Designing a Self-Guided Digital Intervention for Self-Management of Shoulder Pain in People Living With Spinal Cord Injury: Tutorial on Using a Person-Based Approach
Verna Stavric, Nicola L Saywell, Nicola M Kayes

TL;DR
This paper explains how a digital shoulder pain management tool for spinal cord injury patients was designed using user-centered methods.
Contribution
The paper provides a detailed blueprint for operationalizing the person-based approach in digital intervention design.
Findings
A three-step process was used to design SPIN based on user needs and behavioral theory.
Guiding principles and design objectives were formulated to ensure the intervention's relevance and engagement.
The approach leverages existing evidence, tools like the Behaviour Change Wheel, and user feedback.
Abstract
Shoulder pain is prevalent in people living with spinal cord injury. Technology and digital rehabilitation tools are increasingly available, but this has not yet included the provision of a self-guided exercise intervention focused on managing shoulder pain for people living with spinal cord injury. We drew on the person-based approach (PBA) to intervention development to design a Shoulder Pain Intervention delivered over the interNet (SPIN) to address this gap. However, in preparation for the design process, we found very few published examples of how the PBA had been operationalized. The aim of this paper is to provide a detailed explanation of our approach and how we operationalized the PBA in the design of SPIN to maximize relevance and engagement. Our design process followed the key PBA steps, combining additional evidence and theoretical components. Each step ensured that guiding…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
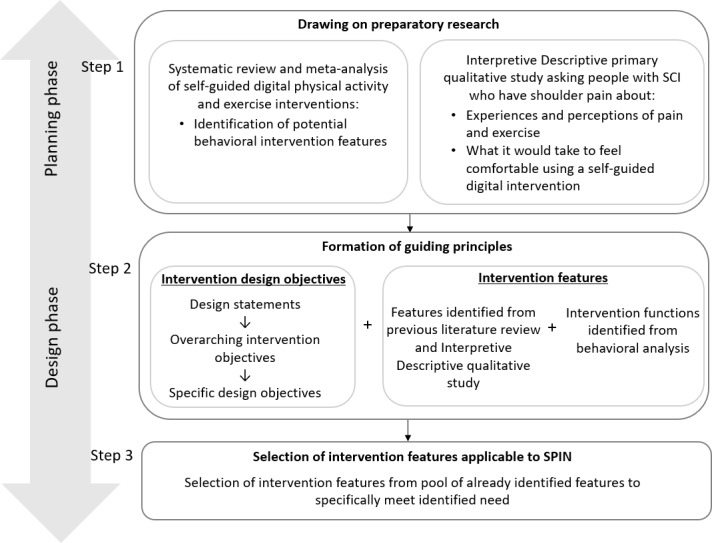 Figure 1
Figure 1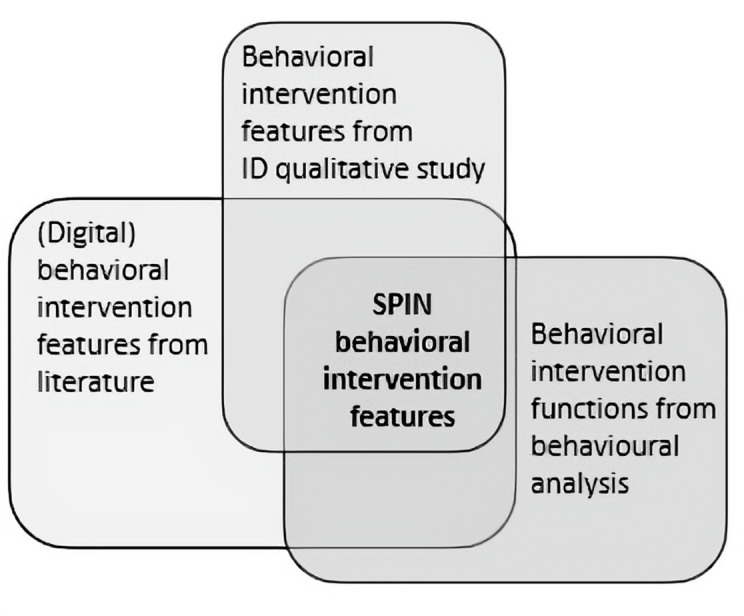 Figure 2
Figure 2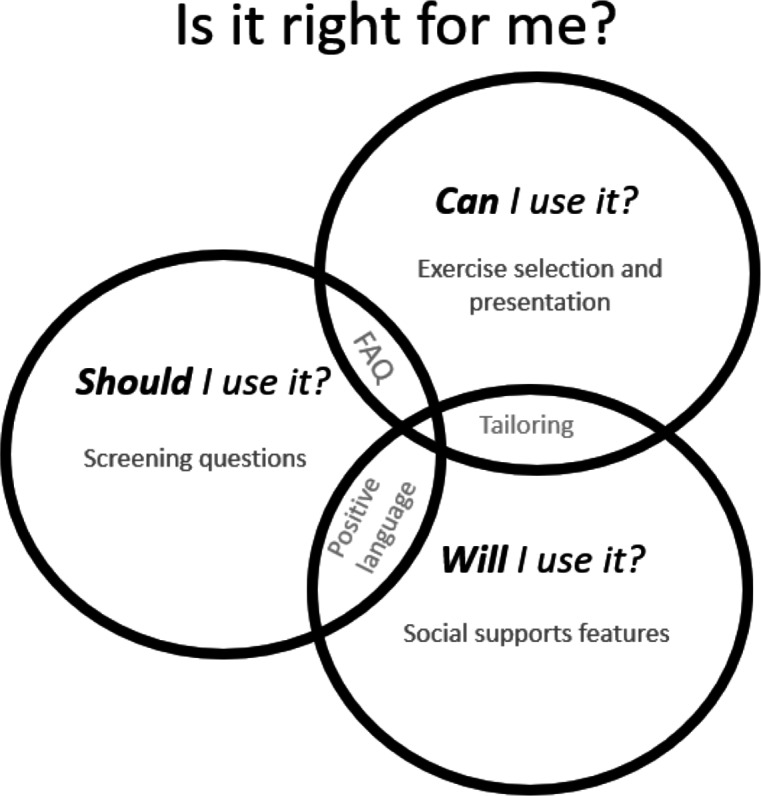 Figure 3
Figure 3| PBA | Phase | This study | |
|---|---|---|---|
| Purpose | Planned outcome | ||
| Use of primary and secondary |
| To determine |
A rich description of key |
| Formulation of | To design an |
Intervention design objectives Intervention features First iteration of SPIN | |
| Interpretive Descriptive qualitative study theme | Reframed to: design statements | Conditions for success |
|---|---|---|
|
| I should use it if: |
I believe it will work for me There is evidence of credibility There is a clear indication that it is suitable for me It resonates with my current attitude toward exercise, support situation |
|
| I can use it if: |
I can use it competently I can use it confidently It can be tailored and adapted to my unique needs I can use it safely, without causing more harm I have the belief that I could use it, given the resources and capacity I have I have the right support to use it |
|
| I will use it if: |
It is responsive to my unique needs It encourages me to progress when I am ready I feel supported to use it I can see progress as a consequence of using it It keeps me coming back |
| Design objectives that address identified needs, issues, and challenges | Working definition | Intervention functions | Intervention features that address the design objectives |
|---|---|---|---|
| To help users relate to and trust the program | The program will give users confidence in the source, message, and value of the program. The program is credible and legitimate and promotes trust. |
Education Training Modeling Enablement Persuasion |
Development team details (names, credentials, and contact info) Endorsements Evidence for shoulder pain exercises How user data will be used or stored Professional polished interface and function |
| To reassure users it will be clear who the program is suitable for, giving users confidence that the program is right for them and at what stage it is right for them | The program will guide users through a process to be able to screen for and identify if they are suitable to use the intervention and to promote trust and confidence that this is a safe and robust process. |
Education Training Modeling Enablement Persuasion |
Screening questionnaire/questions (that will exclude those unsuitable) Monitoring questions at each exercise event and tracking this information
Contact information for the team |
| To provide a sense of potential that it will work for them | The program will help users identify with it and the potential that it may have for them, in their current situation. |
Education Training Modeling Enablement Persuasion |
FAQ section addressing suitability of different situations “Is this right for me?” or “How do I know this is right for me?” or “Questions I can ask to make sure this is right for me?” |
| Design objectives that address identified needs, issues, and challenges | Working definition | Intervention functions | Intervention features that address the design objectives |
|---|---|---|---|
| To promote a sense of safety when using the program | The program will ensure exercises are at the appropriate difficulty level and will be responsive to changes in user presentation to ensure that they don’t significantly aggravate shoulder symptoms. |
Training Environmental restructuring Modeling Enablement |
Exercise selection based on user responses and a priori rules Program-generated advice based on user responses, such as acknowledging concerns, referral to |
| To promote user competence | The program will be easy to use by a range of users and in a range of circumstances, giving them a sense of confidence when using it in the context of their unique life situation. |
Training Environmental restructuring Modeling Enablement |
Language at an appropriate reading level Layout is clear and simple Font size and buttons are large for reduced hand function Minimal scrolling and clicking Consistent screen layout Clear signposts Logical interface Exercises presented in video and audio formats by pwSCI Exercises presented in step-by-step processes Exercises are planned to fit in with daily routine and normal digital device use Tunneling of information (releasing information in small amounts, as the user progresses through “right amount, at the right time”) Graded goal setting, implementation planning Praise for success Advice or support if not yet succeeded Digital use guidance when needed (help link) |
| To promote user autonomy | The program will give users a sense of control and ownership over the program and their progress through the program. |
Training Environmental restructuring Modeling Enablement |
Excercise selection, timing of exercise Intervention delivery Tunneling of options into the most common choices Suggestions or options for different situations |
| Design objectives that address identified needs, issues, and challenges | Working definition | Intervention functions | Intervention features that address the design objectives |
|---|---|---|---|
| To promote a positive emotional experience | The program will incorporate positive autonomy-supportive language that invites, informs, and supports users to work through the program. |
Training Environmental restructuring Enablement Modeling Education Persuasion Incentivization |
Use of Use of anecdotes to describe examples of success, decision-making Acknowledging and addressing concerns about using the program, such as pain or carer support Using Use of useful/interesting/relevant/personal reminders Positive or encouraging wording on feedback on progress toward the goal |
| To promote a sense of relatedness | The program will be relevant to the user by using communication and wording that is tailored to their self-identified preferences and personalized to their unique circumstances. |
Training Environmental restructuring Enablement Modeling Education Persuasion Incentivization |
Feedback as above (and that is immediately reciprocated when interacting with the intervention) Competition with others, and/or Cooperation with others Social connection through the program’s grouping Initial “getting to know you” questionnaire to help with Personalization: (1) identification (including username in correspondence), (2) raising expectation (including relevant information in correspondence that is based on users’ responses to questions/input), and (3) contextualization (
Self-identified support |
| To help users maintain their exercise over the 12 weeks | The program will use a variety of strategies and features to encourage and support users to maintain engagement in their exercise for the duration of the program. |
Training Environmental restructuring Enablement Modeling Education Persuasion Incentivization |
Rewards (points or similar)/competition Goal setting Action planning Communication that is |
| To promote a sense of accountability | The program will provide features that encourage the user to return to the program and to continue with the exercises. |
Training Environmental restructuring Enablement Modeling Education Persuasion Incentivization |
Competition with others or with self Support from others Communication that is Communication that is personalized Rewards that are only released upon completion of a certain amount of exercise |
| To promote a sense of progree and engagement | The program will enable the user to understand their progress through a clear and simple tracking feature. This will be done in a way that encourages further progress and ongoing engagement with the exercise intervention |
Training Environmental restructuring Enablement Modeling Education Persuasion Incentivization |
Feedback and tracking Choice in exercise selection Personalization
|
| Design objectives | Behavioral intervention feature | Identified in Interpretive Descriptive qualitative study | Identified in other literature not included in meta-analysis | |
|---|---|---|---|---|
|
| Ensuring personal relevance | 16 | ✓ | Horsch et al [ |
| Use of credibility and trust-enhancing features | 5 | ✓ | Bossen et al [ | |
|
| Provision of information about actual users | 2 | ✓ | Morrison et al [ |
|
| Allowance of the user to control or adapt features | 7 | ✓ | McClure et al [ |
|
| Ensuring ease of use | 6 | ✓ | Carter et al [ |
|
| Provision of information ‘just in time’ and in ‘just the right amount’ | 9 | ✓ | Oinas-Kukkonen and Harjumaa [ |
| Use of goal setting | 8 | ✓ | Webb et al [ | |
|
| Use of demonstration of behavior | 10 | ✓ | Webb et al [ |
|
| Use of feedback of behavior | 10 | ✓ | Webb et al [ |
|
| Use of tailored feedback | 10 | ✓ | Morrison et al [ |
| All | Use of tailoring based on a number of variables | 5 | ✓ | Morrison et al [ |
| Use of reminders | 8 | ✓ | Webb et al [ | |
| Use of self-monitoring features | 9 | ✓ | Morrison et al [ | |
| Use of positive tone and language | 4 | ✓ | Haines-Saah et al [ | |
| Use of text message | 3 | ✓ | Webb et al [ | |
|
| Use of action/coping planning | 5 | ✓ | Webb et al [ |
|
| Use of facilitation of social comparison and support | 2 | ✓ | Webb et al [ |
|
| Use of rewards and incentives | 1 | ✓ | Khadjesari et al [ |
| All | Use of a combination and a number of features | 14 | Webb et al [ |
| COM-B components | What needs to happen for the target behavior to occur? | Is there a need for change? |
|---|---|---|
| Physical capability | Have the physical ability to access SPIN features and functions and use it | No change needed as SPIN will only be suitable for people who can physically access and use it |
| Psychological capability | Believe they have the capability to use SPIN | |
| Psychological capability | Know that exercise can improve pain symptoms (or not make the condition worse) | |
| Physical opportunity | Have a device that can access SPIN | No change needed as SPIN will only be suitable for those people who have devices that can access SPIN |
| Social opportunity | Know about other pwSCI who have either benefitted from exercise for shoulder pain or are using SPIN | |
| Reflective motivation | Hold beliefs that exercising will reduce pain symptoms and/or improve activity | |
| Reflective motivation | Believe that SPIN has been developed by a credible and trustworthy source | |
| Automatic motivation | Believe that SPIN will identify those that are suitable (and unsuitable) to use it | |
| Automatic motivation | Need to feel that SPIN resonates (with current attitude toward exercise, support situation) | |
| Behavioral diagnosis of the relevant COM-B components | Psychological capability, social opportunity, reflective and automatic motivation need to change for the target behavior to occur | — |
| Likely ”intervention functions” that link to COM-B | Education (psychological capability, reflective motivation), Training (physical opportunity), Modelling (social opportunity), and Persuasion (reflective motivation, automatic motivation) | — |
| COM-B components | What needs to happen for the target behavior to occur? | Is there a need for change? |
|---|---|---|
| Physical capability | Have the physical ability to control and manipulate SPIN features and functions and related equipment and setup | |
| Physical capability | Have the additional support as required | |
| Psychological capability | Believe they have the capability to use SPIN | |
| Psychological capability | Know how to navigate through the intervention | |
| Psychological capability | Know how to perform exercises safely | |
| Physical opportunity | Have a program that is usable and easy to follow | |
| Social opportunity | Haencouragement from peers | |
| Reflective motivation | Have confidence in one’s ability to use the intervention program | |
| Reflective motivation | Have belief the intervention will enable achievement of outcomes important to user | |
| Automatic motivation | Have experience of benefit from intervention and sense of progress | |
| Behavioral diagnosis of the relevant COM-B components | Physical and psychological capability, physical and social opportunity, and reflective motivation need to change for the target behavior to occur | — |
| Likely ”intervention functions” that link to COM-B | Training (physical capability, psychological capability), Environmental restructuring (physical opportunity), Modelling (social opportunity), and Persuasion (reflective motivation) | — |
| COM-B components | What needs to happen for the target behavior to occur? | Is there a need for change? |
|---|---|---|
| Physical capability | Have the physical ability to control and manipulate SPIN features and functions and related equipment and setup | |
| Physical capability | Have the additional support as required | |
| Psychological capability | Believe they have the capability to use SPIN | |
| Psychological capability | Know how to navigate through the intervention | |
| Psychological capability | Know how to perform exercises safely | |
| Physical opportunity | Have a program that is usable and easy to follow | |
| Social opportunity | Have encouragement from peers | |
| Reflective motivation | Have confidence in one’s ability to use the intervention program | |
| Reflective motivation | Have belief the intervention will enable achievement of outcomes important to user | |
| Automatic motivation | Have experience of benefit from intervention and sense of progress | |
| Behavioral diagnosis of the relevant COM-B components | Physical and psychological capability, physical and social opportunity, and reflective motivation need to change for the target behavior to occur | — |
| Likely ”intervention functions” that link to COM-B | Training (physical capability, psychological capability), Environmental restructuring (physical opportunity), Modelling (social opportunity), and Persuasion (reflective motivation) | — |
| 1. Key steps in the person-based approach | 2. Methods we used to operationalize PBA | 3. Strengths and opportunities of our approach | 4. Questions to consider when planning this step |
|---|---|---|---|
| Step 1 (months 3‐6) Identify key behavioral issues (access), needs (not feeling competent), and challenges the intervention must address | Interpretive Descriptive qualitative study to explore user perspectives of self-guided exercise intervention and what would help or hinder uptake of a self-guided digital exercise intervention. Used probes and images during data collection to help users visualize and provide feedback on possible intervention features. | Drawing on Interpretive Descriptive as a nested study within the PBA process helped to provide a robust framework to capture and make sense of user needs and preferences. Interpretive Descriptive is congruent with the goals of PBA and has the benefit of (1) being oriented toward translation from the outset, (2) prioritizing the production of clinically relevant insights, and (3) flexibility in methods so data collection and analysis could be tailored to the intended use of findings for intervention development. | Who are the users? What is the best way to understand their unique context and specific needs? Are there existing tools and methods available that would be fit for purpose to capture user needs and preferences? How is the information going to be used? How might your approach to capturing needs and preferences be optimized for this intended use? Does data already exist (systematic reviews and qualitative research) that can help inform this step? |
| Step 2 (months 6-9-12) Creating intervention design objectives that capture what is unique about your intervention and reflect the specifically identified user needs and challenges the intervention needs to address. | Translate themes from the Interpretive Descriptive study into design statements and conditions for success, drawing on the data from each theme. | Helped to reframe the themes into actionable statements. Provided an evidence-based framework to underpin intervention design objectives. Ensured that user needs and preferences will continue to be reflected in the design process. | How are user needs and preferences currently expressed? Can they be used to underpin design objectives in their current form, or do they need some further refinement/transformation? |
| Step 2 (months 6-9-12) Creating intervention design objectives that capture what is unique about your intervention and reflect the specifically identified user needs and challenges the intervention needs to address. | Two overarching objectives for SPIN were developed from the design statements and conditions of success. It was repeatedly revised, referring to the original research question and design statements, and with input from stakeholders. | Developing 2 overarching objectives, rather than 1, helped to make explicit 2 interrelated but distinct objectives. The intermediary step of developing design objectives from the qualitative study themes ensured that the objectives represent the essence of the needs expressed by the users. Refining with input from stakeholders helped to ensure the objectives remained resonant with the SCI | What is(are) the overarching intervention objective(s)? How will you ensure your overarching objective(s) remain(s) grounded by user needs and preferences? Who might need to be involved in the development of intervention objective(s)? How will you know if your intervention objective(s) adequately capture(s) the perspectives of future users? |
| Step 2 (months 6-9-12) Creating intervention design objectives that capture what is unique about your intervention and reflect the specifically identified user needs and challenges the intervention needs to address. | Specific design objective were identified, drawing on the design statements and overarching intervention objectives. Working definitions were formulated with reference to original data sources and in collaborative discussions as a research team. | The development of specific design statements provided a framework to identify design requirements (system requirements) and intervention features. Investing time to develop the working definitions as a team, with reference to original data sources, was important for clarity and shared understanding. | What process will you use to generate specific design objectives from your overarching design objective(s)? Who might need to be involved in that process? What data sources do you have that you can refer to so you can refine your specific design objectives? |
| Step 3 (months 6‐12) Select and refine intervention features that support the specific design objectives. | Several methods were used to support the selection and refinement of intervention features for SPIN including: (1) extracting data on intervention features from a previous systematic review on self-guided exercise interventions, (2) reviewing relevant behavioral theory, (3) undertaking a behavioral analysis, and (4) drawing on persuasive system design. | Drawing on a multiplicity of methods in this step (1) ensured an evidence-based and theoretically informed approach and (2) enabled a systematic approach to ensure intervention features were those best suited to the behavioral needs of the SPIN user. A systematic approach to identifying intervention features and mapping them back to design objectives helps to imrove the credibility of intervention design. The outcome was a clear framework for SPIN intervention design that was a useful tool to support communication with design colleagues or software developers who were then bringing SPIN to form. | What data sources are available that can help you identify potential intervention features? What midrange theories are available that can help you identify potential intervention features? Are there existing tools and methods available that would be fit for purpose to help you identify intervention features which respond to user needs and preferences? Of all the potential intervention features, which are most likely to meet the design objective(s)? Who else should be involved in this process? How might you ensure that the outcome of this process can be an accessible and usable framework for others involved in intervention development? |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDigital Mental Health Interventions · Innovative Human-Technology Interaction · Spinal Cord Injury Research
Background
Overview
Shoulder pain is common in wheelchair users living with spinal cord injury (SCI) [12]. A lesion to the spinal cord can result in loss of innervation to muscles of the trunk and lower limbs. Consequently, many people living with SCI (pwSCI) rely on their upper extremities not only for performance of daily activities but also for locomotion. Shoulder pain can have a significant impact on their activity, reducing mobility, independence, and quality of life [1-5]. Digital and web-based interventions have increasingly been offered to pwSCI to promote exercise and physical activity [6-9]. These interventions minimize barriers to rehabilitation to address many health concerns, including managing their shoulder pain. Previous authors have found that in the general population, digital or web-based interventions can produce positive effects in various outcomes, such as physical activity [1011].
Technology-supported exercise interventions for pwSCI with persistent shoulder pain are currently available, but they have some limitations. They either require ongoing input and monitoring from a clinician [12-15] or provide general self-management advice [13] but without enough guidance to allow for clear and structured exercise progression specifically for shoulder pain. Self-guided digital exercise interventions have been successfully implemented for people with knee osteoarthritis [1617], dizziness [1819], and breast cancer [20] and may be a viable option for pwSCI. Our recent systematic review and meta-analysis of self-guided digital physical activity and exercise interventions demonstrated positive effects on physical activity at both short- and longer-term follow-up, in people living with chronic conditions [21]. We also found that interventions that used behavioral strategies and were underpinned by a theoretical framework were more effective. This suggests that self-guided digital interventions have the potential to support pwSCI to manage their shoulder pain, but that the intervention would need to be designed systematically and intentionally.
We have designed Shoulder Pain Intervention delivered over the interNet (SPIN) as a self-guided digital intervention to give pwSCI who experience shoulder pain the ability to access and progress evidence-based exercises. The intervention guides pwSCI to monitor symptoms and improvement [22] to promote autonomy in the management of their condition. The aim of SPIN is to be an engaging program that is responsive to the needs of pwSCI who have shoulder pain.
To achieve this, we were guided by the person-based approach (PBA) in the design of SPIN [23]. The PBA follows 4 iterative phases of intervention development that include (1) planning which seeks a deep understanding of the perspectives and psychosocial context of potential users through iterative qualitative research, (2) design based on guiding principles that have been created from insights from the first phase, (3) development and refinements which are made through iterative user feedback, and (4) trialing to evaluate the effectiveness on outcomes and impact on behavior change to make any necessary adjustments. Due to its focus on the development of digital behavior change interventions, the intent and purpose of PBA align well with adjacent behavior change theory and tools such as the COM-B [24], “Behaviour Change Wheel” [25], and behavioral analysis [26]. Furthermore, the PBA process is sufficiently flexible to enable the use of these (and other) tools to achieve the aims and purpose of a given phase. Integrating behavioral science theory and evidence while keeping users’ needs and contexts in focus has been found to maximize engagement and effectiveness of interventions [182527-31undefinedundefinedundefinedundefined]. This tutorial focuses on the first 2 PBA phases of planning and design. See Table 1 for an example of how our study was mapped onto the PBA.
We drew heavily on the existing PBA literature during the planning and designing stages of SPIN. However, the lack of access to detailed examples of how the PBA has been operationalized in practice made it challenging to translate the principles of this approach into reality. This is not a unique problem. Duncan and colleagues [32] noted that published work on the development of an intervention is frequently sparse because it is often included in the same publication as the reporting of a pilot or feasibility study.
Aim
The aim of this paper is to make clear how the principles of the PBA were operationalized in intervention design and the development of SPIN. We have illustrated our use of the PBA framework by outlining the detailed and explicit steps involved in the translation of the evidence, theory, and person-based recommendations into intervention design. In doing so, we have built on the existing methodological framework and enabled others to draw on this approach in future intervention design and development.
Methods and Outcomes
Overview
The planning and design phases of the PBA are described below, along with an overview of how they were operationalized in the design of SPIN. Figure 1 provides an overview of the SPIN design process and the components involved. Each step and its subsequent outcome have been described in detail in the sections that follow.
Overview of Shoulder Pain Intervention delivered over the Internet design steps and components. SCI: spinal cord injury; SPIN: Shoulder Pain Intervention delivered over the interNet.
Step 1: Drawing on Preparatory Research
Methods
This initial phase of the PBA draws on qualitative research, including interviews and focus groups, to gather in-depth insights into the psychological, social, and emotional factors that influence the users’ behavior. The goal is to identify the underlying motivations, beliefs, and barriers that may affect engagement with health interventions [23]. In the context of SPIN, this preparatory research included: (1) a systematic review and meta-analysis investigating the effectiveness of self-guided digital physical activity and exercise interventions [21] and (2) an Interpretive Descriptive qualitative study exploring the perceptions of pwSCI who have shoulder pain, on the use of a self-guided digital intervention to help them manage their shoulder pain [33].
Outcome
The review identified several self-guided digital physical activity and exercise interventions. Data extraction included identifying discrete intervention features and categorizing them using a purpose-built template (Multimedia Appendix 1), based on a synthesis of key literature [2734-40undefinedundefinedundefinedundefinedundefinedundefined]. Using this template, we extracted possible behavioral intervention features relating to qualities such as customizability, the provision of instruction, feedback and monitoring, tailoring, reminders and prompts, goals and planning, social support, and rewards and threats. We also noted the success of interventions using features that supported behavior, particularly self-regulation. This informed an initial pool of possible intervention features for SPIN that were reviewed later in Step 2.
The Interpretive Descriptive qualitative study identified themes that represented an evaluative process pwSCI go through when considering using a self-guided digital exercise intervention: Should I use it?, whether I believe it will work for me right now; Can I use it?, whether I can operate the intervention competently and confidently; and Will I use it?, whether it will be responsive to my unique needs and keep me coming back. These formed the basis of the design statements in Step 2.
Conceptual representations of possible behavioral intervention features identified from the review were used as probes and images during data collection in the Interpretive Descriptive qualitative study. These were used to prompt discussion about what could help pwSCI to engage in a self-guided digital intervention. The pwSCI discussed ways in which these concepts and specific features may support them. These perspectives were extracted from the audio recordings and tabulated to support the identification of behavioral intervention features in Step 2.
Step 2: Formation of Guiding Principles
Overview
The guiding principles in the PBA are formulated by synthesizing key insights from the planning phase (Step 1) into intervention design objectives and corresponding intervention features that address users’ specific needs, preferences, and behavioral barriers [23]. Yardley and colleagues [23] contend that staying true to the identified needs of the people who will use the intervention, throughout the design process, increases intervention relevance, engagement, and effectiveness. In our design of SPIN, we followed several stages to ensure the key context-specific behavioral needs and challenges identified in the Interpretive Descriptive qualitative study remained the focal point during intervention design.
Intervention Design Objectives
Yardley et al [23] suggest generating intervention design objectives to support the creation of the guiding principles but do not expand on how these may be identified. Below, we describe the method we followed to produce intervention design objectives through the creation of design statements, overarching intervention objectives, and specific intervention design objectives.
Design Statements
Methods
We created design statements by using the 3 themes constructed in the Interpretive Descriptive qualitative study. We first reframed each theme into a design statement, giving consideration to how each could be reflected in the design of the intervention. To do this, we reworded the themes to move from a question (Should I use it?) into a design statement (I should use it if…) and then added conditions applicable to each design statement. Each condition reflected key elements from the qualitative findings, resulting in person-centered conditions to be met in the design process. This process provided depth and context to inform the design of SPIN and ensured the next step would be underpinned by the perspectives of the future users of the intervention, in this case, pwSCI.
Outcome
The Interpretive Descriptive qualitative study themes, design statements, and key conditions for success are presented in Table 2.
Overarching Intervention Objectives
Methods
Next, we articulated the overarching intervention objectives. Succinctly describing the intervention objectives allows a snapshot of the key characteristics of the intervention [23]. We, therefore, clearly articulated how SPIN is distinctive and different from other interventions, reflecting the specific behavioral issues, needs, and challenges it must address.
We developed the intervention objectives iteratively, repeatedly revising the wording with reference to the original research question and design statements, and with input from the research team and stakeholders. Stakeholders included pwSCI, a clinician with experience in SCI rehabilitation, a clinician who was also a pwSCI and a representative of a relevant nongovernmental organization. Each iteration strived to reflect the essence of the needs expressed by the participants with wording that represented what ideal uptake and use of this self-guided digital exercise intervention could look like. The overarching intervention objectives were then used as a reference point for later design and development phases.
Outcome
Referring to the design statements and overall research aim, the overarching intervention objectives for SPIN were to:
Be tailored to users’ specific and unique needs so they can relate to it and trust it and so that it can be responsive to their changing needs while using SPIN; andEnable users to use it competently and confidently within their capabilities and support systems in a way that is safe and motivating.
Specific Design Objectives
Methods
Once the overarching intervention objectives were formulated, we created the specific design objectives underpinned by the design statements. We developed a working definition, incorporating the key conditions for success for each specific design objective, to ensure clarity in interpretation. These were then reviewed against the overarching intervention objectives, making sure they supported the overall objectives of SPIN. We continued to refine them as the design process progressed, during our planned discussion forums.
Outcome
Tables35 each refer to a different theme. Specific design objectives and working definitions are presented in the first 2 columns; intervention functions and features are discussed in later sections.
Intervention Features
In the PBA, the guiding principles inform the intervention features by providing a framework for selecting and shaping features that directly support the specific design objectives, and to improve resonance, engagement, and acceptability of an intervention [23]. A range of evidence informed the selection of behavioral intervention features: (1) in our review, we identified a range of features used in digital interventions that have been associated with better health-related outcomes [2734-36undefinedundefined]; (2) we identified possible behavioral intervention design features from our Interpretive Descriptive qualitative study [33]; and (3) we identified behavioral “intervention functions” we were trying to achieve using a behavioral analysis as per Michie and colleagues’ framework [26]. We then mapped these to the most relevant intervention features. Figure 2 represents the layers of evidence that informed SPIN’s intervention features. We will describe each of these in detail below.
Layers of evidence that informed Shoulder Pain Intervention delivered over the Interjet’s intervention features. ID: Interpretive Descriptive; SPIN: Shoulder Pain Intervention delivered over the interNet.
Identifying Behavioral Intervention Features From Previous Literature Review and the Interpretive Descriptive Qualitative Study
Methods
In Step 1, we had earlier identified potential behavioral intervention features for self-guided interventions that were identified from our systematic review and meta-analysis, using the specifically developed template, drawing from the CONSORT-EHEALTH checklist (V.1.6.1) [38]. See Multimedia Appendix 1 for a sample of our template showing sections used to record behavioral intervention features. For this current stage of the SPIN design, we also reviewed intervention features of publications that missed the strict inclusion criteria of the systematic review and meta-analysis but addressed digital delivery of physical activity or exercise intervention for possible relevant behavioral intervention features. We then integrated the data on specific features collected from our Interpretive Descriptive qualitative study. These data were categorized by proposed purpose and function and then mapped against the specific design objectives.
Outcome
There was overlap, resulting in some features identified as addressing more than one design objective. Many of the studies in the systematic review included digital behavioral intervention features that involved instruction on exercise or physical activity performance, self-monitoring of the exercise or physical activity behavior, goals and planning, and prompting. The results of the Interpretive Descriptive qualitative study and other reviewed literature suggested additional behavioral intervention features. Table 6 presents a summary of the behavioral intervention feature categories that we considered for SPIN, the design objective(s) they are related to, and the supporting evidence.
Identifying Intervention Functions From a Behavioral Analysis
Methods
We included a behavioral analysis using the “Behaviour Change Wheel” and COM-B model as outlined by Michie and colleagues [26]. This is a theoretical framework that provides a systematic way of identifying the problem and analyzing the behavioral needs of a target behavior. The “Behaviour Change Wheel” can support intervention design by linking the identified behavioral needs to “intervention functions” through a mechanism of action.
Consistent with the guiding principles and specific design objectives, and for the purpose of this behavioral analysis, we reframed the 3 themes from the Interpretive Descriptive qualitative study into target behaviors: Should I use it?—Signing up to SPIN (Table 7); Can I use it?—Using SPIN (Table 8); and Will I use it?—Returning to SPIN over the 12 weeks (Table 9). The COM-B Model was then used to identify the capability (C), opportunity (O), and motivational (M) components required for each of these behaviors (B) to occur, referring to the specific design objectives. The questions “what needs to happen for the target behavior to occur?” and “is there a need to change?” facilitated the analysis process [26]. We used this process to identify (or “diagnose”) the relevant COM-B components that need to be addressed for the target behavior to occur (see the Behavioral diagnosis of the relevant COM-B components in Tables79).
Next, we mapped these components to established ‘intervention functions,’ using the “Behaviour Change Wheel.” Most relevant “intervention functions” were then identified from the matrix of links between COM-B and intervention functions [26]. The “Behaviour Change Wheel” uses the term “intervention function” in lieu of intervention “type” or “category” since the same intervention feature may address more than 1 function [26].
Outcome
Tables79 present the target behavior for each design objective and what (if any) change is needed to occur based on the COM-B components. “Intervention functions” most likely to support behavior change have also been identified. For example, testimonials about positive experiences of using exercise to help with shoulder pain could be a form of modeling (providing an example for people to aspire to) and persuasion (using communication to induce positive feelings or stimulate action). This mapping process allowed each specific design objective to be checked to ensure it was supported by an appropriate “intervention function” and corresponding intervention feature. “Intervention functions” linked to the target behavior have been included in Likely “intervention functions” that link to the COM-B in each of the tables (Tables79). The guiding principles tables (Tables35) provide an overview of how these “intervention functions” map to the design objectives (“Intervention functions” column).
Step 3: Selection of Intervention Features Applicable to SPIN
Methods
The design phase of the PBA involves identifying intervention features and content, guided by the previously formulated guiding principles, to ensure alignment with users’ psychosocial contexts and to enhance relevance, acceptability, and engagement through iterative user feedback [23]. We were able to begin selecting specific SPIN intervention features once the behavioral analysis was complete. The behavioral intervention features previously identified (Table 6) were reviewed. We mapped those that we felt were contextually appropriate against the “intervention functions.” Each was checked to ensure it supported the specific design objectives and the overarching intervention objective. VS completed this process in consultation with coauthors.
Outcome
Collectively, Tables35 demonstrate a complete representation of the guiding principles of SPIN’s proposed intervention features and functions, mapped back to the design objectives. Some intervention features address more than 1 intervention design objective. These features have been italicized in Tables35. For example, having a forum for frequently asked questions may reduce barriers to starting the intervention and give users the information they need to progress. Having positive, encouraging language can attract users to start using the intervention and motivate them to continue with it. Other intervention features more clearly support only one of the intervention design objectives. Figure 3 schematically presents an example of how overlapping intervention features cohesively support SPIN’s identified design objectives.
Schematic representation of overlapping intervention features.
Application of Our Design Steps to Future Intervention Design
We believe that by explicating how we used the PBA in the development of SPIN, we can support others to use the PBA in the design of interventions. Table 10 provides a summary view of our process and includes some questions that we hope will prompt other researchers to consider how they might operationalize the use of PBA in their work. The table provides an overview of key phases of PBA and possible timelines (column 1) and examples from SPIN (column 2), including tools and methods we drew on as complementary to PBA and which we found useful in operationalizing the approach. In column 3, we have included our reflections on the benefits of our approach. The final column has questions that we hope will serve as prompts for researchers and designers when using this approach.
Ethical Considerations
Ethics approval (Auckland University of Technology Ethics Committee-AUTEC 18/263) and participant consent were received for the earlier work [33] that informed this work.
Discussion
Principal Findings
This paper has described how we applied evidence, theory, and person-based approaches in the design of a self-guided digital intervention to help pwSCI manage their shoulder pain. We have detailed the processes of applying the PBA to the design of SPIN.
This builds on Yardley and colleagues’ [23] collection of work. The PBA emphasizes a detailed, qualitative understanding of users’ psychosocial contexts to inform intervention design. It adds value to user-centered design by addressing factors that influence behavior change, beyond just usability. The PBA complements theory- and evidence-based frameworks, such as the “Behaviour Change Wheel” [25] by tailoring interventions to the needs and preferences of specific populations. Despite growing evidence for the use of the PBA framework in intervention design [29-316263undefinedundefined], there is little available on its operationalization. To our knowledge, the detailed reporting of each step has not been available before.
In a recent systematic review on the effectiveness of self-guided digital exercise interventions, Stavric et al [21] found that interventions with theoretical underpinning had increased congruence with the intervention features leading to significant positive results. This is supported by findings from McEwan [64] who found that theory-based interventions resulted in more consistent significant improvements in physical activity. The pwSCI and shoulder pain who will use SPIN are likely to have minimal contact with a health care professional. Therefore, successful design required an understanding of how SPIN would meet their needs and how pwSCI would use it in daily life in a self-directed way. Engaging people and evidence in intervention design is supported by a range of researchers and designers [233465]. Using a person-based approach, drawing on evidence from the people who will use the intervention, to derive the behavioral strategies has been shown to be effective in a variety of settings and methods of delivery [1829306667].
Despite acknowledgment that interventions supported by theory and evidence maximize outcomes [6869], there remains a paucity of full intervention description or design disclosure [70-73], making it challenging to explicate the link between theory and evidence and intervention features. A key tension we encountered was the limited availability of detailed examples of how the PBA had been operationalized in practice. This required us to make interpretive decisions when translating PBA principles into design elements, often without clear guidance. Additionally, balancing adherence to the PBA’s iterative, user-focused process with practical constraints such as time, resources, and access to participants posed challenges. These limitations were compounded by the fact that we were largely self-taught in the application of both the PBA and behavioral analysis frameworks.
Michie and colleagues [74] recognized the challenges and lack of clarity around the purported mechanisms by which digital interventions work during an international workshop on developing and evaluating digital interventions to promote behavior change in health. DiLiberto and colleagues [75] support the importance of “insider accounts” of intervention implementation and argue that the same transparent reporting practice should apply to intervention design. Of the 16 self-guided interventions included in our systematic review and meta-analysis conducted in the planning phase [21], only 6 provided any reference to methods used to plan, design, and develop them [1976-81undefinedundefinedundefinedundefinedundefined]. Of these, there was little supporting detail on how the design was carried out and none of the included studies reported exploring the behavioral needs of the users before designing the intervention. Future researchers might benefit from greater transparency and reporting of the design phase, including more practical examples of operationalizing person-based and behavioral approaches. Considerations for mitigating these challenges include allocating sufficient time and resources for user involvement beyond the planning stage, documenting key design decisions, and seeking opportunities for peer collaboration to support methodological alignment and confidence.
Strengths
We have shown commitment to providing a robust and transparent process in the operationalization of the design phase of SPIN drawing on the PBA approach. This process included explicitly addressing the identified behavioral needs of the users and kept these central throughout the entire design process. The design of SPIN has demonstrated how we used evidence (from existing literature and from a previous Interpretive Descriptive qualitative study) and theory (from behavioral analysis, “Behaviour Change Wheel,” and COM-B) to enhance the person-based process. This explicit and thorough process of planning and designing SPIN has provided a blueprint for intervention development when using PBA. It also addresses many of the limitations in the reporting on the development processes for existing self-guided digital exercise and physical activity-related interventions.
Limitations
Our operationalization of the PBA design phase reflects our interpretation of the PBA steps through available readings. We acknowledge there may be other perspectives and understandings. However, we believe that it is important to make our experiences visible to build on previous work and support future intervention design. Similarly, we relied on literature and online course instruction for support when we conducted the behavioral analysis using the COM-B. Being self-taught in both the PBA and behavioral analyses may mean that some aspects of our approach are not consistent with the original intent of these approaches. However, this is perhaps an artifact of the knowledge mobilization process, where the application of knowledge can change as knowledge changes hands. By offering transparency in our process, we hope that people can draw their own conclusions regarding the robustness of our approach. The design of SPIN did not include a logic model. Logic models typically include the main intervention components, how they relate to one another, which are meant to produce which effect, and include processes and expected outcomes. However, we did not believe a logic model would have been pragmatically useful as they assume causal relationships which may have restricted our thinking about solutions [82]. Our development process was underpinned by relationship building and community interaction, both of which are complex and require flexibility [8384].
Future Steps of SPIN Using the PBA
With the proposed intervention features selected, SPIN wireframes have been constructed. Wireframes are images or screenshots that show how screens of a website or app are structured and how content is arranged. These have provided a visual representation of the product and an opportunity to comment on content, features, and organization without getting distracted by aesthetics. Further participant consultation and design refinement have occurred. Frontend and backend software programming will occur at a later phase. Reporting of these stages will follow in a subsequent publication.
Conclusion
The design of SPIN has incorporated a deep understanding of the users’ needs and best available evidence by drawing on the PBA design process to maximize chances of engagement and outcomes. This paper has made visible the operationalization of each of the phases and can act as a blueprint to provide guidance to future researchers when using this approach.
Supplementary material
10.2196/66678Multimedia Appendix 1Systematic review data collection template.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dalyan M Cardenas DD Gerard B Upper extremity pain after spinal cord injury Spinal Cord Mar 1999373191195 doi 10.1038/sj.sc.3100802 Medline 10213328 · doi ↗ · pubmed ↗
- 2Curtis KA Drysdale GA Lanza RD Kolber M Vitolo RS West R Shoulder pain in wheelchair users with tetraplegia and paraplegia Arch Phys Med Rehabil Apr 1999804453457 doi 10.1016/s 0003-9993(99)90285-x Medline 10206610 · doi ↗ · pubmed ↗
- 3Gutierrez DD Thompson L Kemp B Mulroy SJ Physical Therapy Clinical Research Network Rehabilitation Research and Training Center on Aging-Related Changes in Impairment for Persons Living with Physical Disabilities The relationship of shoulder pain intensity to quality of life, physical activity, and community participation in persons with paraplegia J Spinal Cord Med 2007303251255 doi 10.1080/10790268.2007.11753933 Medline 17684891 PMC 2031955 · doi ↗ · pubmed ↗
- 4Mc Casland LD Budiman-Mak E Weaver FM Adams E Miskevics S Shoulder pain in the traumatically injured spinal cord patient: evaluation of risk factors and function J Clin Rheumatol Aug 2006124179186 doi 10.1097/01.rhu.0000230532.54403.25Medline 16891921 · doi ↗ · pubmed ↗
- 5Sie IH Waters RL Adkins RH Gellman H Upper extremity pain in the postrehabilitation spinal cord injured patient Arch Phys Med Rehabil 0119927314448 doi 10.5555/uri:pii:000399939290225 L Medline 1729973 · doi ↗ · pubmed ↗
- 6Coulter EH Mc Lean AN Hasler JP Allan DB Mc Fadyen A Paul L The effectiveness and satisfaction of web-based physiotherapy in people with spinal cord injury: a pilot randomised controlled trial Spinal Cord Apr 2017554383389 doi 10.1038/sc.2016.125Medline 27596027 · doi ↗ · pubmed ↗
- 7Best KL Bourassa S Sweet SN Routhier F Expert consensus for a digital peer-led approach to improving physical activity among individuals with spinal cord injury who use manual wheelchairs J Spinal Cord Med 01220234615361 doi 10.1080/10790268.2021.198630834726571 PMC 9897743 · doi ↗ · pubmed ↗
- 8Baehr LA Hiremath SV Bruneau M Jr et al Effect of Tele-exercise to Promote Empowered Movement for Individuals With Spinal Cord Injury (TEEMS) program on physical activity determinants and behavior: a mixed methods assessment Arch Phys Med Rehabil 0120241051101111 doi 10.1016/j.apmr.2023.08.019Medline 37678447 · doi ↗ · pubmed ↗