Painful Paroxysmal Dystonia as a Revealing Symptom of Multiple Sclerosis: A Case Report and Literature Review
Fatima Ez-Zahra Mabrouki, Samah Yousfi, Sanae Elhasnaoui, Yassine Mebrouk

TL;DR
A rare case of multiple sclerosis was identified through painful dystonic movements, highlighting the importance of recognizing unusual symptoms for early diagnosis.
Contribution
This case report emphasizes painful paroxysmal dystonia as a rare but significant initial symptom of multiple sclerosis.
Findings
A 51-year-old woman presented with painful dystonic movements linked to multiple sclerosis.
MRI confirmed demyelinating lesions consistent with MS, and corticosteroid therapy improved symptoms.
Early recognition of atypical motor symptoms is crucial for timely MS diagnosis and treatment.
Abstract
Multiple sclerosis (MS) can present with a wide range of motor symptoms, including movement disorders that are often underrecognized. Among these, painful paroxysmal dystonias, though rare, are particularly important to recognize when they occur as an initial manifestation. We report the case of a 51-year-old woman with no significant past medical history who presented with recurrent, brief, painful dystonic movements affecting the right upper limb and hemiface. Magnetic resonance imaging (MRI) revealed demyelinating lesions consistent with MS, and clinical improvement was achieved with corticosteroid therapy. Early recognition of such presentations is essential for accurate diagnosis and timely management.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
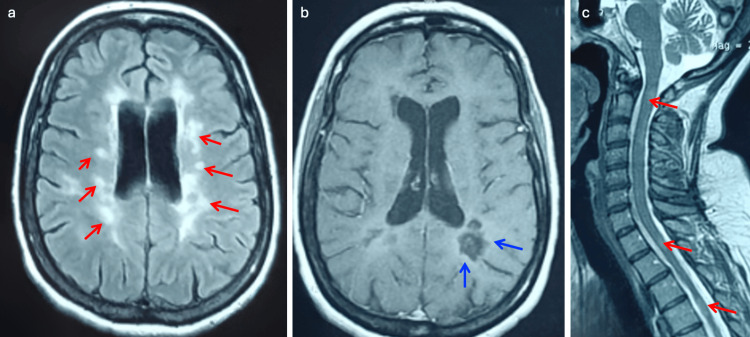 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurological and metabolic disorders · Botulinum Toxin and Related Neurological Disorders · Multiple Sclerosis Research Studies
Introduction
Multiple sclerosis (MS) is a chronic inflammatory and demyelinating disease of the central nervous system, marked by neuroinflammatory and neurodegenerative processes [1]. While its classic presentation involves motor or sensory deficits, visual loss, or cerebellar signs, a broader spectrum of paroxysmal phenomena has been documented, including painful dystonic episodes [2,3].
Painful paroxysmal dystonia, though underrecognized, may constitute an inaugural sign of MS and is frequently mistaken for focal seizures, leading to inappropriate workup and delays in diagnosis [4-6]. This report highlights the diagnostic value of such dystonias through a representative case, supplemented by a literature review on their pathophysiological mechanisms, imaging correlations, and treatment approaches.
Case presentation
A previously healthy, 51-year-old woman presented with brief, stereotyped, and intensely painful dystonic spasms affecting the right upper limb and hemiface. These episodes lasted only a few seconds but occurred frequently. The patient also reported a history of transient neurological symptoms with spontaneous resolution, suggestive of prior demyelinating events. These included episodes of visual blurring and paresthesias involving the right hemibody. Neurological examination revealed quadripyramidal signs, including spasticity, hyperreflexia, and posterior cord syndrome. Neuroimaging was performed to investigate the possibility of a basal ganglia lesion that could explain the clinical presentation. Magnetic resonance imaging (MRI) of the brain and spinal cord revealed multiple supratentorial and cervical demyelinating lesions, including enhancing lesions in the right centrum semiovale (Figure 1).
Brain (axial T2-FLAIR (a) and post-contrast T1 (b)) and cervical spinal cord (sagittal T1 (c)) MRI revealing multiple demyelinating lesions, including an enhancing lesion in the right centrum semiovaleFLAIR: fluid-attenuated inversion recovery
Oligoclonal bands were detected in the cerebrospinal fluid (CSF). Taken together, the clinical presentation, MRI findings of the brain and spinal cord, and the presence of oligoclonal bands in the CSF were consistent with a diagnosis of MS. A five-day course of intravenous methylprednisolone resulted in complete clinical remission, with the disappearance of the dystonic episodes. A disease-modifying therapy with fingolimod was subsequently initiated. After 15 months of treatment, the patient has experienced no clinical relapses, and her Expanded Disability Status Scale (EDSS) score remains at 1.
Discussion
Paroxysmal dystonia in MS is a rare phenomenon, with prevalence rates reported below 2% [7-9]. These episodes are characterized by sudden, involuntary, often painful muscle contractions that result in transient abnormal postures or movements. The episodes are typically brief, lasting from seconds to minutes, and may recur frequently, up to 100 times per day [7,9,10].
Historically termed “painful tonic spasms,” these movements are triggered by voluntary actions, sensory stimuli, or even hyperventilation [7,9,11]. They often lead to diagnostic confusion with focal seizures or other paroxysmal movement disorders.
The pathophysiology is believed to involve ephaptic transmission in demyelinated axons, particularly within the corticospinal tract [7,9-11]. Osterman et al. proposed that demyelinated fibers may abnormally discharge due to disrupted myelin integrity, allowing adjacent axons to cross-excite [9,11]. Inflammatory activity may exacerbate this process, explaining the rapid response to corticosteroids in many cases, including ours.
Imaging studies have identified possible involvement of the internal capsule, thalamus, basal ganglia, brainstem, and cervical spinal cord in generating these dystonic spasms [8,10,11]. However, no consistent radiological-clinical correlation has been universally validated, emphasizing the complex and multifocal nature of MS-related movement disorders.
The differential diagnosis includes epilepsy, tetany, stiff-person syndrome, and psychogenic movement disorders. In our patient, the episodic nature, stereotypy, absence of electroencephalogram (EEG) abnormalities, and response to steroids favored an MS-related paroxysmal dystonia rather than epileptic or functional origin.
Therapeutic options extend beyond corticosteroids. Antiepileptic drugs, such as carbamazepine, oxcarbazepine, levetiracetam, and phenytoin, have shown benefit in various series [9-11]. Acetazolamide, clonazepam, botulinum toxin, and even cannabis-based therapies have also been used with variable success [7,9-11]. In some cases, symptoms resolve spontaneously within weeks.
Ultimately, identification of dystonic paroxysms as an MS manifestation is critical. Their appearance may signal active demyelination and justify not only symptomatic management but also initiation or escalation of disease-modifying therapies [12].
Conclusions
Painful paroxysmal dystonias, though rare, are a clinically significant manifestation of MS. When appearing as inaugural symptoms, they pose diagnostic challenges and are often misinterpreted. Early recognition is essential to prevent diagnostic delays and to ensure the timely initiation of appropriate therapy. Corticosteroids and antiepileptics are effective in most cases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Movement disorders in multiple sclerosis and other demyelinating diseases J Neurol Sci Mehanna R Jankovic J 1832820132352252810.1016/j.jns.2013.02.007 · doi ↗ · pubmed ↗
- 2Paroxysmal symptoms in multiple sclerosis-a review of the literature J Clin Med Freiha J Riachi N Chalah MA Zoghaib R Ayache SS Ahdab R 3100920203299291810.3390/jcm 9103100 PMC 7600828 · doi ↗ · pubmed ↗
- 3Movement disorders in early MS and related diseases. A prospective observational study Neurol Clin Pract Abboud H Yu XX Knusel K Fernandez HH Cohen JA 2431920193085900410.1212/CPJ.0000000000000560 PMC 6382384 · doi ↗ · pubmed ↗
- 4Paroxysmal dystonia as an initial presentation of multiple sclerosis posing a diagnostic challenge Neurosciences (Riyadh) Al Dehailan AS 2362392420193138082510.17712/nsj.2018.3.20190025 PMC 8015510 · doi ↗ · pubmed ↗
- 5Les dystonies paroxystiques dans la sclérose en plaques (SEP) [Article in French]Rev Neurol (Paris) Delannoy E Maarouf A Caucheteux N Chaunu MP Dubard De Gaillarbois T Tourbah A 661712015
- 6Paroxysmal dystonia as the first manifestation of multiple sclerosis with internal capsular plaque [Article in Turkish]Noro Psikiyatr Ars Uca AU AltaşM 2952965120142836064410.4274/npa.y 7515 PMC 5353141 · doi ↗ · pubmed ↗
- 7Paroxysmal attacks in multiple sclerosis Mult Scler Tüzün E Akman-Demir G Eraksoy M 402404720011179546210.1177/135245850100700609 · doi ↗ · pubmed ↗
- 8Investigation of paroxysmal dystonia in a patient with multiple sclerosis: a transcranial magnetic stimulation study Clin Neurophysiol Trompetto C Avanzino L Bove M Buccolieri A Uccelli A Abbruzzese G 637011920081804242610.1016/j.clinph.2007.09.123 · doi ↗ · pubmed ↗