Prognostic implications of N-terminal pro–B-type natriuretic peptide in patients undergoing transcatheter aortic valve implantation
Nadia Salerno, Isabella Leo, Giovanni Canino, Antonio Bellantoni, Assunta Di Costanzo, Francesco Comito, Giuseppe Antonio Mazza, Giuseppe Panuccio, Salvatore Giordano, Salvatore De Rosa, Daniele Torella, Sabato Sorrentino

TL;DR
This study shows that N-terminal pro–B-type natriuretic peptide levels are strong predictors of poor outcomes in patients after a heart valve procedure called TAVI.
Contribution
The study introduces age-specific thresholds for NT-proBNP to assess long-term outcomes after TAVI and highlights the value of serial measurements.
Findings
Elevated baseline NT-proBNP predicted higher risk of mortality and heart failure rehospitalization after TAVI.
Patients with persistently high NT-proBNP levels had the worst outcomes compared to those with low levels.
Serial NT-proBNP measurements added prognostic value and could guide post-TAVI management.
Abstract
N-terminal pro–B-type natriuretic peptide (NT-proBNP) is a recognized marker of myocardial wall stress, but its prognostic role in patients undergoing transcatheter aortic valve implantation (TAVI) remains incompletely defined. This study assessed whether NT-proBNP levels at admission and discharge – interpreted using age-specific guideline thresholds – are associated with long-term clinical outcomes post-TAVI. We retrospectively analysed 683 consecutive patients who underwent successful TAVI at Magna Graecia University between 2009 and 2023. NT-proBNP was measured at both admission and discharge. Patients were stratified into low or high NT-proBNP groups based on age-adjusted cutoffs. Among 468 patients with paired measurements, four NT-proBNP trajectory groups were identified: Low–Low, Low–High, High–Low, and High–High. The primary endpoint was a composite of all-cause mortality or…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
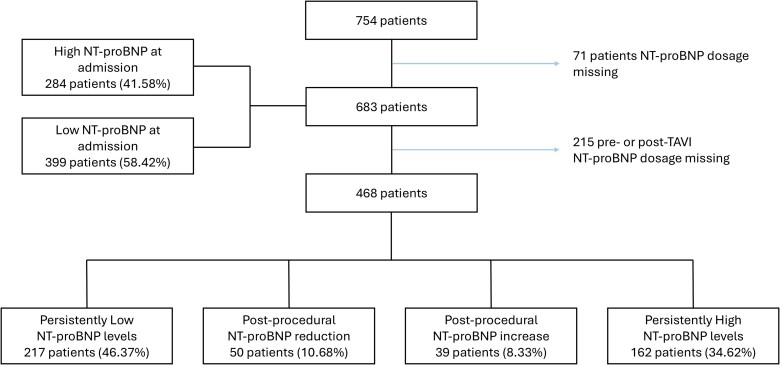 Figure 1
Figure 1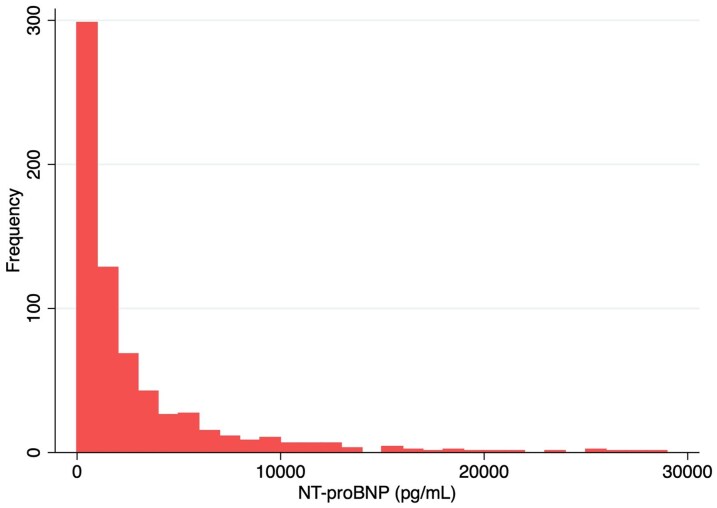 Figure 2
Figure 2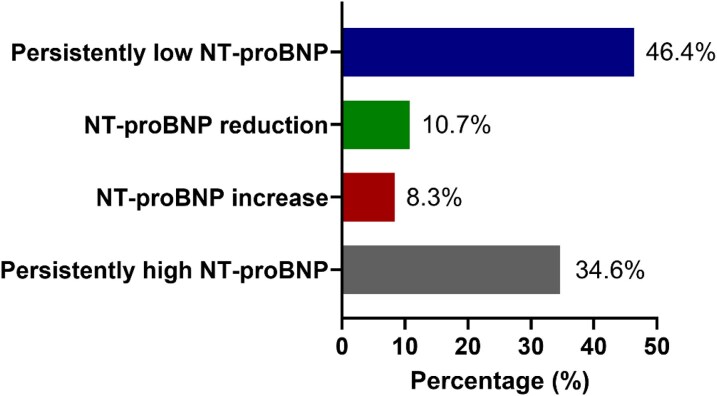 Figure 3
Figure 3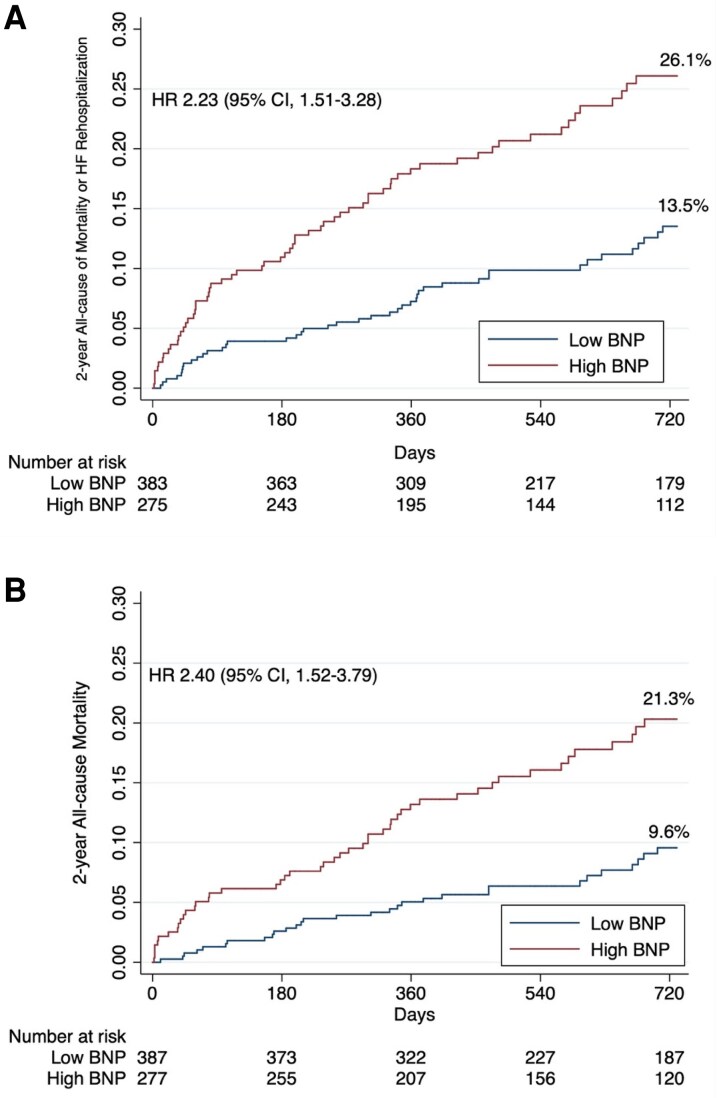 Figure 4
Figure 4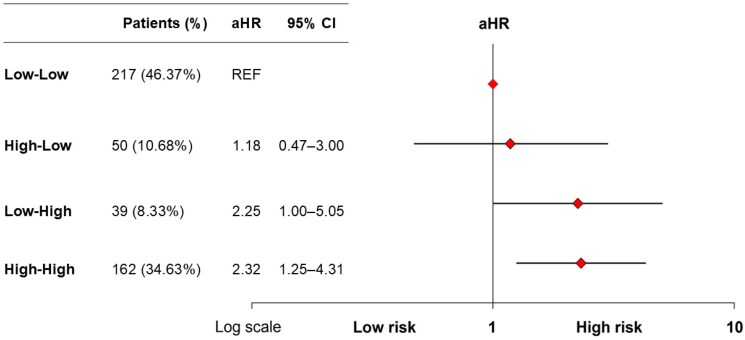 Figure 5
Figure 5| Variables | Low NT-proBNP | High NT-proBNP |
|
|---|---|---|---|
| Age | 80.12 ± 5.30 | 80.14 ± 6.36 | 0.52 |
| Female sex | 221 (55.39) | 156 (54.93) | 0.95 |
| BMI, kg/m² | 28.13 ± 4.77 | 26.90 ± 4.65 | <0.001 |
| BSA, m² | 1.80 ± 0.18 | 1.76 ± 0.20 | 0.005 |
| NYHA Class III/IV | 247 (76.47) | 218 (90.08) | <0.001 |
| Euroscore II | 4.45 ± 4.10 | 5.98 ± 5.07 | <0.001 |
| Hypertension | 376 (94.24) | 255 (89.79) | 0.03 |
| Dyslipidaemia | 290 (72.68) | 170 (59.86) | <0.001 |
| Diabetes Mellitus type 2 | 140 (35.09) | 105 (36.97) | 0.61 |
| Smoking history | 86 (21.61) | 45 (15.85) | 0.06 |
| Prior cerebrovascular event | 36 (9.02) | 24 (8.45) | 0.80 |
| Prior Valvular Surgery | 16 (3.91) | 12 (4.38) | 0.67 |
| Prior PCI | 85 (21.30) | 62 (21.83) | 0.87 |
| Chronic kidney disease | 81 (19.80) | 100 (36.50) | <0.001 |
| Severe Chronic kidney disease | 11 (2.78) | 62 (22.06) | <0.001 |
| Atrial Fibrillation | 69 (17.29) | 99 (34.86) | <0.001 |
| Prior pacemaker implantation | 28 (7.02) | 26 (9.15) | 0.31 |
| Peripheral artery disease | 60 (15.04) | 33 (11.62) | 0.20 |
| COPD | 88 (22.06) | 60 (21.13) | 0.77 |
| Haemoglobin, g/dL | 12.44 (1.60) | 11.90 (1.68) | <0.001 |
| Creatinine, mg/dL | 1.04 (0.55) | 1.56 (1.51) | <0.001 |
| Platelets, 10³/μL | 216 (71.54) | 203 (70.78) | 0.01 |
|
| |||
| LVEF | 54.96 ± 5.27 | 48.15 ± 9.37 | <0.001 |
| LVEF < 50% | 60 (15.04) | 153 (53.87) | <0.001 |
| Mean Gradient, mmHg | 46.40 ± 11.80 | 51.35± 16.01 | <0.001 |
| Peak Gradient, mmHg | 72.15± 19.52 | 75.70± 26.45 | 0.03 |
| Aortic Valve area baseline, cm2 | 0.77 ± 0.15 | 0.67 ± 0.18 | <0.001 |
| PAPS, mmHg | 37.85 ± 8.91 | 44.34 ± 12.66 | <0.001 |
| TAPSE, mm | 22.74 ± 2.68 | 21.32 ± 3.54 | <0.001 |
| Moderate or Severe MR | 24 (6.02) | 50 (17.73) | <0.001 |
| Moderate or Severe TR | 19 (4.76) | 29 (10.39) | 0.005 |
| Moderate or Severe AR | 19 (4.76) | 29 (10.39) | 0.005 |
| Age category | Guideline-recommended | Patients with elevated | NT-proBNP concentration pg/mL (mean; IQR) |
|---|---|---|---|
| Age < 50 years | 450 pg/mL | – | – |
| Age 50–74 years | 900 pg/mL | 51 (17.96%) | 879.00 (430.00–3385.00) |
| Age ≥ 75 years | 1800 pg/mL | 233 (82.04%) | 1281.50 (534.00–3457.00) |
| Variables | Low NT-proBNP | High NT-proBNP |
|
|---|---|---|---|
| CCU Stay, h | 65.41 ± 48.94 | 83.80 ± 95.98 | <0.001 |
| Fluoro Time, min | 21.81 ± 10.61 | 23.26 ± 12.27 | 0.07 |
| Valve in valve | 10 (2.51) | 9 (3.17) | 0.60 |
| Self-expandable valve | 284 (71.18) | 220 (77.46) | 0.07 |
| Death IH | 4 (1.00) | 8 (2.82) | 0.08 |
| Major bleeding | 44 (11.06) | 37 (13.03) | 0.43 |
| Minor bleeding | 32 (9.94) | 34 (13.99) | 0.14 |
| Pacemaker implantation | |||
| PM | 69 (17.34) | 55 (19.37) | 0.08 |
| ICD | 3 (0.75) | 8 (2.82) | 0.08 |
| New onset AF | 30 (7.52) | 26 (9.15) | 0.44 |
|
| |||
| Aspirin | 278 (70.03) | 166 (58.66) | 0.002 |
| P2Y12 inhibitor | 230 (57.93) | 160 (56.54) | 0.72 |
| Anticoagulants | 105 (26.32) | 118 (41.55) | <0.001 |
| Beta blockers | 265 (67.26) | 189 (68.23) | 0.79 |
| Calcium Blocker | 68 (17.26) | 55 (19.86) | 0.39 |
| ACE-I | 169 (42.89) | 127 (46.01) | 0.42 |
| ARBS | 194 (49.24) | 88 (31.88) | <0.001 |
| MRA | 44 (11.17) | 85 (30.80) | <0.001 |
| Diuretics | 296 (75.51) | 240 (86.96) | <0.001 |
| ARNI | 6 (1.55) | 10 (3.72) | <0.001 |
|
| |||
| LVEF | 54.59 ± 5.41 | 48.51 ± 9.00 | <0.001 |
| Mean gradient post | 10.10 ± 4.89 | 10.58 ± 6.02 | 0.12 |
| Aortic Regurgitation 2–3+ | 19 (4.76) | 29 (10.39) | 0.005 |
| PAPS, mmHg | 37.07 ± 8.70 | 41.06 ± 10.41 | <0.001 |
| TAPSE, mm | 22.93 ± 2.49 | 21.99 ± 3.30 | <0.001 |
| Variable | Hazard ratio | 95% confidence interval |
|
|---|---|---|---|
| High NT-proBNP at admission | 1.85 | 1.18–2.88 | 0.007 |
| Female sex | 1.30 | 0.85–2.00 | 0.231 |
| BMI (per unit) | 0.99 | 0.95–1.04 | 0.802 |
| Anaemia | 1.31 | 0.88–1.96 | 0.185 |
| Smoking | 1.73 | 1.05–2.84 | 0.030 |
| Baseline LVEF (per %) | 0.99 | 0.96–1.01 | 0.239 |
| COPD | 1.65 | 1.07–2.55 | 0.023 |
| Dyslipidaemia | 0.72 | 0.48–1.07 | 0.104 |
| Atrial Fibrillation | 1.45 | 0.96–2.21 | 0.078 |
| Chronic Kidney Disease | 0.99 | 0.64–1.52 | 0.949 |
| Variable | Hazard ratio | 95% confidence interval |
|
|---|---|---|---|
| Post-procedural NT-proBNP reduction | 1.18 | 0.47–3.00 | 0.723 |
| Post-procedural NT-proBNP increase | 2.25 | 1.00–5.05 | 0.049 |
| Persistently high NT-proBNP levels | 2.32 | 1.25–4.31 | 0.008 |
| Female sex | 1.02 | 0.64–1.63 | 0.941 |
| BMI (per unit) | 1.00 | 0.95–1.05 | 0.930 |
| Anaemia | 1.45 | 0.89–2.37 | 0.134 |
| Baseline LVEF (per %) | 0.99 | 0.96–1.02 | 0.513 |
| COPD | 2.27 | 1.40–3.67 | 0.001 |
| Dyslipidaemia | 0.73 | 0.46–1.16 | 0.181 |
| Atrial Fibrillation | 1.33 | 0.82–2.16 | 0.250 |
| Chronic Kidney Disease | 0.90 | 0.54–1.48 | 0.675 |
- —Italian Ministry of Health10.13039/501100003196
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Heart Failure Treatment and Management · Atrial Fibrillation Management and Outcomes
Introduction
Transcatheter aortic valve implantation (TAVI) has become the standard of care for patients with severe symptomatic aortic stenosis (AS), with its indications now extended across the entire spectrum of surgical risk.^1^ Despite these advances, substantial variability remains in both the timing of intervention and postprocedural outcomes, underscoring the need for robust tools to guide clinical decision-making throughout the care continuum.^2^
In this context, biomarkers capable of identifying patients at increased long-term risk may enhance follow-up strategies and inform therapeutic decisions.^3^ Among the most promising, N-terminal pro–B-type natriuretic peptide (NT-proBNP) is a well-established marker of myocardial wall stress and is widely used for both the diagnosis and prognostication of heart failure (HF).^4^ In AS, elevated NT-proBNP levels have been associated with symptom onset, disease severity, and adverse outcomes. Importantly, higher preprocedural NT-proBNP values have also been linked to increased mortality and HF-related rehospitalization following TAVI.^5–8^ Nevertheless, the optimal timing of measurement, appropriate threshold values, and the prognostic significance of both baseline levels and dynamic changes in NT-proBNP remain inadequately defined.
Recent European Society of Cardiology (ESC)-endorsed consensus statements have proposed age-adjusted NT-proBNP thresholds for the diagnosis of acute HF (≥450 pg/mL for patients <50 years, ≥900 pg/mL for those aged 50–75 years, and ≥1800pg/mL for those >75 years), demonstrating strong diagnostic accuracy in emergency settings. However, whether these thresholds can be extrapolated to risk stratification in the TAVI population has yet to be validated.^4^
In this study, we aimed to evaluate the prognostic value of NT-proBNP levels measured both before and after TAVI in a large real-world cohort, applying age-specific thresholds derived from current guidelines and expert consensus. This approach is intended to clarify the longitudinal prognostic utility of NT-proBNP in TAVI recipients and to support the integration of biomarker-guided strategies into routine postprocedural management.
Methods
Study population
Consecutive patients who underwent successful TAVI between September 2009 and December 2023 at the Cardiology Department of Magna Graecia University were retrospectively included in a pre-specified institutional dataset. All clinical data were collected from electronic medical records and anonymized before analysis. The study was conducted in accordance with the principles of the Declaration of Helsinki and approved by the local institutional review board.
Study protocol and definitions
All procedures were performed according to standard clinical practice. Both balloon-expandable and self-expandable valves were used. The transfemoral approach was predominantly adopted, with percutaneous access and the use of a pre-closure technique.^9^ Prosthesis sizing was based on pre-procedural computed tomography. Rapid right ventricular pacing was routinely applied during balloon dilation for native or bioprosthetic valve deployment. Anaemia was defined per WHO sex-specific thresholds (Hb <13.0 g/dL men; <12.0 g/dL women); severity categories were mild 11.0–12.9/11.0–11.9 g/dL, moderate 8.0–10.9 g/dL, severe <8.0 g/dL. NT-proBNP levels were measured at admission and at discharge. NT-proBNP was quantified using the cobas h 232 NT-proBNP (Plus) assay (Roche Diagnostics); results are reported in pg/mL, with a uniform platform used across the study period. Clinical follow-up assessments were scheduled at 1 month, 6 months, and 2 years post-procedure. Decompensated heart failure was defined according to consensus-based, age-adjusted NT-proBNP thresholds: ≥450 pg/mL for patients <50 years, ≥900 pg/mL for those aged 50–75 years, and ≥1800pg/mL for patients >75 years.^4^ Patients with values above these thresholds were classified as having elevated NT-proBNP levels. Additionally, patients were categorized into four NT-proBNP trajectory groups based on pre- and post-procedural values using the guideline-recommended cutoffs previously reported: (1) Low–Low: NT-proBNP below threshold at both admission and discharge; (2) Low–High: NT-proBNP below threshold at admission, but above threshold at discharge; (3) High–Low: NT-proBNP above threshold at admission, but below threshold at discharge; (4) High–High: NT-proBNP above threshold at both time points. To assess potential selection from missing trajectories, we compared baseline characteristics of patients with vs. without serial NT-proBNP. The primary outcome measure was a composite of all-cause mortality or HF rehospitalization at 2 years of follow-up. Secondary outcomes were all-cause mortality at 2 years of follow-up and in-hospital bleeding, pacemaker implantation, and new-onset atrial fibrillation. All the outcomes were defined according to the Valve Academic Research Consortium 3 consensus.
Statistical analysis
Continuous variables were expressed as mean ± standard deviation and compared using Student’s t-test. Categorical variables were expressed as frequencies and percentages and compared between groups using the chi-squared test. Event rates were estimated using the Kaplan–Meier method and compared with the log-rank test. The primary endpoint was analysed using multivariable Cox proportional hazards regression to estimate the adjusted risk of death or HF rehospitalization associated with elevated NT-proBNP levels, as previously defined. Covariates included in the multivariable model were selected based on baseline imbalances and established prognostic relevance in the literature. For sensitivity, we repeated the Cox analyses within atrial fibrillation (AF) strata and by procedural period – early (2009–2016) vs. contemporary (2017–2023). Within each stratum, we ran (i) a univariable Cox with high NT-proBNP at admission as the exposure and (ii) a multivariable Cox model. We also fit a unified model with an NT-proBNP × period interaction. As an additional sensitivity analysis, we built a parsimonious model that included EuroSCORE II (entered per 1% absolute risk) together with NT-proBNP, AF, BMI, anaemia, smoking, and dyslipidaemia. The discriminative performance of the Cox regression models was assessed using Harrell’s concordance statistic (C-statistic), which quantifies the model’s ability to correctly rank the survival times of patients. A C-statistic value of 0.5 indicates no discriminative power, while a value of 1.0 indicates perfect discrimination.
Statistical analyses were performed using Stata version 12.1 (StataCorp, College Station, TX, USA). A two-tailed P-value <0.05 was considered statistically significant.
Results
Baseline and echocardiographic characteristics
A total of 683 patients with severe AS undergoing TAVI were included in the analysis (Figure 1 and Supplementary material online, Table S1). Among them, 284 patients (41.6%) presented with elevated NT-proBNP levels at admission, as defined by prespecified age-adjusted thresholds. Baseline characteristics stratified by NT-proBNP levels are summarized in Table 1.
Study flow chart.
There were no significant differences between the two groups in terms of age, sex, diabetes, or prior cardiovascular interventions. However, patients with elevated NT-proBNP levels exhibited significantly lower body mass index (BMI) and body surface area (BSA), and more frequently presented with NYHA class III–IV symptoms (P < 0.01). The high NT-proBNP group also had a significantly greater prevalence of chronic kidney disease (CKD), and atrial fibrillation (AF) (P < 0.001 for all).
Echocardiographic assessment revealed worse baseline cardiac morphology and function in the high NT-proBNP group, including lower left ventricular ejection fraction (LVEF), smaller aortic valve area, higher transvalvular gradients, elevated pulmonary artery pressures (PAPs), and a higher prevalence of both right and left valvular dysfunction (P < 0.01 for all comparisons). Laboratory evaluation showed significantly lower haemoglobin and platelet counts, and higher serum creatinine concentrations in patients with elevated NT-proBNP levels (P < 0.01 for all).
Preprocedural and postprocedural NT-proBNP distribution
- illustrated the distribution of NT-proBNP levels at admission. The median NT-proBNP level was 1219 pg/mL (IQR: 513–3457 pg/mL), while the mean was substantially higher at 3391 pg/mL due to the influence of outliers.
NT-proBNP distribution at admission.
Based on guideline-recommended age-adjusted thresholds (Table 2), 51 patients (17.96%) aged 50–74 years and 233 patients (82.04%) aged ≥75 years had elevated NT-proBNP levels at baseline. Among the 683 patients included, discharge NT-proBNP measurements were available for 468 individuals. Clinical and procedural characteristics of patients without available NT-proBNP trajectories are presented in Supplementary material online, Table S2 and did not substantially differ from those of the remaining study population. Of these, 217 patients (46.4%) exhibited persistently low NT-proBNP levels, 50 (10.7%) showed a postprocedural reduction, 39 (8.3%) had a postprocedural increase, and 162 (34.6%) had persistently elevated NT-proBNP levels (Figure 3).
Distribution of NT-proBNP patterns.
Procedural and clinical outcomes
Procedural characteristics and in-hospital outcomes stratified by NT-proBNP levels are reported in Table 3. Patients with elevated NT-proBNP at admission experienced significantly longer lengths of stay in the Coronary Care Unit (CCU) compared to those with low levels (P < 0.001). No significant differences were observed in procedural characteristics or the incidence of periprocedural complications.
Postprocedural echocardiographic evaluations demonstrated that patients in the high NT-proBNP group continued to have significantly lower LVEF, higher PAPs, and reduced TAPSE (P < 0.001 for all). Moderate-to-severe postprocedural aortic regurgitation was more frequent in this group (P = 0.005), while mean transvalvular gradients were comparable between groups (P = 0.12).
Over a 2-year follow-up, patients with elevated NT-proBNP levels at baseline experienced a significantly higher incidence of the composite endpoint of all-cause mortality or HF rehospitalization compared to those with low baseline levels (26.1% vs. 13.7%; HR 2.23, 95% CI 1.51–3.28; Figure 4A). Similarly, all-cause mortality alone was higher in the high NT-proBNP group (21.3% vs. 9.6%; HR 2.40, 95% CI 1.52–3.79; Figure 4B). The predictive performance of NT-proBNP for these outcomes was modest, with C-statistics of 0.613 and 0.606, respectively. Importantly, elevated preprocedural NT-proBNP remained an independent predictor of the primary outcome after multivariable adjustment (HR 1.85; 95% CI 1.18–2.88; P = 0.007; Table 4). Sensitivity analyses confirmed prognostic value across AF status and implantation period, with no significant interactions (see Supplementary material online, Table S3, Panel A-B). In an additional model incorporating EuroSCORE II as a global surgical-risk measure, high NT-proBNP at admission remained independently associated with the 2-year endpoint (HR 1.88, 95% CI 1.22–2.89; P = 0.004) (see Supplementary material online, Table S4).
(A) Risk of all-cause mortality and HF rehospitalization at 2 years of follow-up according to NT-proBNP levels at admission based on guideline-recommended cutoffs. (B) Risk of all-cause mortality at 2 years of follow-up according to NT-proBNP levels at admission based on guideline-recommended cutoffs.
Finally, compared to patients with persistently low NT-proBNP levels, no significant difference in the primary outcome was observed in those who exhibited a postprocedural reduction in NT-proBNP (aHR 1.18; 95% CI 0.47–3.00), while those with postprocedural NT-proBNP elevation (aHR 2.25; 95% CI 1.00–5.05) and those with persistently high levels (aHR 2.32; 95% CI 1.25–4.31) had significantly greater risk (Figure 5), based on models adjusted for sex, BMI, anaemia, LVEF, COPD, dyslipidaemia, atrial fibrillation, and chronic kidney disease (Table 5). Results were consistent when EuroSCORE II was incorporated into the multivariable Cox model, with persistently high and increasing NT-proBNP trajectories remaining significantly associated with adverse outcomes, in line with the findings of the main analysis (see Supplementary material online, Table S5).
Risk of 2-year mortality or HF rehospitalization according to periprocedural NT-proBNP trajectories.
Discussion
In this retrospective cohort of nearly 700 patients undergoing TAVI, we evaluated the prognostic utility of NT-proBNP levels measured both before and after the procedure. The main findings emanating from our study are as follows: (i) Preprocedural NT-proBNP levels exhibited a markedly right-skewed distribution, reflecting substantial heterogeneity in disease severity and systemic stress; (ii) Approximately 50% of patients exceeded the age-specific thresholds recommended by ESC consensus statements for the diagnosis of acute decompensated heart failure (HF); (iii) Elevated baseline NT-proBNP levels were independently associated with a two-fold increase in the risk of all-cause mortality or HF rehospitalization at 2 years; (iv) Age-adjusted, consensus-based cutoffs showed fair discriminative capacity for predicting long-term adverse outcomes; and (v) Persistently elevated or rising NT-proBNP levels post-TAVI identified patients at particularly high risk, whereas a postprocedural reduction in NT-proBNP was associated with improved prognosis.
NT-proBNP is a well-established biomarker for risk stratification in patients with AS, with prognostic value in both symptomatic and asymptomatic stages.^10^ It has been increasingly incorporated into longitudinal surveillance strategies aimed at detecting early signs of disease progression and decompensation.^11^ Notably, in the multicentre, randomized EARLY TAVR trial, NT-proBNP was used as part of a predefined algorithm to trigger early intervention. Specifically, a threefold rise from baseline – alongside an absolute NT-proBNP value >375 pg/mL in patients ≤75 years or >1350 pg/mL in those >75 years – was used to prompt aortic valve replacement. Importantly, nearly 40% of patients in the surveillance arm developed overt symptoms during follow-up, highlighting the limitations of symptom-based monitoring alone.^12^
Despite these promising applications, the broader integration of NT-proBNP into clinical decision-making remains hindered by the absence of standardized protocols regarding its timing, interpretation, and role across different disease stages. For instance, the 2021 ESC Guidelines for Valvular Heart Disease recommend natriuretic peptide measurement only in select asymptomatic patients with preserved ejection fraction – underscoring a conservative approach that positions NT-proBNP as a secondary, rather than primary, clinical tool.^1^
Nevertheless, consistent evidence from large-scale observational studies supports its robust prognostic value. Medranda et al., for example, reported that baseline BNP levels ≥500 pg/mL were associated with a > 3-fold increased risk of stroke or death at 30 days post-TAVI.^7^ Similarly, Sørensen et al. demonstrated that NT-proBNP ≥420 pmol/L independently predicted a twofold higher risk of one-year HF hospitalization and all-cause mortality.^13^
The variation in NT-proBNP thresholds across studies reflects differences in population characteristics, assay platforms, and clinical context – diagnostic vs. prognostic.^14^ In our study, we minimized such variability by adopting the age-adjusted NT-proBNP cutoffs recommended by international consensus statements for acute HF diagnosis. These thresholds, originally derived from the ICON and ICON-RELOADED studies, have demonstrated consistent diagnostic accuracy across a range of clinical conditions and patient subgroups – irrespective of renal function, BMI, AF, or diabetes.^15,16^ Their application in our TAVI cohort yielded fair predictive value, reinforcing their broader potential in risk stratification beyond acute care settings.
Importantly, nearly half of our TAVI patients met the NT-proBNP criteria for acute HF despite being referred for elective intervention. This finding underscores the limitations of symptom-based referral pathways and suggests that a substantial proportion of high-risk patients may experience delays in treatment. Our results advocate for a more structured, biomarker-guided surveillance approach, particularly in elderly, frail, or minimally symptomatic individuals, in whom clinical evaluation may underestimate disease burden.
Beyond static measurements, our analysis also explored NT-proBNP trajectories surrounding the procedure. Patients who demonstrated postprocedural reductions – i.e. ‘biochemical responders’ – experienced significantly lower rates of death or HF rehospitalization. These findings align with those of Seoudy et al., who similarly reported improved outcomes in patients with declining NT-proBNP levels at discharge.^6^ Interestingly, while responders typically presented with more severe preprocedural haemodynamic compromise, non-responders exhibited a higher burden of comorbidities – suggesting distinct pathophysiologic substrates underlying differential NT-proBNP dynamics. Indeed, from a mechanistic standpoint, persistently elevated or rising NT-proBNP levels after TAVI likely reflect unresolved myocardial stress and maladaptive cardiac remodelling. Although relief of valvular obstruction by TAVI reduces left ventricular afterload, many patients – particularly those with long-standing pressure overload – may already exhibit irreversible structural changes, including myocardial fibrosis, impaired diastolic function, or reduced contractile reserve. These pathophysiologic alterations can blunt the haemodynamic benefits of valve replacement and sustain neurohormonal activation, thereby maintaining high natriuretic peptide levels.^17^ Comorbidities like AF, renal dysfunction, and pulmonary hypertension may further exacerbate myocardial load.^18,19^ In contrast, patients who exhibit postprocedural NT-proBNP decline may represent a subgroup with more favourable myocardial substrate and greater capacity for reverse remodeling.^5,6^
Taken together, these findings highlight the value of NT-proBNP not only as a static prognostic biomarker but also as a dynamic tool for postprocedural risk stratification. This may be particularly relevant in the context of emerging cardioprotective therapies – such as Sodium-glucose cotransporter-2 inhibitors (SGLT2i) and angiotensin receptor–neprilysin inhibitors (ARNI) – which have demonstrated benefits in selected high-risk populations.^20^ Early identification of such patients through NT-proBNP monitoring could enable the timely initiation of adjunctive medical therapy, ultimately improving long-term outcomes. This may be particularly relevant in light of the recently published DapaTAVI randomized trial, which demonstrated that dapagliflozin led to a 28% relative reduction in the composite endpoint of all-cause mortality or worsening HF, and a 37% reduction in HF events compared to standard care.^21^ Importantly, our patient cohort was enrolled before the availability of this evidence, highlighting a key opportunity for NT-proBNP–guided identification of high-risk individuals – such as those with persistently elevated levels – who may derive the greatest benefit from early initiation of SGLT2 inhibition. Such a strategy might have prevented HF progression and improved outcomes in our population.
Limitations
This study has several limitations that warrant consideration. First, it is a retrospective, single-centre analysis in a TAVI-treated cohort, which may limit the external validity of our findings and carries inherent risks of selection and information bias despite multivariable adjustment. The absence of a comparator group of asymptomatic or less-severe AS patients managed without AVR/TAVI prevents any inference on biomarker-guided timing of intervention, and subgroup sample sizes were relatively small, limiting statistical power. Second, NT-proBNP assessment was based on routine clinical care, with variability in timing and some missingness. We relied on a single predischarge measurement for feasibility, while alternative post-TAVI time points and serial sampling beyond discharge were not systematically collected. As a result, we cannot establish the optimal timing of NT-proBNP measurement, and the discharge landmark may have introduced survivor bias. Third, although multivariable models adjusted for key clinical covariates, residual confounding cannot be excluded. Baseline LVEF was imbalanced, with many patients <50%, which may confound the association between NT-proBNP and outcomes. We mitigated this by modelling LVEF as a continuous covariate in all multivariable analyses (avoiding arbitrary cutoffs), but residual confounding cannot be excluded, so findings are prognostic rather than causal. Additional unmeasured factors – including frailty, functional status, inflammatory markers, and comorbidity burden – were not captured, and although EuroSCORE II was incorporated as a replacement composite to mitigate double-counting, it only partially reflects frailty and reserve capacity. Fourth, this study was not designed or powered to compare NT-proBNP with other candidate biomarkers or multimarker panels. Alternative markers such as hs-troponin, sST2, GDF-15, or galectin-3 were not collected systematically, and the prognostic discrimination of NT-proBNP was modest. The question of the most effective biomarker for treatment-timing or management decisions, therefore, remains open and warrants prospective, head-to-head comparative studies with decision-analytic metrics. Finally, patient selection may have led to conservative bias. The exclusion of less decompensated patients – characterized by lower NT-proBNP levels, higher LVEF/TAPSE, and lower PAPs – would likely bias associations toward the null. In addition, STS score, formal frailty indices, and health-status measures were not systematically collected. Although we adjusted for EuroSCORE II – entered as a replacement composite to avoid double-counting – this score only partially captures frailty and functional reserve, so residual confounding may persist. Collectively, these limitations underscore that our results should be interpreted as associative and hypothesis-generating rather than causal, and future prospective studies are warranted to validate and extend these findings.
Conclusion
In this large, real-world cohort of patients undergoing TAVI, elevated NT-proBNP levels – defined according to age-specific ESC consensus thresholds – were independently associated with an increased risk of long-term mortality and HF rehospitalization. Patients with persistently elevated or rising NT-proBNP levels after TAVI experienced the poorest outcomes, whereas a postprocedural decline identified a subgroup with a more favourable prognosis. These findings support the role of NT-proBNP as a practical and informative biomarker for risk stratification both before and after TAVI. Integration of NT-proBNP monitoring into standardized clinical pathways may enhance patient selection, inform follow-up strategies, and guide timely initiation of emerging medical therapies aimed at improving post-TAVI outcomes.
Supplementary Material
oeaf169_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachs J, Capodanno D, Conradi L, De Bonis M, De Paulis R, Delgado V, Freemantle N, Gilard M, Haugaa KH, Jeppsson A, Jüni P, Pierard L, Prendergast BD, Sádaba JR, Tribouilloy C, Wojakowski W; ESC/EACTS Scientific Document Group. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J 2022;43:561–632.34453165 10.1093/eurheartj/ehab 395 · doi ↗ · pubmed ↗
- 2Auffret V, Ridard C, Salerno N, Sorrentino S. Unmet needs in TAVR: conduction disturbances and management of coronary artery disease. J Clin Med 2022;11:6256.36362484 10.3390/jcm 11216256 PMC 9658775 · doi ↗ · pubmed ↗
- 3Hecht S, Giuliani C, Nuche J, Farjat Pasos JI, Bernard J, Tastet L, Abu-Alhayja'a R, Beaudoin J, Côté N, De Larochellière R, Paradis J-M, Clavel M-A, Arsenault BJ, Rodés-Cabau J, Pibarot P. Multimarker approach to improve risk stratification of patients undergoing transcatheter aortic valve implantation. JACC Adv 2024;3:100761.38939373 10.1016/j.jacadv.2023.100761 PMC 11198363 · doi ↗ · pubmed ↗
- 4Bayes-Genis A, Docherty KF, Petrie MC, Januzzi JL, Mueller C, Anderson L, Bozkurt B, Butler J, Chioncel O, Cleland JGF, Christodorescu R, Del Prato S, Gustafsson F, Lam CSP, Moura B, Pop-Busui R, Seferovic P, Volterrani M, Vaduganathan M, Metra M, Rosano G. Practical algorithms for early diagnosis of heart failure and heart stress using NT-pro BNP: a clinical consensus statement from the Heart Failure Association of the ESC. Eur J Heart Fail 2023;25:1891–1898.37712339 10.100 · doi ↗ · pubmed ↗
- 5O’Leary JM, Clavel MA, Chen S, Goel K, O’Neill B, Elmariah S, Crowley A, Alu MC, Thourani VH, Leon MB, Pibarot P, Lindman BR. Association of natriuretic peptide levels after transcatheter aortic valve replacement with subsequent clinical outcomes. JAMA Cardiol 2020;5:1113–1123.32667623 10.1001/jamacardio.2020.2614 PMC 7364343 · doi ↗ · pubmed ↗
- 6Seoudy H, Frank J, Neu M, Güßefeld N, Klaus Y, Freitag-Wolf S, Lambers M, Lutter G, Dempfle A, Rangrez AY, Kuhn C, Frey N, Frank D. Periprocedural changes of NT-pro BNP are associated with survival after transcatheter aortic valve implantation. J Am Heart Assoc 2019;8:e 010876.30686097 10.1161/JAHA.118.010876 PMC 6405592 · doi ↗ · pubmed ↗
- 7Medranda GA, Salhab K, Schwartz R, Green SJ. Prognostic implications of baseline B-type natriuretic peptide in patients undergoing transcatheter aortic valve implantation. Am J Cardiol 2020;130:94–99.32665134 10.1016/j.amjcard.2020.06.017 · doi ↗ · pubmed ↗
- 8Mizutani K, Hara M, Iwata S, Murakami T, Shibata T, Yoshiyama M, Naganuma T, Yamanaka F, Higashimori A, Tada N, Takagi K, Araki M, Ueno H, Tabata M, Shirai S, Watanabe Y, Yamamoto M, Hayashida K. Elevation of B-type natriuretic peptide at discharge is associated with 2-year mortality after transcatheter aortic valve replacement in patients with severe aortic stenosis: insights from a multicenter prospective OCEAN-TAVI (optimized transcatheter valvular intervention–transcatheter · doi ↗ · pubmed ↗