Impact of initial hematocrit levels during direct procurement and perfusion on the likelihood of primary graft dysfunction in donation after circulatory death heart transplantation
Emmanuel Odekunle, Adham Makarem, George Olverson, Kamila Drezek, Eriberto Michel, David D’Alessandro, Ioannis Mastoris, Shannon N. Tessier, Asishana Osho, S. Alireza. Rabi

TL;DR
This study examines how hematocrit levels during heart perfusion affect transplant outcomes, finding no significant benefit from higher levels.
Contribution
The study provides new insights into the clinical impact of hematocrit levels during heart perfusion in transplantation.
Findings
Higher hematocrit levels did not reduce primary graft dysfunction.
Higher hematocrit was linked to increased postoperative support requirements.
No significant difference in graft dysfunction was observed between hematocrit groups.
Abstract
Optimizing perfusion parameters when using ex vivo heart perfusion systems is critical for maximizing organ quality and extending perfusion duration. Hematocrit (HCT) of the perfusate may influence oxygen delivery and perfusion dynamics, yet its clinical significance remains uncertain. In this retrospective single-center study, we utilize regression models to explore the relationship between hematocrit (HCT) of the device perfusate during normothermic machine perfusion (using the Transmedics Organ System [OCS]) and recipient outcomes following transplantation. Cohorts with HCT <15% packed cell volume [PCV] were compared with those with HCT ≥15% PCV. Among 74 recipients, moderate and severe primary graft dysfunction (defined as needing extracorporeal machine oxygenation post-transplant) did not differ significantly between cohorts. Mean inotrope scores 48 hours post admission were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
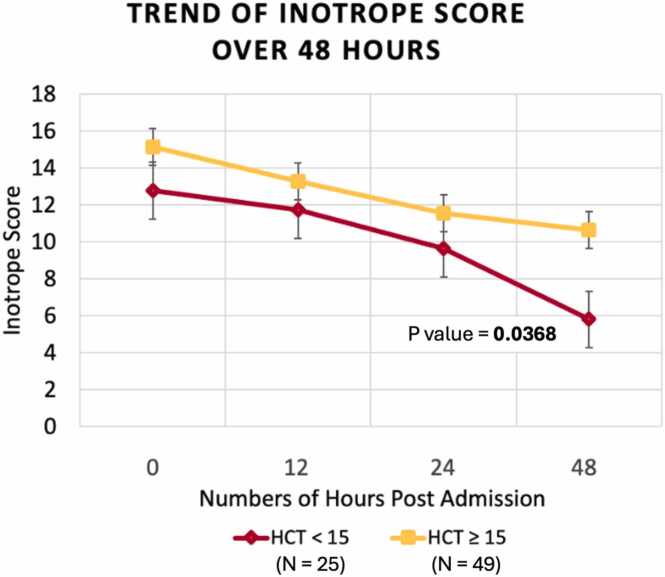 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTransplantation: Methods and Outcomes · Organ Transplantation Techniques and Outcomes · Mechanical Circulatory Support Devices
Background
Donation after circulatory death (DCD) heart transplantation presents challenges due to warm ischemia time (WIT), which some studies suggest is associated with increased risk of primary graft dysfunction (PGD).1, 2 To mitigate these risks, many centers have adopted the direct procurement and perfusion method, wherein the heart is perfused ex vivo using normothermic, oxygenated donor blood. This perfusate is crucial for maintaining the heart’s vitality during the procurement process, as it is purported to provide adequate oxygen, nutrition, and metabolic substrates.3 This study aims to investigate whether increased hematocrit (HCT) levels in the perfusate might offer protective effects by reducing the likelihood of PGD, among other outcomes, in DCD heart transplant recipients.
Methods
This single-center retrospective study examined DCD heart transplants performed at Massachusetts General Hospital between December 2019 and January 2023. Hearts were procured using the Transmedics OCS ex vivo normothermic perfusate system, and perfusate HCT was measured at time of sampling via i-STAT CG8+ analysis within 10 minutes of perfusion initiation. These printouts do not provide measurements of free heme. Hearts were stratified into 2 groups: HCT ≥15% packed cell volume (PCV) and HCT <15% PCV, with 15% as the lower limit of the i-STAT analysis.
Outcomes analyzed included PGD incidence and extracorporeal machine oxygenation (ECMO) utilization. Secondary outcomes were intensive care unit (ICU) and hospital length of stay, pre- and post-transplant arterial and venous lactate levels, and inotropic support scores at ICU admission and 48 hours post admission. PGD and inotropes, as calculated below, were defined per International Society for Heart and Lung Transplant consensus guidelines.4, 5 Inotropes were weaned primarily based on achieving a cardiac index >2.2 liter/min/m^2^. Additional criteria included a serum lactate <2.0 mmol/liter and clinical signs of adequate tissue perfusion. Vasopressors were weaned based on achieving a mean arterial pressure ≥65 mm Hg. Perioperative care protocols were standardized to minimize variability. A multidisciplinary heart failure team rounded on patients daily and applied these standardized protocols, which helped ensure consistency. Although physician discretion remained a factor, adherence to the established criteria supported uniformity between groups.
Continuous variables are presented as medians with interquartile ranges or means with standard deviations, while categorical variables are reported as frequencies with percentages. Continuous variables were compared using the Wilcoxon Rank Sum test or the independent samples t-test, depending on normality assessed via histograms. Categorical variables were analyzed using the chi-square test or Fisher’s exact test. HCT was treated as a binary variable. Associations with study outcomes were assessed using simple linear regression for continuous outcomes and univariate logistic regression for binary outcomes. To assess for potential timeline, we examined the perfusate HCT levels distribution over time and discovered no systematic trend that would be indicative of earlier transplants receiving higher or lower HCT perfusates thus reducing the likelihood of a confounding learning curve or evolution of protocol.
The analysis included less than 5% missing data, addressed via complete case analysis. Statistical significance was set at a p-value of <0.05. Analyses were performed using SAS 9.4 (SAS Institute, Cary, NC).
Results
Seventy-four DCD heart transplant recipients (HCT < 15% PCV: N = 25; HCT ≥ 15% PCV: N = 49) were included with findings reported in Tables 1 and 2. Baseline donor and recipient demographics were similar between groups (Table 1). Procedure and hemodynamic characteristics 24 hours post ICU admission were not statistically different between cohorts (Table 2).Table 1. Baseline Donor and Recipient Demographics in PGD Following DCD Heart TransplantationTable 1VariablesHCT < 15(n = 25)HCT ≥ 15(n = 49)p-valueRecipient characteristicsAge, year, median [Interquartile Range (IQR)]55 [44, 63]57 [47, 62]0.6985Male, sex, n (%)18 (72)39 (79.6)0.5615Height, m1.7335 (0.092)1.7496 (0.077)0.4315Weight, kg82.8 (15.3)86.4 (14.4)0.3205Body Mass Index (BMI), kg/m^2^27.5 (4.5)28.2 (4.2)0.5013Blood group0.2653 O14 (56)29 (59.2) A11 (44)16 (32.7) B0 (0)4 (8.1) AB0 (0)0 (0)Race0.4717 White20 (80)39 (79.6) Black3 (12)5 (10.2) Other2 (8)5 (10.2)Cardiac disease etiology0.1571 Nonischemic dilated cardiomyopathy12 (48)26 (53) Ischemic dilated cardiomyopathy9 (36)16 (32.7) Other4 (16)7 (14.3)Durable left ventricular assist device14 (56)24 (49)0.8908Chronic kidney disease9 (36)21 (42.9)0.6239Diabetes mellitus10 (40)18 (36.7)0.7166Hyperlipidemia14 (56)23 (46.9)0.6235Coronary artery disease12 (48)23 (46.9)0.9311Prior sternotomy14 (56)32 (65.3)0.4580History of smoking10 (40)25 (51)0.4625Donor characteristicsAge, years, median [IQR]28 [25, 33]33 [26, 39]0.1026Male, sex, n (%)21 (84)40 (81.6)0.8002Donor-recipient sex mismatch7 (28)11 (22.4)0.5986Height, m1.762 (0.113)1.764 (0.083)0.9171Weight, kg85.1 (15.1)91.9 (18.2)0.1074BMI, kg/m^2^27.5 (5.2)29.6 (6.2)0.1522Left ventricular ejection fraction63.5 (6.4)61.7 (6.4)0.2410Cause of death/mechanism of injury0.5536 Anoxia12 (48)26 (53) Cerebrovascular accident1 (4)6 (12.2) Head trauma11 (44)16 (32.7) Other1 (4)1 (2.1)Abbreviations: DCD, donation after circulatory death; HCT, hematocrit; PGD, primary graft dysfunction.Table 2. Procedure and Hemodynamic CharacteristicsTable 2VariablesHCT < 15(n = 25)HCT ≥ 15(n = 49)p-valueProcedure characteristicsWarm ischemic time, minutes22 [19, 24]21 [18, 25]0.7658OCS perfusion time, minutes246 [232, 278]254 [220, 290]0.6353Cardiopulmonary bypass time199 [165, 214]194 [167, 236]0.9635*Hemodynamic characteristics (24 hours post ICU admission)*Mean arterial pressure74 [71, 84]74.5 [70, 81.5]0.9768Heart rate109 [108, 109]109 [108, 110]0.8740Central venous pressure11 [8, 13]11.5 [9.5, 14]0.2850Mean pulmonary artery pressure19 [15, 24]20 [18, 23]0.4521Abbreviations: HCT, hematocrit; OCS, Organ Care System.
There were no significant differences in moderate or severe PDG incidence (p = 0.8654, odds ratio (OR) 0.90, 95% confidence interval (CI) 0.26-3.04), and ECMO utilization (HCT < 15%: 4 (16%) vs HCT ≥ 15%: 9 (18.37%); p = 0.8002) (Table 3). The odds of PGD (p = 0.8654, OR 0.90 95% CI 0.266-3.042) and ECMO requirement (p = 0.8003, OR 1.181 95% CI 0.325-4.295) were not significantly different between groups.Table 3. Outcomes of Patients Following DCD Heart Transplantation Categorized by HCT LevelTable 3OutcomesHCT < 15(n = 25)HCT ≥ 15(n = 49)p-valuePGD0.8654 None20 (80)40 (81.6) Moderate1 (4)2 (4.1) Severe4 (16)7 (14.3)ECMO4 (16)9 (18.37)0.8002Post-transplant hospital length of stay, days14 [11, 20]19 [14, 26]0.3719Post-transplant intensive care unit length of stay, days6 [5, 7]8 [6, 12]0.1042Venous delta lactate1.75 (1.14)2.09 (1.41)0.3534Arterial delta lactate1.80 (1.47)1.91 (1.33)0.7503Inotrope score Admission12.77 (5.47)15.16 (7.77)0.1734 48 hours after admission5.79 (4.57)10.64 (10.89)0.0368Postoperative complications7 (35)17 (39.5)0.7301Postoperative stroke0 (0)2 (4.6)0.3270Postoperative sepsis1 (5)4 (9.3)0.5565Postop renal failure1 (7.7)9 (34.6)0.0695Post-Op-ReOp bleeding3 (15)4 (9.3)0.5030Prolonged ventilation10 (50)20 (46.5)0.7964Rate of survival25 (100)44 (91.7)0.9567Abbreviations: DCD, donation after circulatory death; ECMO, extracorporeal machine oxygenation; HCT, hematocrit; PGD, primary graft dysfunction.Italic p-value represents a statistically significant p-value based on an alpha of 0.05.
The mean inotrope score 48 hours post admission was significantly higher in DCD recipients with higher perfusate HCT (5.79 vs 10.64; p = 0.0368), although the inotrope score at admission was similar between the groups (Table 3). There was also a trend toward longer hospital (14 vs 19; p = 0.3719) and intensive care unit (6 vs 8; p = 0.1042) length of stay for the higher HCT group, though this difference did not reach statistical significance (Table 3). A similar trend was observed for postoperative renal dysfunction in the higher HCT cohort, although it did not reach statistical significance (Table 3).
Discussion
There is considerable variability in the HCT percentage among hearts perfused via direct procurement and perfusion using the Transmedics OCS. This analysis demonstrates that higher perfusate HCT during ex vivo machine is not associated with significant reductions in PGD or ECMO utilization but may correlate with elevated inotrope requirements post transplant (Figure 1). These findings raise valuable questions on the potential impact of perfusate composition on graft quality and patient outcomes.Figure 1. Graph showing the association between higher hematocrit levels during ex vivo heart perfusion and duration of inotrope use. HCT, hematocrit.Figure 1
These findings suggest that lower HCT levels during ex vivo heart perfusion—relative to physiologic levels in the recipient—might be protective for the transplanted heart. While the presence of RBCs in the perfusate contributes to oxygen delivery, the ideal HCT range remains undefined. Although vascular resistance is primarily influenced by vessel size, increased viscosity within the perfusate at higher HCT levels could contribute to reduced perfusion efficiency during ex vivo perfusion.6 Consequently, our higher HCT group may have increased viscosity, potentially leading to perfusion issues that become apparent only after transplantation.7 The observed trend toward higher postoperative renal failure in the higher HCT cohort may be part of the same physiologic process. Increased perfusate viscosity may impair microcirculatory flow, leading to subclinical myocardial ischemia and reduced early graft recovery. This may, in turn, compromise systemic perfusion and renal blood flow post-transplant, contributing to transient renal dysfunction. Higher HCT levels in the perfusate could also result in increased hemolysis-induced graft injury due to the introduction of hemolytic toxins.8, 9 These results contrast with findings from lung transplantation studies, where lower hemoglobin perfusate levels have been linked to a higher incidence of early allograft dysfunction, as well as juvenile porcine models of DCD heart perfusion, which showed suboptimal heart recovery and impaired function under low-hemoglobin conditions.10, 11 Furthermore, these findings could influence transplant protocols by potentially reducing the duration of blood collection, which adds to the WIT and the risk of introducing external toxins. Previous studies have demonstrated the benefits of minimizing WIT on graft health and survival.12, 13
Emerging evidence from other organ perfusion studies, such as in lungs and kidneys, suggests that acellular perfusates may reduce proinflammatory signaling while maintaining organ viability.14, 15, 16 Although cellular perfusates may afford increased length of preservation, their role in increasing graft injury warrants further investigation.17, 18, 19 Thus, an important factor to consider is the anticipated length of time the organ will be perfused when selecting a perfusate composition.
Limitations of this study include its retrospective single-center, which limits generalizability and the ability to establish strong causality. The relatively small sample size may have reduced statistical power. Moreover, the study may not have accounted for all potential confounding variables, such as variations in surgical techniques and postoperative management. For instance, variability in additional procedural data such as coronary flow rates, rate of adenosine infusion may influence outcomes and should be evaluated in further studies. Additionally, there is the technological limitation of classifying HCT values to either ≥15% PCV or <15% PCV based on i-STAT analysis reports because of nonspecific measurements for HCT values <15% PCV. Furthermore, echocardiographic and detailed hemodynamic parameters at 48 hours were not consistently collected in this cohort. The absence of these data limits physiologic interpretation and represents an important area for future prospective studies. Thus, while these results provide preliminary insights into the impact of perfusate HCT on postoperative transplant outcomes, this study is primarily hypothesis-generating and would necessitate larger prospective studies needed to establish causality and inform clinical guidelines.
Conclusion
Higher perfusate HCT level during ex vivo perfusion of DCD hearts does not appear to protect against PGD or ECMO utilization post transplant but may be associated with higher inotrope requirements and longer ICU stays. These findings raise important questions about optimal HCT levels for ex vivo perfusion and further exploration of perfusate composition for DCD heart transplantation.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cho P.D.Kim S.T.Zappacosta H.Severe primary graft dysfunction in heart transplant recipients using donor hearts after circulatory death: United States experience J Heart Lung Transplant 4420257607693961311910.1016/j.healun.2024.11.027 · doi ↗ · pubmed ↗
- 2Jolliffe J.Brookes J.Williams M.Donation after circulatory death transplantation: a systematic review and meta-analysis of outcomes and methods of donation Ann Cardiothorac Surg 14202511273994450610.21037/acs-2024-dcd-0132 PMC 11811570 · doi ↗ · pubmed ↗
- 3Pinnelas R.Kobashigawa J.A.Ex vivo normothermic perfusion in heart transplantation: a review of the Trans Medics(®) Organ Care System Future Cardiol 1820225153450334410.2217/fca-2021-0030 · doi ↗ · pubmed ↗
- 4D’Alessandro D.A.Wolfe S.B.Osho A.A.Hemodynamic and clinical performance of hearts donated after circulatory death J Am Coll Cardiol 802022131413263617505010.1016/j.jacc.2022.07.024 · doi ↗ · pubmed ↗
- 5Kobashigawa J.Zuckermann A.Macdonald P.Report from a consensus conference on primary graft dysfunction after cardiac transplantation J Heart Lung Transplant 3320143273402466145110.1016/j.healun.2014.02.027 · doi ↗ · pubmed ↗
- 6Delong C.Sharma S.Physiology, peripheral vascular resistance Stat Pearls 2024 Stat Pearls Publishing Treasure Island (FL)30855892 · pubmed ↗
- 7Piety N.Z.Reinhart W.H.Stutz J.Shevkoplyas S.S.Optimal hematocrit in an artificial microvascular network Transfusion 572017225722662868148210.1111/trf.14213 PMC 5583001 · doi ↗ · pubmed ↗
- 8Frimat M.Boudhabhay I.Roumenina L.T.Hemolysis derived products toxicity and endothelium: model of the second hit Toxins 1120196603176615510.3390/toxins 11110660 PMC 6891750 · doi ↗ · pubmed ↗