women who gave birth to a singleton, 497 deliveries originated from a fresh embryo transfer (60%), 294 from a FET (36%), and 36 women conceived naturally (4%), with similar proportions in each study group. The 12-month cumulative live birth rate was 48.2% (275/571) in the TLE group, 48.3% (278/575) in the TLR group, and 47.9% (274/572) in the CON group (P = 0.99). Stillbirth/intrauterine death rates were comparable between the three groups (TLE = 0.5% (3/571), TLR = 0.5% (3/575), CON = 0.3% (2/572)).
The preterm birth rate (<37 weeks) was 7.3% (20/275) in the TLE group, 6.1% (17/278) in the TLR group, and 6.2% (17/274) in the CON group. The very preterm birth rate (<32 weeks) was 1.5% (4/275) in the TLE group, 0.4% (1/278) in the TLR group, and 0.7% (2/274) in the CON group.
Mean (SD) weight at birth was 3413 (588) g in the TLE group, 3412 (588) g in the TLR group, and 3377 (578) g in the CON group (P = 0.70). Regression analyses of birth weight percentiles of boys and girls born after fresh and FETs indicated no differences between the three treatment groups (Fig. 1). The proportions of children born with low and very low birth weight were comparable between the groups. Taken together, when the randomization group was not considered, children born after fresh embryo transfer had an average birth weight of 3360 (541) g, after FET 3476 (613) g, and after natural conception 3351 (543) g.
Birth weights plotted against gestational age in weeks placed in the Dutch reference curves for boys and girls. Coloured dots represent birthweight in the TLE group (pink), TLR group (turquoise), and CON group (grey). TLE, embryo selection based on a commercially available Day 3 TLM algorithm, used adjunctively with morphology, and uninterrupted culture; TLR, routine morphological embryo selection and uninterrupted culture; CON, routine morphological embryo selection and interrupted culture.
Mean (SD) gestational age at birth was 39.4 (1.9) weeks in the TLE group, 39.5 (1.5) weeks in the TLR group, and 39.3 (1.9) weeks in the CON group. Mean Apgar score after delivery was comparable between the groups.
Major congenital malformations occurred in four children in the TLE group, four in the TLR group, and seven in the CON group. Minor congenital malformations occurred in five children in the TLE group, three in the TLR group, and five in the CON group.
Health problems immediately after delivery were reported for eight babies in the TLE group, 12 in the TLR group, and 11 in the CON group.
Of all 13 twin pregnancies, five occurred after fresh embryo transfer (4 SET, 1 DET), six after FET (6 SET), and two were natural conceptions.
Discussion
In this study, we examined the obstetric and perinatal outcomes of a multicentre RCT on TLM. We found that uninterrupted culture in a TLM incubator with and without the application of a machine learning embryo selection algorithm is safe in terms of obstetric and perinatal results compared to interrupted culture and morphological selection.
The incidence of serious pregnancy complications overall was very similar in the three groups. Pre-eclampsia was more often observed in the TLR group but the age-adjusted RR did not indicate a significant difference compared to the CON group. Two other studies have also found no indication that obstetric risks, including hypertensive disorders, are higher with TLM (Insua et al., 2017; Ahlstrom et al., 2023).
The proportion of women who had a spontaneous start of the delivery, induced delivery, ventouse delivery, or caesarean section was similar in the three groups. Previous studies only compared the number of caesarean sections between time-lapse and standard incubation. A retrospective analysis of data from an RCT found a lower number of caesarean sections in the time-lapse group (Insua et al., 2017), while a large population-based retrospective analysis reported no differences for the number of caesarean sections (Ahlstrom et al., 2023).
The proportion of preterm and very preterm births was comparable in the three groups, which is consistent with evidence from most earlier studies (Insua et al., 2017; Kovacs et al., 2019; Ma et al., 2022; Ahlstrom et al., 2023). One study found a lower risk for preterm births in the time-lapse group, but the retrospective cohort study design of this report should be considered when interpreting the results (Mascarenhas et al., 2019).
No significant differences were observed between the three groups for average birth weight. The proportion of children born with a low and very low birth weight was also comparable across groups. Five other studies have also reported no differences between time-lapse and standard incubation regarding birth weight (Insua et al., 2017; Kovacs et al., 2019; Ma et al., 2022; Ahlstrom et al., 2023; Bhide et al., 2024). The two studies, which reported a higher mean birth weight in the TLM group compared to conventional incubation should be interpreted with caution: the first because of its retrospective design (Mascarenhas et al., 2019) and the second because of the use of double embryo transfers (Guo et al., 2021). When data from all three treatment groups were pooled, our study confirmed the findings from earlier meta-analyses, which showed that children born after fresh embryo transfer have a lower average birth weight compared to children born after FET (Maheshwari et al., 2018; Zaat et al., 2021). It has been proposed that the lower birth weight in children born after fresh transfer may be related to ovarian stimulation during the oocyte retrieval cycle and corresponding hormonal changes that affect the uterine environment (van Duijn et al., 2021). Gestational age at delivery was similar in the three groups, as was also described by six other studies (Insua et al., 2017; Kovacs et al., 2019; Mascarenhas et al., 2019; Ma et al., 2022; Ahlstrom et al., 2023; Bhide et al., 2024).
The health of children born in this study was not affected by randomization to the TLE, TLR, or CON group. Health problems directly after delivery, Apgar scores, the rates of major and minor congenital malformations, late miscarriages, and stillbirth/intrauterine deaths were all found to be comparable in all three groups. These findings are reassuring and generally in line with other studies (Insua et al., 2017; Ma et al., 2022; Ahlstrom et al., 2023; Bhide et al., 2024).
Strengths of our study include the broad inclusion criteria and multicentre design. Furthermore, our results are very robust, since each of the five laboratories used their own laboratory protocols, incubator settings, culture media, standard dishes, and cryopreservation techniques. Moreover, patients received a SET in almost all cases, with the exception of 18 of 1731 patients (1%) who changed their mind after randomization. Most pregnancies involved singleton births. Thirteen twin deliveries, 10 of which followed SET, were excluded from the analysis due to the increased risk of maternal and perinatal complications associated with multiple pregnancies (Rao et al., 2004).
In our study, embryos in the TLE and TLR groups were cultured in micro-wells, which shared a common culture medium well, whereas embryos in the CON group were cultured in individual medium droplets. While such methodological differences in embryo culture conditions may influence embryo development, they do not appear to have affected our clinical outcomes. Findings from previous studies on group versus individual culture have not been consistent, with some reporting an effect on clinical outcomes and others observing no significant difference (Ebner et al., 2010; Fancsovits et al., 2022; Herreros et al., 2024). In our study, embryos in all groups were cultured in the same time-lapse incubator. The control group reflected embryo culture conditions in a benchtop incubator. This approach had the advantage of a direct and clear comparison of uninterrupted and interrupted culture conditions and embryo selection methods, while minimizing interference from other incubator variables. However, a limitation of our control group is that our results cannot be used to draw conclusions about the safety of TLM compared to big box incubators. Embryos of multiple patients are cultured simultaneously in big box incubators, which leads to more door openings and thereby disturbances compared to benchtop incubators. However, the available data from three other RCTs also suggest that TLM is safe to use in comparison to several conventional incubators (Insua et al., 2017; Kovacs et al., 2019; Bhide et al., 2024).
Another limitation of our study is that we only tested one time-lapse incubator, while more systems are currently available. It is advisable to report the safety of this add-on technique for each of the available time-lapse systems. Obstetric and perinatal data were recorded by research personnel based on hospital records. We also obtained data from patients with an online questionnaire. Discrepancies in data retrieved from questionnaires were carefully cross-checked with information recorded by research personnel to ensure consistency between both data sources, because self-reported data can be less accurate. In total, 72% of the patients who had a singleton ongoing pregnancy replied to our questionnaires. APGAR scores were retrieved from patient questionnaire only and therefore, this outcome should be considered with care. Power calculations were conducted for primary outcomes of the RCT. We are aware that imprecision for many of the comparisons reported here is sizeable.
In conclusion, our study shows that uninterrupted embryo culture with or without a TLM selection algorithm based on machine learning does not pose any obstetric or perinatal risks when compared to routine interrupted culture and morphological embryo selection. However, long-term data are not yet available and therefore, potential epigenetic effects, which may manifest later in life, cannot be excluded based on our data.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ahlstrom A , Lundin K, Cimadomo D, Coticchio G, Selleskog U, Westlander G, Winerdal J, Stenfelt C, Callender S, Nyberg C et al No major differences in perinatal and maternal outcomes between uninterrupted embryo culture in time-lapse system and conventional embryo culture. Hum Reprod 2023;38:2400–2411.37879843 10.1093/humrep/dead 219 · doi ↗ · pubmed ↗
- 2Ahlstrom A , Lundin K, Lind AK, Gunnarsson K, Westlander G, Park H, Thurin-Kjellberg A, Thorsteinsdottir SA, Einarsson S, Astrom M et al A double-blind randomized controlled trial investigating a time-lapse algorithm for selecting day 5 blastocysts for transfer. Hum Reprod 2022;37:708–717.35143661 10.1093/humrep/deac 020PMC 9383441 · doi ↗ · pubmed ↗
- 3Aparicio B , Cruz M, Meseguer M. Is morphokinetic analysis the answer? Reprod Biomed Online 2013;27:654–663.24135156 10.1016/j.rbmo.2013.07.017 · doi ↗ · pubmed ↗
- 4Berntsen J , Rimestad J, Lassen JT, Tran D, Kragh MF. Robust and generalizable embryo selection based on artificial intelligence and time-lapse image sequences. P Lo S One 2022;17:e 0262661.35108306 10.1371/journal.pone.0262661 PMC 8809568 · doi ↗ · pubmed ↗
- 5Bhide P , Chan DYL, Lanz D, Alqawasmeh O, Barry E, Baxter D, Gonzalez Carreras F, Choudhury Y, Cheong Y, Chung JPW et al Clinical effectiveness and safety of time-lapse imaging systems for embryo incubation and selection in in-vitro fertilisation treatment (TILT): a multicentre, three-parallel-group, double-blind, randomised controlled trial. Lancet 2024;404:256–265.39033010 10.1016/S 0140-6736(24)00816-X · doi ↗ · pubmed ↗
- 6Ebner T , Shebl O, Moser M, Mayer RB, Arzt W, Tews G. Group culture of human zygotes is superior to individual culture in terms of blastulation, implantation and life birth. Reprod Biomed Online 2010;21:762–768.21051291 10.1016/j.rbmo.2010.06.038 · doi ↗ · pubmed ↗
- 7Fancsovits P , Pribenszky C, Lehner A, Murber A, Kaszas Z, Nemes A, Urbancsek J. Prospective-randomized study comparing clinical outcomes of IVF treatments where embryos were cultured individually or in a microwell group culture dish. Biol Futur 2022;73:229–236.35278201 10.1007/s 42977-022-00113-8 · doi ↗ · pubmed ↗
- 8Goodman LR , Goldberg J, Falcone T, Austin C, Desai N. Does the addition of time-lapse morphokinetics in the selection of embryos for transfer improve pregnancy rates? A randomized controlled trial. Fertil Steril 2016;105:275–285.e 10.26522611 10.1016/j.fertnstert.2015.10.013 · doi ↗ · pubmed ↗