Qualitative Analysis of Caregiver and Patient Experiences With and Barriers to Medical Nutrition Therapy Utilization in Pediatric Type 1 Diabetes
Svetlana Azova, Hannah Michelson, David Williams, Belinda Lennerz, Katharine Garvey

TL;DR
This study explores why families of children with type 1 diabetes struggle to use recommended nutrition therapy, identifying key barriers and experiences.
Contribution
The study introduces a theoretical model explaining barriers to medical nutrition therapy in pediatric type 1 diabetes through a socioecological lens.
Findings
Five domains of barriers to MNT utilization were identified: individual, shared child/caregiver-specific, interpersonal, institutional, and community/societal.
Key barriers included diabetes technologies affecting meal practices and the balance between caregiver involvement and patient independence.
Cultural and sociodemographic factors significantly influenced MNT utilization.
Abstract
Despite recommendations by major diabetes organizations, medical nutrition therapy (MNT) in pediatric type 1 diabetes (T1D) remains underutilized. Suboptimal prandial practices and limited engagement in nutritional counseling with the diabetes care team may impact health outcomes in these youth. This study aimed to understand patient and caregiver experiences with and barriers to MNT utilization. Utilizing the socioecological framework and the phenomenological research design augmented by grounded theory methods, we conducted semi-structured interviews with caregivers of patients with T1D < 18 years and youth with T1D 12–17 years with T1D duration ≥1 year. Emergent themes were used to generate a theoretical model of the relationship between the family unit encompassing the child with T1D and suboptimal MNT utilization. We recruited 9 caregivers and 9 patients. Qualitative analysis…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
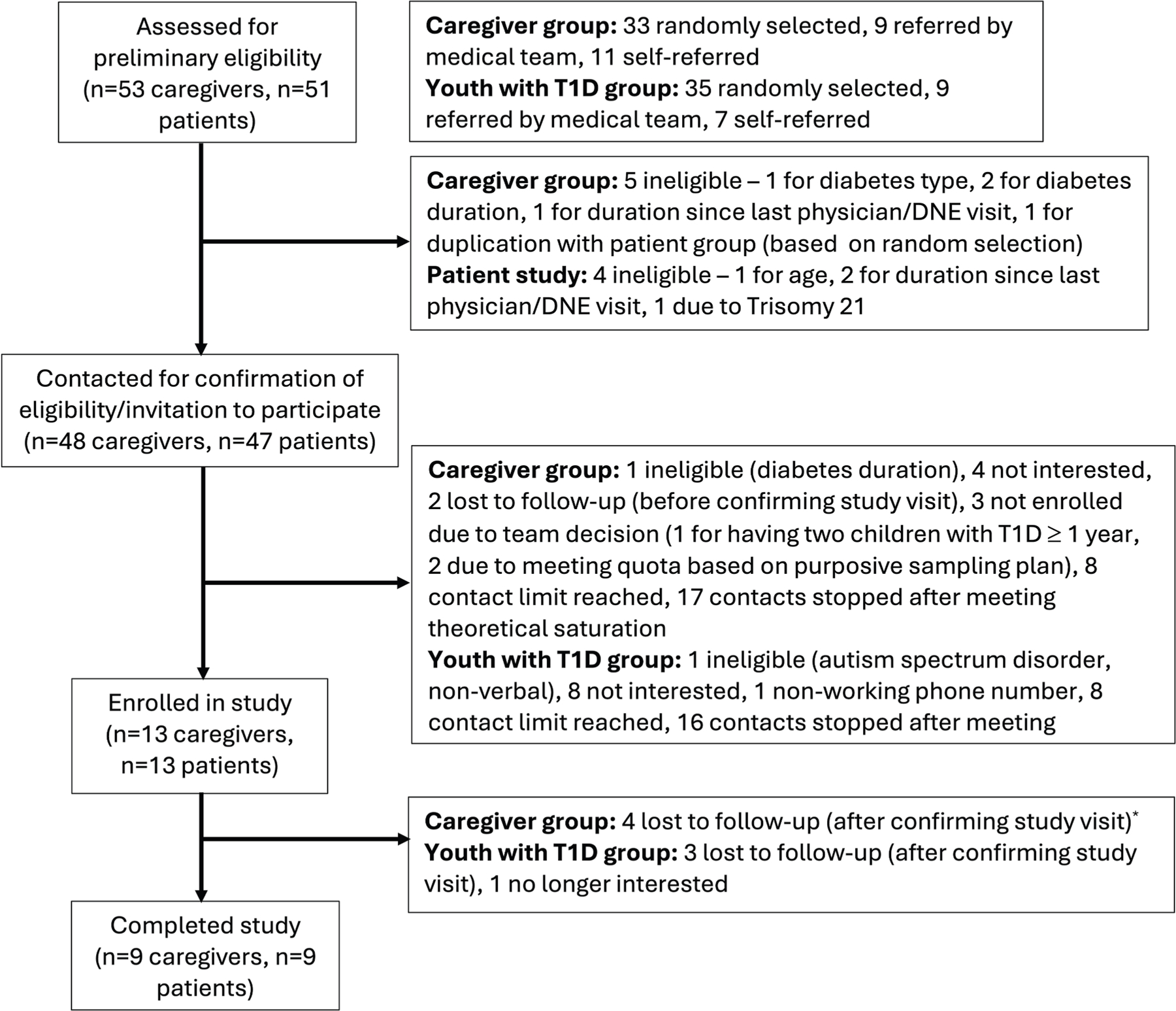 Figure 1
Figure 1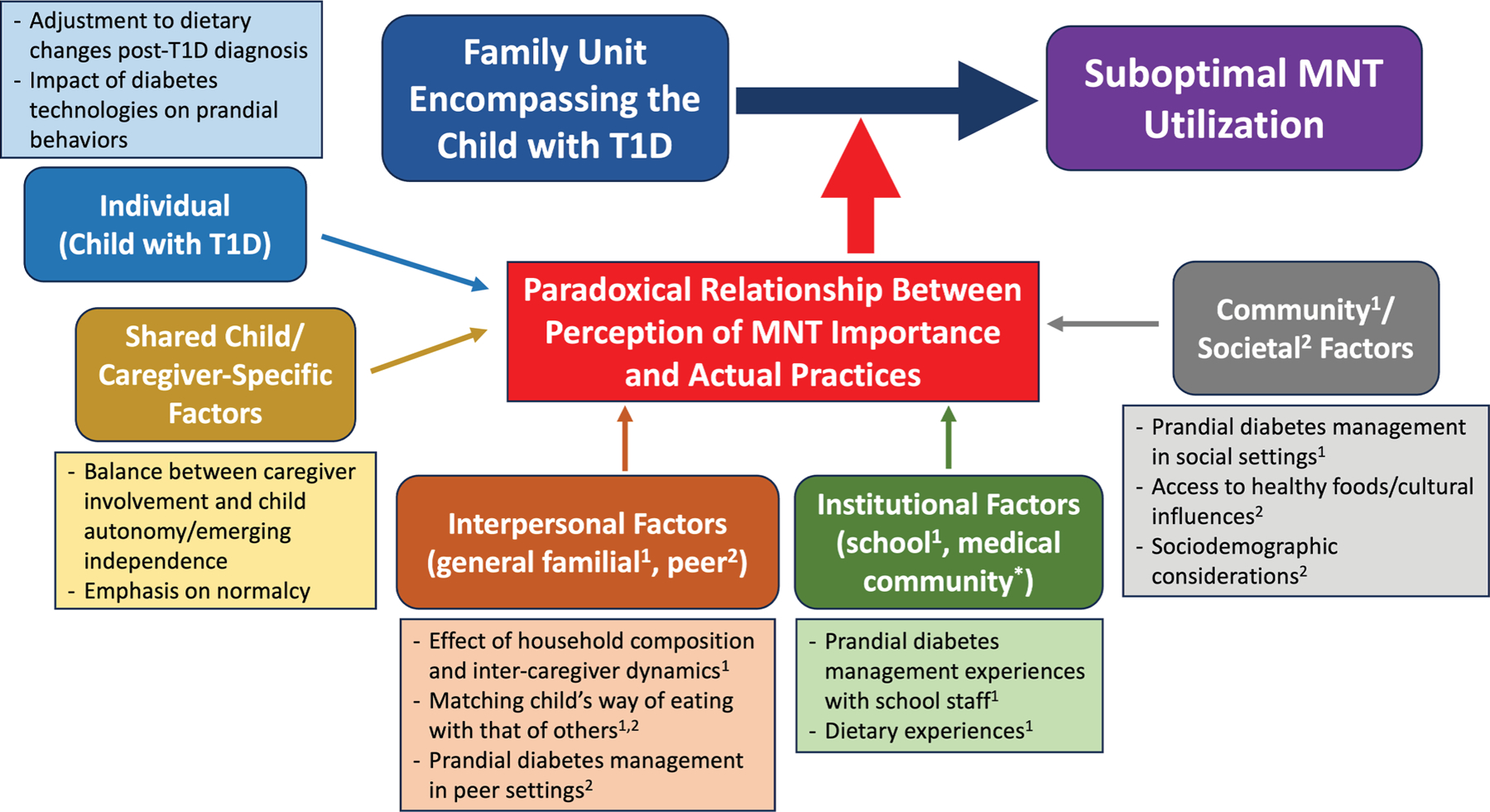 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdolescent and Pediatric Healthcare · Diabetes Management and Research · Child Nutrition and Feeding Issues
Introduction
Major diabetes organizations, including the American Diabetes Association (ADA) and International Society for Pediatric and Adolescent Diabetes, acknowledge the importance of individualized medical nutrition therapy (MNT) in children with type 1 diabetes (T1D) for glycemic and weight management and in the prevention of long-term complications.^1,2^ However, many children and families encounter challenges with optimal MNT utilization,^3–10^ despite documented glycemic^6,10–13^ and metabolic^5,7,14^ benefits. This is often manifested by suboptimal dietary quality^3,4,6,8^ and low engagement with a registered dietitian (RD).^9,10^ Prior studies identified several potential barriers. These included general concerns about time constraints, expense, child food preferences, and picky eating, and themes unique to diabetes, such as caregiver desire to avoid limiting their child’s diet or making them feel different^15,16^ and difficulties with carbohydrate estimation.^17^ Culturally-based nutritional challenges have also been identified among Hispanic caregivers of children with T1D.^18^
Most studies cited above have focused on assessing children’s adherence with the recommended RD follow-up or dietary composition from a caloric and macronutrient standpoint or evaluated caregivers’ perceived challenges to compliance with those guidelines.^3,4,6,8–10,15,17,18^ Qualitative research offers a unique opportunity to analyze the voices and lived experiences of participants to more deeply understand attitudes, beliefs, and expectations about care and ultimately inform intervention design. Our qualitative study involving separate semi-structured interviews with patients and caregivers of children with T1D is innovative in utilizing the socioecological framework^19^ to understand perceptions of MNT and barriers that may be contributing to MNT underutilization. We aimed to use our findings to build a theoretical model of factors impacting MNT utilization in pediatric T1D. Ultimately, understanding the drivers of and barriers to MNT utilization will facilitate design of interventions aimed at improving health outcomes in this population.
Methods
Study Design, Setting, and Selection of Participants
We utilized a phenomenological research design augmented by grounded theory methods^20^ to investigate drivers of and barriers to optimal MNT utilization in pediatric T1D. This hybrid research design allowed us to utilize the socioecological framework^19^ to explore the lived participant experiences with MNT and to identify knowledge gaps in our understanding of factors contributing to MNT underutilization. We assessed MNT utilization via a combination of prandial practices and engagement in nutritional counseling with the diabetes care team. Optimal prandial practices were based on whether the child’s reported way of eating generally met the benchmarks for a healthful diet^1,2^ and how well youth adhered with the recommended mealtime insulin administration practices (ie, pre-bolus dosing and carbohydrate/insulin matching).^1,2^ Engagement in nutritional counseling was assessed via whether participants had incorporated nutrition-focused discussions into routine clinical visits with their diabetes care team (eg, if the child had an RD visit in the electronic medical record [EMR] within the last 12 months of enrollment).
We conducted separate 1:1 semi-structured interviews with patients and caregivers of children with T1D followed by the Outpatient Diabetes Program at Boston Children’s Hospital (BCH), a large, pediatric, tertiary care, urban, academic medical center that serves approximately 2200 children with diabetes. All participants had a single study visit. Inclusion criteria were English-speaking caregivers of patients with T1D < 18 years and youth with T1D 12–17 years with T1D duration of ≥ 1 year and ≥ 1 diabetes medical visit at BCH in the past year. In addition, the participant had to be able to participate in the interview (eg, verbal, without prohibitive cognitive or developmental delays).
Eligible participants were identified from an Outpatient Diabetes Population Management database used for quality improvement and from review of the EMR. Initially, participants for each group (ie, caregiver and youth with T1D) were randomly selected from the database in blocks of 30 and maximum variation purposive sampling strategies were employed to recruit participants with a diverse distribution of characteristics of interest. These patient-related characteristics included age, sex, diabetes duration, use of a continuous glucose monitor (CGM), mode of insulin delivery, most recent hemoglobin A1c (HbA1c) (within the last 12 months prior to the date of random selection), and presence/absence of an RD visit within 1 year prior to the date of random selection. Email and telephone outreaches were conducted by trained study personnel. To aid in recruitment, we also approached several endocrinologists and diabetes nurse educators for potential referrals. Lastly, we posted study flyers at the BCH diabetes clinics and on the private BCH Diabetes Program Facebook and Instagram pages. If the same patient appeared in both cohorts on random selection, a team decision was made to only keep them on one list based on purposive sampling needs. However, if referred by the medical team, or contact was self-initiated, considerations for enrollment of both the child and caregiver were made on an individual basis, if combined interest was expressed. If a caregiver-patient dyad was enrolled for separate interviews, the interviewers performed 1 interview each prior to any analysis to avoid bias. As recruitment was ongoing, theoretical sampling was employed in response to emergent themes during analysis until data saturation was reached. All participants received $75 compensation.
Data Collection
To facilitate data collection, detailed interview guides (Supplemental Files 1 and 2) were developed covering 4 major topics: (1) general questions about the child’s T1D history, (2) general thoughts about the role of nutrition in a child’s T1D care, (3) patient-specific nutrition-related questions, and (4) experiences with nutrition-focused discussions and recommendations encountered during visits with the diabetes dietitian/nutritionist and medical providers (this data will be explored in a separate manuscript). The interview guides were developed by the research team, with consultation from faculty with expertise in pediatric T1D and qualitative research. While the guides contained prompts covering a comprehensive overview of topics to capture the needed data, interviewers were instructed to utilize a semi-structured style to provide deeper insights.
Two trained female interviewers (S.A., H.M.) conducted the semi-structured interviews between October 2023 and April 2024. Interviews were carried out virtually using the Zoom platform (Version 5) and lasted an average of 60 minutes. Interviews were audio- and video-recorded and transcribed using Hoffman Transcription. Interview transcripts were reviewed and edited for accuracy prior to analysis. In addition to the recordings, interviewers kept an observation log for each interview, writing down pertinent participant verbal comments and nonverbal cues and behaviors, and engaged in reflexivity reflections^20^ post-interview, documenting overall impressions and thoughts about emergent themes.
Data Analysis
Descriptive statistics were calculated and presented as means and standard deviations (after confirming normality with Shapiro-Wilk test) or proportions, as appropriate.
For qualitative analysis, the research team initially utilized a combination of inductive and deductive coding approaches and ultimately condensed their findings into categories and themes. Prior to coding, a multidisciplinary research team of pediatric endocrinologists, experts in qualitative research, and a research assistant created a draft codebook informed by the socioecological framework.^19^ Emergent coding was also utilized based on data from the first 6 interviews. The actual analysis consisted of 3 phases, led by the same 2 study team members who conducted the interviews (S.A., H.M.). In the first phase, each coder read the finalized interview transcript and then completed independent, blind level 1 coding of the interviews. After coding of an interview was complete, coders met and reviewed the applied codes, resolving any differences. The codebook was iteratively amended based on notes and observations from the first 6 coded interviews (3 caregiver, 3 patient). Those interviews were later recoded using the updated codes. Additional coders (K.G., D.W.) were available to resolve any discrepancies and disagreements in the coding.
In the second phase, after identifying a gap in our understanding of the exact drivers of MNT underutilization in pediatric T1D, the study team invoked grounded theory methods and engaged in axial coding to expand upon the core concepts and to connect the level 1 codes into broader categories. In the final phase, team members met to identify major themes and to explore the interconnections between these in order to build a theoretical model of factors mediating and impacting the relationship between the family unit encompassing the child with T1D and MNT utilization. Throughout this iterative process, we modified our recruitment efforts via theoretical sampling strategies to capture additional insights and observations needed to refine aspects of our emergent model that required further clarification. Data collection and analyses were completed when theoretical saturation was achieved. Throughout all phases, the coders engaged in analytic memo writing to generate additional insights and inform axial coding, higher level analysis, and acknowledgment of reflexivity.^20^ All analyses were performed using Dedoose software (Version 9.0.107, SocioCultural Research Consultants, LLC).^21^
Data Availability
The datasets generated during and analyzed in the current study and the coding dictionary used are available from the corresponding author upon reasonable request.
Results
Participant Characteristics
A total of 18 participants were included in the study (9 caregivers, 9 patients) (Fig. 1). There was only one caregiver-patient dyad that participated in the respective interviews, both self-referred. For the caregiver group, we present relevant characteristics for both the caregivers and the children on behalf of whom the interviews were conducted (Table 1). Almost all caregivers were female (88%), all were white, non-Hispanic, and completed more than 12 years of education, and the majority were in the higher-than-average income bracket. The average age of the children on behalf of whom the interviews were completed was 12.0 ± 5.2 years, 67% were female, and the majority had favorable HbA1c values and were using a CGM and automated insulin delivery (AID) system (similar to the statistics seen in our Diabetes Program). One child had celiac disease. Child characteristics in the youth with T1D group are summarized in Table 2. The average age of the youth was 15.5 ± 1.6 years, 56% were female, and the majority were using a CGM and AID system. Notably, only 33% of children in both cohorts had a single one-on-one RD visit in the prior year.
Qualitative Analysis
Our iterative analysis identified several key themes addressing drivers of and barriers to optimal MNT utilization in pediatric T1D that covered the 5 main interconnected domains, informed by the socioecological framework^19^: individual, shared child/caregiver-specific, interpersonal, institutional, and community/societal. The themes within each domain are presented below, supported by salient participant quotes. These themes were then used to generate a theoretical model depicting the intricate process that connects the family unit encompassing the child with T1D and suboptimal MNT utilization (Fig. 2). The central theme that emerged was a paradoxical relationship between appreciation of MNT importance and actual practices, with several emergent mediating themes, described below.
Domain 1: Individual (Child) Factors
Both caregivers and patients identified several individual (child) factors influencing the relationship between the family unit encompassing the child with T1D and MNT utilization. The quotes associated with each theme are presented in Table 3.
Theme 1: Difficulties with Adjustment to Dietary Changes Post-Diabetes Diagnosis.
Participants described challenges that children with T1D experienced when adjusting to diet-related changes post-diagnosis, which not uncommonly led to restricted eating behaviors in the child, sometimes also due to fear of or discomfort with insulin injections. Conversely, several participants described maladaptive strategies aimed at regaining a sense of food freedom and normalcy, including sneaking of food and using hypoglycemia as a catalyst. Factors that seemed to play a protective role in helping to facilitate adjustment included child age at T1D diagnosis, pre-diabetes eating habits, and the presence of routine/structure.
Theme 2: The Impact of Diabetes Technologies on Way of Eating and Prandial Behaviors.
Caregivers and patients described associations between diabetes technologies and maladaptive prandial behaviors in the child, including intake of foods of lower dietary quality due to a sense of increased food freedom and de-intensified prandial diabetes management practices. Concurrently, several participants noted benefits of diabetes technologies in facilitating prandial management.
Domain 2: Shared Child/Caregiver-Specific Factors
The following themes reflect factors relevant to both the child with T1D and the caregiver. The quotes associated with each theme are presented in Table 4.
Theme 1: Balance Between Caregiver Involvement and Child Autonomy/Emerging Independence When it Comes to the Child’s Nutritional Management.
Some participants described challenges with regard to emerging independence and balancing responsibility for the management of the child’s prandial behaviors, especially when it came to adolescents. The ability to effectively balance caregiver involvement and child autonomy through a collaborative approach was often associated with more optimal nutritional practices in the patient.
Theme 2: Relationship Between Acknowledgment of Optimal Prandial Management and its Execution.
Both patients and caregivers, while acknowledging the importance of optimal prandial management, identified several general challenges related to its execution.
Many participants acknowledged challenges with (1) prandial insulin timing and (2) carbohydrate/insulin matching (the latter in some cases attributed to fear of hypoglycemia). Many saw deviations from the expected practices as an adaptation for glycemic stability based on the current situation or prior experiences/observations. Regardless, participants often acknowledged the importance of these prandial practices.(3) Both caregivers and patients described management nuances and difficulties specific to various components of the meal/macronutrient composition (ie, differential effects of carbohydrates, glycemic index, protein, fat, and portion sizes on blood glucose) and foods that are challenging from a glycemic perspective. Some participants presented strategies for managing the differential effects of meal/macronutrient composition and challenging foods. Others gave examples of foods that had a more favorable effect on the child’s glycemic trends, often in association with a lower insulin requirement. Many participants also described observed/perceived effects of dietary factors on health beyond glycemia.(4) There were several factors driving approaches to the child’s way of eating, including emphasis on maintaining normalcy/not restricting. In addition, while none of the children with T1D in this study had a history of a diagnosed eating disorder, concern for the development of disordered dietary habits was not uncommon. These sentiments may have contributed to some participants describing the child’s overall diet quality as being suboptimal or variable. Many participants, however, also acknowledged the importance of mindful eating habits, translating into healthful practices in the child. When asked to assess their general understanding and comfort when it came to managing the child’s way of eating, participants often described these favorably. However, some noted fluctuations in their understanding and comfort or acknowledged that these alone were not always sufficient in optimizing MNT utilization.
Theme 3: Juxtaposition Between Perception of Overall Importance of Nutrition in T1D Care and Desire for Normalcy.
In addition to actual practices, overall participant perceptions about the role and importance of nutrition in T1D care also impacted MNT utilization in the child. The emphasis was once again on maintenance of normalcy and prioritization of diabetes management, although several participants expressed the general perception of the importance of making mindful choices when it comes to food options/practices and acknowledged the role of individualization. When asked about the overall importance of nutrition, many participants recognized the pivotal role that it plays both in diabetes management (including when compared to other treatment modalities) and overall health, amidst challenges balancing recognition and actual practice.
Domain 3: Interpersonal Factors
There were several general familial and peer-related factors impacting the relationship between the family unit encompassing the child with T1D and MNT utilization. The quotes associated with each theme are presented in Table 5.
Subdomain 1: General Familial Factors
Theme 1: Effect of Household Composition and Intercaregiver Dynamics on Approaches to the Child’s Way of Eating.
Nontraditional household composition and divergent approaches to way of eating presented challenges to the child’s nutritional management. Conversely, an intact household and convergent views on nutritional management were often protective factors when it came to optimal MNT utilization.
Theme 2: Attempts at Matching Child’s Way of Eating with That of the Rest of the Family.
Participants described challenges matching the family’s way of eating to that of the child with T1D. However, some caregivers shared the family’s successful attempts at supporting and integrating the child’s way of eating into their routine, despite potential challenges. Baseline familial dietary habits preceding the child’s T1D diagnosis at times facilitated this adjustment.
Subdomain 2: Peer-Related Factors.
In addition to dietary challenges related to the family unit, participants also described peer-related factors that have impacted the relationship between the child with T1D and MNT utilization. These included difficulties surrounding matching the child’s way of eating with that of the peers (Theme 1) and challenges with prandial diabetes management in peer settings (Theme 2).
Domain 4: Institutional Factors
Participants described school-related challenges that may have impacted the relationship between the child and MNT utilization. The quotes associated with each theme are presented in Table 6.
Theme 1: Variable Prandial Diabetes Management Experiences with School Staff.
Several participants acknowledged staff-related challenges when it came to the child’s prandial management at school. However, some participants endorsed more positive, collaborative interactions between the patient/family and school staff.
Theme 2: Suboptimal School-Related Dietary Experiences.
Both caregivers and patients also described specific diet-related challenges at school, often related to food quality. Some participants endorsed both (1) self-/family-directed and (2) school-related accommodations that facilitated the child’s nutritional management.
Domain 5: Community/Societal Factors
Broader community and societal factors also played an important role in mediating the relationship between the family unit encompassing the child with T1D and MNT utilization. The quotes associated with each theme are presented in Table 7.
Subdomain 1: Factors Related to Broader Community/Social Settings.
Participants described variable experiences with prandial diabetes management in social settings (Theme 1). Several noted challenges with proper insulin timing and carbohydrate/insulin matching (eg, due to the unpredictability of the meal composition at restaurants). Others felt self-conscious about insulin administration in public. Despite challenges, some participants endorsed adaptive prandial strategies in the social setting, including the availability of nutritional information in restaurants. A few emphasized the value of community support and education in helping to manage the child’s way of eating.
Subdomain 2: Societal Factors.
Larger societal factors also played a pivotal role in mediating the relationship between the family unit encompassing the child with T1D and MNT utilization. These included nutritional challenges stemming from easier access to foods of lower dietary quality, often in the setting of cultural influences (Theme 1), and potential impact of sociodemographic inequities on MNT utilization (Theme 2).
Discussion
Our qualitative analysis of semi-structured interviews elucidated valuable insights regarding experiences with MNT among both patients and caregivers of children with T1D and identified important barriers to MNT utilization using the socioecological framework. There was a central theme juxtaposing participant recognition of the importance of MNT in the management of the child’s T1D with challenges to its actual implementation, mediated by factors across 5 domains (individual, shared child/caregiver-specific, interpersonal, institutional, and community/societal). These challenges to MNT implementation included difficulties with adherence to a healthful way of eating, appropriate timing of prandial insulin administration, and proper carbohydrate/insulin matching and suboptimal engagement in nutritional counseling with the child’s diabetes care team (eg, absence of an RD visit within the prior year). Prior studies highlighted the emphasis on normalcy and avoidance of dietary restriction,^15,16^ as well as inherent challenges with carbohydrate estimation,^17^ as potential barriers. While our study offered further credence to these concepts, it expanded our understanding of the pivotal role that the child’s surrounding environment plays in ensuring optimal MNT utilization, underscoring the need for diabetes medical providers to consider and address factors that both encompass and extend beyond the child-caregiver dyad (eg, those related to the family unit as a whole, peers, school setting, and broader community) through patient-/family-centered strategies.
Among individual (child-related) factors, difficulties with adjustment to dietary changes post-T1D diagnosis often contributed to challenges with optimal MNT utilization, even amidst acknowledgment of its importance. Adjustment to a new, lifelong diagnosis is challenging, especially if it is associated with the need for multiple adaptations and changes to one’s previous lifestyle habits and routines. This applies to youth with T1D,^16^ which ultimately impacts their overall perceptions about and experiences with MNT. As demonstrated in our study, maladjustment to prandial changes can lead to food avoidance, which may increase future risk of disordered eating behaviors. These are relatively common in youth with T1D^22^ and should be screened for regularly during visits with the diabetes care team.^2^ Conversely, some children exhibited loosened dietary practices, including sneaking of food and using hypoglycemia as a catalyst for food freedom (particularly for high-carbohydrate items). While overtreatment of low blood glucoses in youth with T1D has been described, at times attributed to the fear of hypoglycemia,^23^ to our knowledge, the concept of using it as a way to regain a sense of normalcy has not been commonly reported.
Protective factors that facilitated adjustment to nutritional changes included younger age, baseline healthy eating habits, and presence of routine/structure. Patients that were diagnosed at a younger age tended to have an easier adaptation to nutritional changes, as these simply became part of their identity and felt just like normal events/persistent parts of life. In addition, children who had followed more healthy eating habits pre-diagnosis also had an easier adjustment to diet-related modifications following T1D diagnosis. Finally, presence of routines and schedules has previously been recognized in helping to facilitate diabetes self-management in youth with T1D.^24^ It is thus not surprising that adherence to routines set by families often helped optimize MNT utilization in the child, and deviations from set practices created both anticipated and unanticipated challenges. These factors are important to consider when approaching patients and families of children with T1D in order to appropriately tailor nutritional counseling to meet individual needs.
When it comes to diabetes technologies, and especially AID systems, the themes of increased food freedom and relaxed mealtime bolus dosing practices were prevalent in our study, often resulting in increased consumption of higher glycemic index foods, larger portion sizes, inconsistent pre-bolus dosing, and imprecise carbohydrate/insulin matching. While these devices have revolutionized the care of children with T1D, resulting in improved overall glycemic outcomes, reduced risk of hypoglycemia, and decreased disease burden,^25–27^ prior studies have suggested that their use may in fact be associated with the aforementioned maladaptive prandial practices^28–30^ and delivery of higher insulin doses,^27^ at least partially in response to post-prandial glycemic excursions. This can lead to both increased intake of lower quality foods and resultant excessive weight gain.^31^ While the idea of increased food freedom may certainly have benefits, especially in ameliorating disease burden and if restricted eating was previously a concern, access to foods of lower quality and improper prandial insulin management may have pronounced negative long-term consequences, especially on cardiometabolic health. Thus, concrete efforts should be made to properly educate patients using diabetes technologies, particularly AID systems, to continue to be mindful of their dietary choices and pay careful attention to proper prandial diabetes management.
This study also uncovered several shared themes among child and caregiver-specific factors impacting MNT utilization in youth with T1D. One recurring theme was the balance between caregiver involvement and emerging independence in the child with regard to nutritional management. It was evident from many interviews that with increasing independence, many children struggled to make healthy eating choices or engage in optimal prandial diabetes management practices. Older age was also recently identified as being associated with a lower likelihood of annual RD follow-up among children with T1D.^10^ The ADA acknowledges that self-management in pediatric diabetes should involve both youth and their caregivers, emphasizing the importance of family involvement through childhood and adolescence,^2^ which has been associated with positive outcomes when it comes to treatment adherence.^32^ With regard to nutritional management in T1D, several studies have shown that caregiver choices and perceptions impact youth diet quality.^33,34^ However, maintaining a balance between interdependence and independence can be challenging, especially in adolescence. This can certainly impact children’s prandial behaviors, as demonstrated in our study. A recurring protective factor in attaining an effective balance between caregiver involvement and patient independence in this study was the use of a collaborative approach and involving the child in the decision-making process, even starting at a young age, which may result in healthier nutritional choices. These concepts are important to consider when providing dietary counseling to families across different child age ranges and transitional stages.
Within the interpersonal domain, general familial factors also impacted the relationship between the child with T1D and MNT utilization. Among them was the effect of household composition and inter-caregiver dynamics on approaches to the child’s way of eating. Presence of nontraditional households without 2 intact caregivers may be associated with distinct struggles when it comes to all aspects of managing a chronic disease, including T1D, especially in the setting of concurrent sociodemographic challenges.^35^ In these cases, competing demands may force attention to be focused on the most critical aspects of care (ie, insulin management). Additionally, if more than one household is present, variability in approaches is possible, as described by several participants in this study, leading to inconsistencies in prandial management. The same may also apply to intact households where caregivers hold different perceptions regarding dietary practices. Conversely, convergent caregiver approaches and positive modeling behaviors are important factors in facilitating healthy eating habits in the child.^33,34^ Thus, these factors should be assessed for and incorporated into any nutritional counseling that occurs for youth with T1D and their families.
Related to both general familial and peer-related factors, participants also discussed challenges in matching the child’s way of eating with that of their family members and peers. When it comes to families, those with baseline mindful dietary practices typically had an easier time with integration. With regard to peers, the concept of trying to fit in and the impact of peer perceptions on diabetes self-management have been described in literature.^36,37^ In some studies, the presence of peer support seemed to have a positive impact on the emotional well-being and treatment adherence in adolescents with T1D,^32,37^ something that also came out in this study. These concepts underscore the importance of both assessing for possible general familial and peer-related challenges impacting diabetes self-management in youth and disseminating information on T1D to the community and schools, as well as empowering children and adolescents with this disease to provide appropriate education to their family members and peers.
Within the domain of institutional factors influencing the relationship between the family unit encompassing the child with T1D and MNT utilization, for this manuscript, we decided to highlight school-related considerations and challenges. Participants described both staff- and diet-related challenges impacting the child’s ability to optimally manage their way of eating and prandial behaviors at school. Some participants did identify both self-/family-directed and school-related accommodations, including bringing food from home and availability of carbohydrate counts for meals, respectively. However, the latter was not universally present, thus creating the potential for inequities in the children’s ability to properly manage prandial aspects of their diabetes at school. Both the ADA and other prior studies acknowledge the importance of proper diabetes management in schools, including providing appropriate training and support to the personnel responsible for the care of the child and ensuring access to the necessary nutritional information, which may ultimately improve patient outcomes and experiences.^2,38,39^ Public health advocacy efforts to improve the overall food quality at schools for all children are also important. The diabetes care team should regularly assess for these potential school-related barriers to optimal MNT utilization and advocate on behalf of their patients’ needs.
While not discussed within the scope of this manuscript, interactions within the medical community undoubtedly shape the way families and children with T1D approach MNT. It is notable that only 33% of participants in both cohorts had a single one-on-one RD visit within the year prior to enrollment. While low, this is higher than the average annual RD follow-up rate among youth with T1D recently identified at our institution (20.8%).^10^ Regardless, limited engagement with this important component of the diabetes care team can certainly impact participant perceptions and experiences regarding MNT and will be explored further in a separate analysis.
Lastly, but importantly, broader community and societal factors also played a role in how families and children with T1D approached MNT utilization. There was an aspect of unpredictability regarding available food options, carbohydrate content, and/or proper insulin management in social settings (eg, restaurants). In addition, some children felt perceived judgment and shame from others with regard to prandial insulin management in public. The latter has previously been described in the context of general challenges with diabetes self-management in social settings among youth with T1D.^36,37^ When it comes to societal influences, many called out the stereotypical American diet as generally not being the most healthful^40^ and described challenges with figuring out insulin doses to cover the carbohydrate content of foods without nutrition labels. Preference for prepackaged versus whole foods was previously described in T1D, due to the ease afforded by carbohydrate estimation for the former.^17^ High availability of and easy access to energy-dense foods/snacks, often leading to a lower diet quality in the child, may complicate glycemic management and increase future risk of cardiovascular disease in patients with T1D. Many participants in our study expressed desire for additional counseling on how to properly manage foods without nutrition labels.
Several caregivers also acknowledged that healthier foods tend to be more expensive. In one study, the presence of severe food insecurity in patients with type 2 diabetes was associated with higher body mass index in the setting of lower overall caloric consumption but intake of energy-dense foods with higher glycemic load.^41^ There is limited data on this topic in T1D,^42–46^ with documented associations between the presence of food insecurity and a higher HbA1c in youth with T1D,^42,46^ potentially mediated at least in part by the former’s impact on MNT.^44^ Cultural, racial, and ethnic challenges often have an impact on overall diet quality among individuals and may certainly affect both diabetes management^35^ and MNT utilization in youth with T1D.^18^ As an example, a recent study exploring the lived experiences of Hispanic caregivers of children with T1D followed by our institution identified culturally-based nutritional challenges, including difficulties with acculturation and integration, especially within the context of the T1D diagnosis, as well as uncertainty of how to incorporate medical advice into their dietary habits.^18^ Careful consideration of sociodemographic and cultural factors is imperative in providing individualized, equitable nutritional care to youth with T1D and their families.
This study has several limitations. The small sample size and lack of diversity may have limited the transferability of our findings. However, the comprehensiveness of the data collection within the context of the socioecological framework,^19^ the inclusion of both caregivers and patients, and the use of maximum variation purposive and theoretical sampling strategies allowed us to gather wide-ranging and representative insights regarding experiences with and barriers to MNT utilization among youth with T1D, thereby achieving data saturation. Nonetheless, we were unable to explore all potential barriers to MNT utilization in depth. For example, only one child in the study (caregiver group) had celiac disease, which presented unique insights, however, did not allow us to perform a comprehensive analysis. In addition, many children, particularly in the caregiver group, had favorable HbA1c values compared to the most recent average HbA1c in our overall diabetes population (8.0% ± 1.6%),^31^ missing opportunities to effectively understand how barriers to MNT utilization may impact prandial management of youth struggling to meet glycemic targets. Thus, future studies can focus on additional challenges related to MNT utilization in patients with certain comorbid conditions and those with higher HbA1c levels.
In addition, for the purposes of this study, we did not consider patient race and ethnicity or caregiver socioeconomic status and educational level under purposive sampling criteria, the former due to the availability of some recently published data (particularly for Hispanic youth followed by our program^18^) and the latter because of the logistical and ethical challenges in determining these at the time of recruitment and enrollment. All of the patients in our study identified as White, non-Hispanic (in our program, ~75% are White, non-Hispanic, ~5% Black, non-Hispanic, and ~10% Hispanic) and most caregivers in the caregiver cohort were in the middle-income bracket or higher and all completed 12+ years of education, suggesting a particularly motivated group and introducing selection bias. When it comes to race and ethnicity, while we did intend to recruit a more diverse sample, it is notable that for the caregiver group, 3 out of the 4 participants lost to follow-up after confirming the study visit had children that were either Black, non-Hispanic or Hispanic. This suggests potential unique challenges these families may face when it comes to participation in virtual interviews, despite the study team’s attempts to accommodate their specific situations (eg, agreeing to do the interviews in the evening or over the weekend). While our qualitative findings are likely not representative of the patient population as a whole, this study still generated important pilot data on MNT utilization perceptions and barriers, paving the road for the design of larger studies to capture the insights of families of children with T1D who come from historically marginalized backgrounds and/or have lower socioeconomic status and educational level in the caregiver(s).
Lastly, the potential for interviewer bias and power differential should be considered. Both interviewers made efforts to build rapport and ensure participant comfort (eg, emphasizing participant confidentiality and avoiding wearing a white coat), while maintaining professional distance, to ensure data validity. Researcher biases were continually examined through the use of reflexivity,^20^ engaging in reflective analytic memo writing following each interview and during every stage of the analysis.
Conclusions
In conclusion, this qualitative study of children and caregivers of youth with T1D provided an important opportunity to explore their experiences with MNT and to understand potential barriers to its optimal utilization. A socioecological framework was employed to characterize the conveyed challenges into individual, shared child/caregiver-specific, interpersonal, institutional, and community/societal domains. The central theme was the overall recognition of the importance of nutritional considerations in the management of the child with T1D juxtaposed against barriers to their implementation in real-life scenarios. In addition to providing useful preliminary data to inform broader investigative studies, we hope that our findings will help motivate the design of future interventions aimed at promoting MNT appreciation and utilization and improving both short- and long-term health outcomes in children with T1D.
Supplementary Material
MMC2
MMC1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Annan SF, Higgins LA, Jelleryd E, ISPAD clinical practice consensus guidelines 2022: nutritional management in children and adolescents with diabetes. Pediatr Diabetes. 2022;23(8):1297–1321.36468223 10.1111/pedi.13429 · doi ↗ · pubmed ↗
- 2American Diabetes Association Professional Practice C. 14. Children and adolescents: standards of care in Diabetes-2025. Diabetes Care. 2025;48(Supplement_1):S 283–S 305.39651980 10.2337/dc 25-S 014PMC 11635046 · doi ↗ · pubmed ↗
- 3Rovner AJ, Nansel TR. Are children with type 1 diabetes consuming a healthful diet?: a review of the current evidence and strategies for dietary change. Diabetes Educ 2009;35(1):97–107.19244565 10.1177/0145721708326699 PMC 2772111 · doi ↗ · pubmed ↗
- 4Patton SR. Adherence to diet in youth with type 1 diabetes. J Am Diet Assoc 2011;111(4):550–555.21443987 10.1016/j.jada.2011.01.016PMC 3066432 · doi ↗ · pubmed ↗
- 5Nansel TR, Haynie DL, Lipsky LM, Laffel LM, Mehta SN. Multiple indicators of poor diet quality in children and adolescents with type 1 diabetes are associated with higher body mass index percentile but not glycemic control. J Acad Nutr Diet. 2012;112(11):1728–1735.23102173 10.1016/j.jand.2012.08.029PMC 3985553 · doi ↗ · pubmed ↗
- 6Mackey ER, O’Brecht L, Holmes CS, Jacobs M, Streisand R. Teens with type 1 diabetes: how does their nutrition measure up? J Diabetes Res 2018;2018: 5094569.30258854 10.1155/2018/5094569 PMC 6146652 · doi ↗ · pubmed ↗
- 7Dluzniak-Golaska K, Panczyk M, Szostak-Wegierek D, Szypowska A, Sinska B. Analysis of the diet quality and dietary habits of children and adolescents with type 1 diabetes. Diabetes Metab Syndr Obes 2019;12:161–170.30705601 10.2147/DMSO.S 186237 PMC 6342209 · doi ↗ · pubmed ↗
- 8Şahin Bodur G, Keser A, Sıklar Z, Berberoğlu M. The relationship between diet quality of adolescents with Type 1 diabetes and nutritional status and biochemical parameters. J Clin Pract and Res 2021;43:458–464.