Perceptions of faculty and medical students regarding an undergraduate research culture activity in Myanmar: a qualitative study
Htain Lin Aung, Moe Oo Thant, July Maung Maung, Ye Hlaing Oo, Thin Thin Toe, Hla Moe

TL;DR
This study examines how a research program at a Myanmar medical university is perceived by students and faculty, highlighting its benefits and challenges.
Contribution
The study provides insights into the effectiveness and challenges of an undergraduate research culture activity in a resource-limited setting.
Findings
Participants gained improved understanding of scientific literature and practical research skills.
Challenges included limited research preparedness, scheduling conflicts, and weak coordination with clinicians.
Suggestions for improvement include clearer guidelines, pre-research training, and stronger supervision.
Abstract
This study explored the perceptions of faculty members and third-year medical students regarding the research culture activity (RCA), a program designed to engage undergraduates in research at the University of Medicine, Mandalay, Myanmar. It aimed to identify the knowledge, attitudes, and skills (KAS) gained, the challenges encountered, and suggestions for improvement. This qualitative study employed 4 semi-structured focus group discussions with 17 third-year medical students and 16 faculty members who participated in the 2020 RCA. Student responses related to KAS were analyzed using a deductive framework approach, while challenges and suggestions were examined through inductive thematic analysis. Discussions were audio-recorded, transcribed verbatim in Burmese, translated into English, and collaboratively coded using Atlas.ti version 9.0.5. Participants reported improved…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
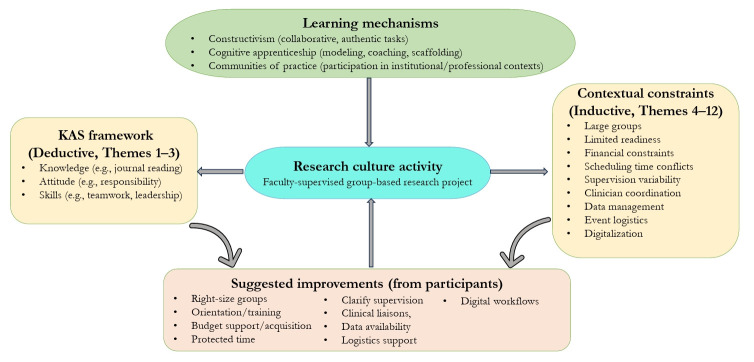 Figure 1
Figure 1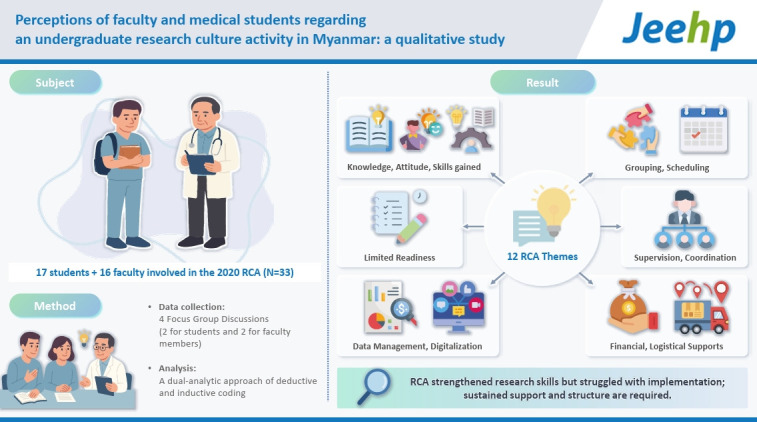 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealth and Medical Research Impacts · Innovations in Medical Education
Graphical abstract
Introduction
Background/rationale
Research training in undergraduate medical education strengthens evidence-based practice, critical thinking, and professional development. Globally, research exposure is increasingly integrated into medical curricula to promote academic literacy and interest in research careers [1-3]. However, in Myanmar, a resource-limited country in Southeast Asia, undergraduate research remains underdeveloped, with limited institutional capacity and insufficient faculty preparedness. The University of Medicine, Mandalay (UMM) launched the research culture activity (RCA) in 2015 for third-year (paraclinical) undergraduate medical students. The RCA is a cohort-wide, compulsory, faculty-supervised, group-based project embedded in the third-year paraclinical phase. It is implemented as a 2-month block (typically November–December) within the academic timetable. Mentored student teams select or are assigned feasible topics aligned with departmental priorities, conduct basic retrospective or cross-sectional data analyses, and prepare a poster or short paper for a program-wide presentation day featuring formative feedback. Operational details (cohort size, grouping, supervisor allocation, and outputs) are summarized in Supplement 1. This initiative is briefly described in the 2019 program guidebook of Myanmar’s outcome-based integrated Bachelor of Medicine and Bachelor of Surgery (MBBS) curriculum, particularly in the vertical module titled “Research culture and skill” [4]. The RCA’s supervised, group-based structure reflects principles of social constructivism, in which students co-construct knowledge through authentic tasks and guided participation [5]. Supervisory roles parallel cognitive apprenticeship models—modeling, coaching, and scaffolding—that make expert reasoning visible [6]. These theoretical perspectives informed our analytic focus on both learning outcomes and implementation challenges. Despite its positive intentions, several challenges were reported anecdotally by faculty and students during the early years of RCA implementation, yet these had not been systematically studied or documented. This study therefore aimed to explore these perceptions in a structured manner. Understanding how such programs are perceived can inform the development of more effective undergraduate research initiatives in low-resource medical education settings. To our knowledge, this is the first systematic evaluation of an undergraduate research initiative in Myanmar.
Objectives
This study aimed to explore the perceptions of students and faculty regarding the RCA, focusing on: (1) knowledge, attitudes, and skills (KAS) gained; (2) challenges encountered; (3) strategies to address these challenges; and (4) suggestions for improving RCA implementation.
Methods
Ethics statement
Ethical approval was obtained from the Ethics Review Committee of the University of Medicine, Mandalay (ID no., 342/ME/UMM/2020). Written informed consent, including permission for audio recording, was obtained from all participants after they were informed of the study’s aims, minimal risks, rights (voluntary participation, option to skip questions, and the ability to withdraw before anonymization), and the intended use of data (scholarly publication only).
Personal characteristics of the research team
The facilitators, H.L.A. and M.O.T.—senior faculty members with prior qualitative research training—conducted the focus group discussions (FGDs) with faculty and students. They were not involved in RCA supervision or the teaching of third-year students. Transcription in Burmese (by H.L.A. and M.O.T.) and translation into English (by Y.H.O.) were reviewed by bilingual researchers (J.L.M.M., T.T.T., H.M.). All 6 researchers held MBBS degrees and at least 1 master’s degree; H.M. also held a PhD (Doctor of Philosophy). The team comprised 5 males and 1 female. H.L.A., T.T.T., and H.M. had international training in medical education; H.L.A., M.O.T., and J.L.M.M. were experienced qualitative researchers; and Y.H.O., a certified pathologist, was also an accredited English-language expert.
Relationship with participants
No pre-existing supervisory relationships existed between the facilitators and the participants.
Theoretical framework and methodology
This qualitative study followed a constructivist approach [5], emphasizing the centrality of participant experiences in generating meaning. In addition to constructivism, the study drew upon cognitive apprenticeship theory [6] to interpret supervisory roles (modeling, coaching, scaffolding) and situated learning/communities of practice theory [7] to situate the RCA within its institutional and clinical environment. These frameworks informed both data collection and interpretation. A deductive framework was used to analyze student responses related to KAS, while inductive thematic analysis was applied to explore broader themes related to challenges and suggestions [8,9].
Participant selection
Because the RCA was implemented only for third-year students in 2020, purposive sampling was used to include the entire cohort and their supervising faculty as the most relevant participants for the study. A total of 33 individuals participated: 17 third-year medical students (2019–2020 academic year) who took part in the RCA 2020, and 16 faculty members from the Departments of Pathology, Pharmacology, and Microbiology who supervised the same cohort (Table 1). Students were selected across the 3 subject areas and participated in both poster and paper presentations. Faculty participants held various academic ranks, including demonstrator, assistant lecturer, lecturer, and associate professor. There were no refusals or dropouts.
Setting and context
All 4 FGDs were conducted at the Department of Medical Education’s meeting room at UMM during August and September 2020. Only researchers and participants were present during each session. The setting was private, easily accessible, and conducive to open discussion.
Data collection
The research team developed a semi-structured interview guide (Supplement 2), which was pilot tested. Each FGD lasted between 60 and 90 minutes. All sessions were audio recorded, and researchers took concurrent field notes. Two researchers (H.L.A. and M.O.T.) transcribed the recordings verbatim in Burmese, which were subsequently translated into English by co-author (Y.H.O.). The transcripts and translations were cross-checked for accuracy by co-authors (J.L.M.M., T.T.T., and H.M.). Data saturation was achieved after the fourth FGD (Dataset 1).
Data analysis
Three researchers (H.L.A., M.O.T., J.L.M.M.) independently coded the translated transcripts. A dual-analytic approach was employed. For student responses related to KAS, a deductive framework approach was used to organize data into 3 predefined categories: knowledge, attitude, and skills. Within each category, subcodes were developed inductively based on participants’ responses. For the remaining open-ended questions addressing challenges, coping strategies, and suggestions, inductive thematic analysis was conducted following the 6-phase framework by Braun and Clarke [9]. Coding and theme generation were performed manually and supported by Atlas.ti ver. 9.0.5 (MacOS and Windows; https://atlasti.com/). The coding framework was refined collaboratively through consensus meetings, supported by analytic memoing to document coding decisions and track the evolution of codes and themes, thereby creating an audit trail. This process enhanced transparency and reproducibility. Although participants did not review the coded transcripts or findings, credibility was strengthened through triangulation across multiple coders and data sources. Two additional researchers (T.T.T. and H.M.) independently reviewed the coded outputs and finalized the thematic structure through consensus.
Results
A total of 12 themes were identified from the focus group discussions with faculty and students. These were categorized into 2 overarching domains: (1) KAS gained from student groups (3 themes) (Table 2), and (2) challenges, coping strategies, and suggestions for improvement (9 themes). Themes emerged consistently across student and faculty groups, with several areas of concordance and complementary perspectives. Illustrative quotations for each theme are presented in Table 3 and extended quotations in Supplement 3. The narrative below focuses on thematic synthesis across domains.
Knowledge, attitudes, and skills gained
Theme 1: knowledge acquisition
Students reported a clearer understanding of research structures and terminology, along with improved ability to read journal articles, interpret data, and contextualize evidence within clinical learning.
Theme 2: attitudinal shifts
Participants described greater responsibility and motivation, enhanced teamwork, and an emerging recognition that research is an integral component of professional identity.
Theme 3: skill development
Participants highlighted a wide range of practical competencies grouped under the category of “skills.” In this context, skills denote observable capacities that students developed through the RCA, beyond knowledge and attitudes. Reported skills included technical abilities (e.g., using Excel for data management), communication skills (e.g., delivering presentations and engaging in professional dialogue with faculty and clinicians), and interpersonal skills (e.g., teamwork, leadership, and precision in collaborative tasks). Students regarded these competencies as foundational to academic and clinical success.
Challenges and suggestions for improvement
Theme 4: student participation
Large groups decreased accountability and added time burdens to private study.
Theme 5: research readiness
Gaps in technical skills and unclear guidance impeded progress; both groups favored standardized orientation and training.
Theme 6: financial constraints
Student-borne costs were common; faculty advocated for a formal institutional budget line.
Theme 7: scheduling conflicts
The RCA clashed with clinical rotation timetables; suggested remedies included protected time and curricular integration.
Theme 8: supervision styles
Supervisor engagement varied; students preferred senior mentorship, while faculty proposed more distributed, less hierarchical supervision.
Theme 9: coordination with clinicians in hospital settings
Hospital workload and communication barriers complicated data collection; designated clinical liaisons and formal notification systems were suggested.
Theme 10: data management
Sample-size feasibility and data quality were concerns; retrospective designs were viewed as more workable.
Theme 11: logistics of the RCA presentation event
Limited preparation time, unequal distribution of participation certificates, and unclear marking were noted; proposals included brief pre-event preparation windows, publishing student work, and stronger peer Q&A.
Theme 12: digitalization
Digital workflows were recommended to reduce printing costs and to build an RCA archive. While many participants emphasized the RCA’s educational benefits, others expressed frustration with large group sizes, repeated revisions, and inconsistent supervision—highlighting the ongoing implementation challenges. Cross-thematic analysis revealed shared priorities and clear opportunities for program enhancement. Despite role-specific perspectives, overlapping concerns and proposed solutions reflected a mutual investment in strengthening the RCA’s structure, relevance, and sustainability. Table 3 summarizes how the 12 themes were constructed (analytic route, primary voice, codes, and representative quotations), while Fig. 1 presents a thematic map linking learning mechanisms, KAS gains (Themes 1–3), contextual challenges (Themes 4–12), and suggested improvements.
Discussion
Key results
The RCA supported student development across KAS, while also revealing persistent implementation challenges. Issues previously noted informally in earlier RCA cycles—most notably time conflicts—were systematically confirmed in this study. Understanding was deepened by documenting both student and faculty perspectives. Faculty accounts closely mirrored those of students, and both groups proposed program-level improvements, including structured preparation, clearer supervision, better scheduling integration, and dedicated budget allocation.
Interpretation
Grounded in constructivism, the observed KAS gains reflect knowledge-building through authentic, collaborative inquiry. Variation across groups corresponded to cognitive-apprenticeship processes (modeling, coaching, and scaffolding) that were applied with uneven consistency among supervisors. These patterns align with the RCA’s intended principles of supervised, problem-oriented learning in medical education (see Results for detailed examples). To sustain impact in low-resource settings, institutional mechanisms are needed to address student preparation, supervision, time allocation, and access to modest resources (including digital support). These insights can inform the design of structured, curriculum-integrated research modules in similar contexts, offering a context-sensitive and adaptable approach to early research engagement in medical education. For detailed skill examples and case illustrations, readers are referred to the Results section.
Comparison with previous studies
Across diverse contexts, undergraduate research programs consistently promote motivation and skill development but face ongoing challenges related to supervision, time, and systemic constraints. In Oman, both students and supervisors reported benefits alongside heavy supervisory workloads [10]; in a US program, structured mentorship and protected time emerged as key enablers despite logistical barriers [11]. Studies in Saudi Arabia similarly identified structural obstacles—particularly limited time and mentorship shortages—which closely parallel the challenges reported by our participants [12]. In Tanzania, mentorship capacity was found to be a critical determinant of undergraduate research engagement, underscoring the importance of supervisory availability in resource-limited environments [13]. Sudanese medical students likewise expressed strong research interest while encountering practical limitations such as insufficient preparation and inadequate institutional resources [14]. Collectively, these studies affirm that undergraduate research initiatives enhance motivation and skills, yet sustainability is often constrained by supervisory burdens and systemic limitations. Our study extends this literature by providing a combined analysis of faculty and student perspectives within a single institutional context, adding granularity to the understanding of how research culture initiatives can be adapted in low-resource medical education environments.
Limitations
This single-institution study limits general transferability. The focus group design may have introduced social desirability and hierarchical influences, and participants did not review the transcripts or findings for validation. The KAS component followed a predefined framework, which may have constrained the emergence of novel themes. Data were self-reported and were not triangulated with RCA outputs, grades, or supervisor assessments (these were not collected). Moreover, the qualitative design did not allow quantification of theme prevalence. The feasibility of certain recommendations must be interpreted in light of Myanmar’s political and resource constraints during the study period. Finally, as data collection preceded the post-2022 diffusion of generative artificial intelligence (AI), future research should incorporate outcome-based measures and assess AI-related access and competencies.
Generalizability
While context-specific, the findings may be adaptable to other resource-constrained medical schools if key conditions are met—such as appropriate group sizing, preparatory training, structured supervision with protected time, modest funding, clinical liaison support, and digital tool integration. Accordingly, broad generalizations should be avoided. Instead, we propose the RCA as a context-sensitive model that warrants local piloting, iterative adaptation, and evaluation.
Suggestions
Future RCA practice should prioritize the development of clearer operational guidelines, implementation of pre-orientation and data management workshops, and strengthening of faculty supervision through targeted training and cross-departmental collaboration. Institutions can further enhance RCA effectiveness by adopting digital platforms for supervision and coordination and by integrating proposal-writing and research funding literacy modules to prepare students for sustained research engagement. These measures would help address the barriers identified in this study and enhance RCA’s immediate feasibility in resource-limited settings.
Conclusion
This study confirms the RCA’s value in fostering research capacity and professional attitudes among medical students while highlighting barriers related to supervision, scheduling, and resource availability. The RCA remains a promising and adaptable model for promoting a culture of research in resource-limited medical schools. To strengthen its practical application, future studies should prospectively assess knowledge–attitude–skill outcomes, compare supervision models and group sizes, evaluate protected-time scheduling with modest financing, and explore digital workflows and long-term follow-up to determine whether early exposure translates into sustained research engagement.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Farand P Dube T Zaccagnini M Bergeron L Benoit-Piau J St-Onge C Integrating a longitudinal course on the principles of research in an outcomes-based undergraduate medical education curriculum Perspect Med Educ 202413518526 https://doi.org/10.5334/pme.1264 10.5334/pme.126439429978 PMC 11488199 · doi ↗ · pubmed ↗
- 2Macharia EW Kahiri MW Challenges faced by students in conducting research project at Kenya Medical Training College Int J Community Med Public Health 20241129872995 https://doi.org/10.18203/2394-6040.ijcmph 20242156 10.18203/2394-6040.ijcmph 20242156 · doi ↗
- 3Sarhan MM Aljohani LN Alsaleh RI Mubaraki RA Almozaen MA Alharbi RS Barriers faced by undergraduate dental students when conducting research: a qualitative study BMC Med Educ 202525191 https://doi.org/10.1186/s 12909-025-06790-y 10.1186/s 12909-025-06790-y 39915773 PMC 11804027 · doi ↗ · pubmed ↗
- 4University of Medicine 1 Yangon The MBBS Program: Program Guide 2021 [Internet]University of Medicine 1 Yangon 2024[cited 2025 Aug 26]. Available from: https://um 1yangon.edu.mm/wp-content/uploads/2024/01/UM-1-MBBS Program-Guide-2021.pdf
- 5Arega NT Hunde TS Constructivist instructional approaches: a systematic review of evaluation-based evidence for effectiveness Rev Educ 202513 e 70040 https://doi.org/10.1002/rev 3.70040 10.1002/rev 3.70040 · doi ↗
- 6Lyons K Mc Laughlin JE Khanova J Roth MT Cognitive apprenticeship in health sciences education: a qualitative review Adv Health Sci Educ Theory Pract 201722723739 https://doi.org/10.1007/s 10459-016-9707-4 10.1007/s 10459-016-9707-427544386 · doi ↗ · pubmed ↗
- 7Kirtchuk L Markless S Communities of practice: a theoretical framework for undergraduate longitudinal placements Clin Teach 202421 e 13692 https://doi.org/10.1111/tct.13692 10.1111/tct.1369237957816 · doi ↗ · pubmed ↗
- 8Fife ST Gossner JD Deductive qualitative analysis: evaluating, expanding, and refining theory Int J Qual Methods 20242316094069241244856 https://doi.org/10.1177/16094069241244856 10.1177/16094069241244856 · doi ↗