Factors Associated With Low Utilization of Cervical Cancer Screening Services in Gazipur, Bangladesh
Sadia Fatema Kabir, Muhammad Ashik-Ur-Rahman, Abdur Rahman, Md. Afzal Hossen, Rowfun Rahman, Farhana Huq, Mohibbul Haque, Junnatul Fardous Marfi, Md Abdullah Saeed Khan, Mohammad Delwer Hossain Hawlader

TL;DR
This study explores why few women in Bangladesh use cervical cancer screening services, finding fear and lack of knowledge are key barriers.
Contribution
The study identifies specific factors associated with low cervical cancer screening uptake in a specific Bangladeshi district.
Findings
Only 4.76% of women in the study had ever been screened for cervical cancer.
Fear of pain and shyness were the main reasons for not undergoing screening.
Low knowledge about screening's cancer-preventive role was linked to nonutilization.
Abstract
Despite its availability, cervical cancer screening services continue to remain underutilized in many regions. This study aimed to assess the prevalence and determinants of cervical cancer screening uptake among women in the north‐central area of Bangladesh. In this cross‐sectional study, between May and October 2022, women aged 30–60 years attending a tertiary care hospital in Gazipur district were approached for inclusion. Face‐to‐face interviews were conducted using a semistructured questionnaire. A total of 252 women were consecutively recruited within the study period. The self‐reported screening practice was recorded and verified by matching with identification numbers provided for screening by the hospital, and reasons for nonutilization were also collected. Only 12 women (4.76%) had ever been screened for cervical cancer. Lower knowledge scores (OR: 0.26 and 95% CI: 0.08–0.95)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
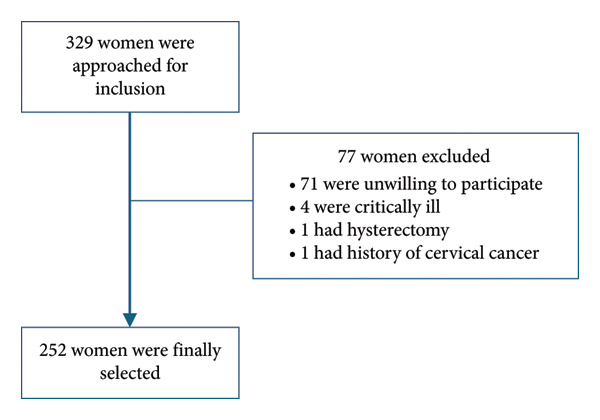 Figure 1
Figure 1| Characteristic |
|
|---|---|
| Age (years) | 38.59 (6.91) |
| Age groups (years) | |
| ≤ 30 years | 30 (11.90) |
| 31–40 years | 145 (57.54) |
| 41–50 years | 65 (25.79) |
| 51–60 years | 12 (4.76) |
| Education | |
| No formal education | 42 (16.67) |
| Primary | 94 (37.30) |
| SSC | 87 (34.52) |
| HSC | 10 (3.97) |
| Graduation and above | 19 (7.54) |
| Occupation | |
| Housewife | 207 (82.14) |
| Garment worker | 22 (8.73) |
| Job holder | 23 (9.13) |
| Husband’s education | |
| No formal education | 34 (13.50) |
| Primary | 71 (28.17) |
| SSC | 103 (40.87) |
| HSC | 17 (6.75) |
| Graduation and above | 27 (10.71) |
| Husband’s occupation | |
| Business | 59 (23.41) |
| Farmer | 56 (22.22) |
| Garment worker | 18 (7.14) |
| Job holder | 57 (22.62) |
| Others | 62 (24.60) |
| Monthly family income (BDT) | |
| ≤ 10,000 | 70 (27.78) |
| 10,001–20,000 | 134 (53.17) |
| 20,001–30,000 | 24 (9.52) |
| > 30,000 | 24 (9.52) |
| Residence | |
| Rural | 210 (83.33) |
| Urban | 42 (16.67) |
| Age of marriage | |
| ≤ 18 years | 219 (86.90) |
| > 18 years | 33 (13.10) |
| Number of family members | |
| More than four | 144 (57.14) |
| Up to four | 108 (42.86) |
| Comorbidities | |
| Absent | 220 (87.30) |
| Present | 32 (12.70) |
| Pain during menstruation | |
| Absent | 238 (94.44) |
| Present | 14 (5.56) |
| Regularity of menstrual cycle | |
| Irregular | 23 (9.13) |
| Regular | 229 (90.87) |
| Age at first pregnancy | |
| > 18 | 90 (35.71) |
| ≤ 18 | 162 (64.29) |
| Number of pregnancies | |
| One | 42 (16.67) |
| Two | 84 (33.33) |
| More than two | 126 (50.00) |
| Number of live births | |
| > 2 | 85 (33.73) |
| ≤ 2 | 167 (66.27) |
| Number of MR or abortion | |
| More than one | 14 (5.56) |
| None | 207 (82.14) |
| One | 31 (12.30) |
| Number of still births | |
| None | 235 (93.25) |
| One or more | 17 (6.75) |
| Hygiene product used | |
| Cloths and others | 145 (57.54) |
| Sanitary napkin | 107 (42.46) |
| Age at menarche (years) | |
| > 12 | 30 (11.90) |
| ≤ 12 | 222 (88.10) |
| Use of family planning method | 247 (98.02) |
| Oral contraceptives | 226 (89.68) |
| Condom | 28 (11.11) |
| Injectable contraceptives | 45 (17.86) |
| Other methods | 2 (0.79) |
| Knowledge score | 7.96 (0.55) |
| Attitude score | 12.56 (1.04) |
| Cervical cancer screening | |
| Ever screened | 12 (4.76) |
| Never screened | 240 (95.24) |
| Characteristic | Cervical cancer screening practice |
| |
|---|---|---|---|
| Ever screened, | Never screened, | ||
| Age (years) | 42.42 (10.43) | 38.40 (6.66) | 0.2122 |
| Education | 0.7583 | ||
| No formal education | 2 (4.76) | 40 (95.24) | |
| Primary | 5 (5.32) | 89 (94.68) | |
| SSC | 4 (4.60) | 83 (95.40) | |
| HSC | 1 (10.00) | 9 (90.00) | |
| Graduation and above | 0 (0.00) | 19 (100.00) | |
| Occupation | 0.6013 | ||
| Garment worker | 0 (0.00) | 22 (100.00) | |
| Housewife | 12 (5.80) | 195 (94.20) | |
| Job holder | 0 (0.00) | 23 (100.00) | |
| Husband’s education | 0.4323 | ||
| No formal education | 0 (0.00) | 34 (100.00) | |
| Primary | 5 (7.04) | 66 (92.96) | |
| SSC | 6 (5.83) | 97 (94.17) | |
| HSC | 1 (5.88) | 16 (94.12) | |
| Graduation and above | 0 (0.00) | 27 (100.00) | |
| Husband’s occupation |
| ||
| Business | 4 (6.78) | 55 (93.22) | |
| Farmer | 1 (1.79) | 55 (98.21) | |
| Garment worker | 0 (0.00) | 18 (100.00) | |
| Job holder | 0 (0.00) | 57 (100.00) | |
| Others | 7 (11.29) | 55 (88.71) | |
| Monthly family income (BDT) | 0.5993 | ||
| ≤ 10,000 | 3 (4.29) | 67 (95.71) | |
| 10,001–20,000 | 7 (5.22) | 127 (94.78) | |
| 20,001–30,000 | 2 (8.33) | 22 (91.67) | |
| > 30,000 | 0 (0.00) | 24 (100.00) | |
| Residence | 0.4283 | ||
| Rural | 9 (4.29) | 201 (95.71) | |
| Urban | 3 (7.14) | 39 (92.86) | |
| Age of marriage | 0.6613 | ||
| ≤ 18 years | 10 (4.57) | 209 (95.43) | |
| > 18 years | 2 (6.06) | 31 (93.94) | |
| Number of family members | 0.9324 | ||
| > 4 | 7 (4.86) | 137 (95.14) | |
| Up to 4 | 5 (4.63) | 103 (95.37) | |
| Any comorbidities | 0.1843 | ||
| Absent | 9 (4.09) | 211 (95.91) | |
| Present | 3 (9.38) | 29 (90.63) | |
| Pain during menstruation | > 0.9993 | ||
| Absent | 12 (5.04) | 226 (94.96) | |
| Present | 0 (0.00) | 14 (100.00) | |
| Regularity of menstrual cycle | 0.3013 | ||
| Irregular | 2 (8.70) | 21 (91.30) | |
| Regular | 10 (4.37) | 219 (95.63) | |
| Age at first pregnancy | 0.2223 | ||
| > 18 | 2 (2.22) | 88 (97.78) | |
| ≤ 18 | 10 (6.17) | 152 (93.83) | |
| Number of pregnancies | 0.3423 | ||
| More than two | 7 (5.56) | 119 (94.44) | |
| One | 0 (0.00) | 42 (100.00) | |
| Two | 5 (5.95) | 79 (94.05) | |
| Number of live births | 0.7563 | ||
| > 2 | 3 (3.53) | 82 (96.47) | |
| ≤ 2 | 9 (5.39) | 158 (94.61) | |
| Hygiene product used | 0.5124 | ||
| Cloths and others | 8 (5.52) | 137 (94.48) | |
| Sanitary napkin | 4 (3.74) | 103 (96.26) | |
| Age at menarche (years) | 0.3703 | ||
| > 12 | 0 (0.00) | 30 (100.00) | |
| ≤ 12 | 12 (5.41) | 210 (94.59) | |
| Use of family planning method |
| ||
| Yes | 10 (4.05) | 237 (95.95) | |
| No | 2 (40.00) | 3 (60.00) | |
| Number of MR or abortion | 0.1803 | ||
| More than one | 2 (14.29) | 12 (85.71) | |
| None | 9 (4.35) | 198 (95.65) | |
| One | 1 (3.23) | 30 (96.77) | |
| Number of still births | 0.5763 | ||
| None | 11 (4.68) | 224 (95.32) | |
| One or more | 1 (5.88) | 16 (94.12) | |
| Knowledge score | 8.25 (0.45) | 7.94 (0.55) |
|
| Knowledge categories | 0.3753 | ||
| Good | 12 (5.48) | 207 (94.52) | |
| Poor | 0 (0.00) | 33 (100.00) | |
| Attitude score | 13.25 (1.60) | 12.53 (1.00) | 0.1172 |
| Attitude categories | 0.3383 | ||
| Positive | 10 (4.41) | 217 (95.59) | |
| Negative | 2 (8.00) | 23 (92.00) | |
| Characteristic | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| OR1 | 95% CI1 |
| OR1 | 95% CI1 |
| |
| Husband’s occupation | ||||||
| Business | Ref | — | — | Ref | — | — |
| Farmer | 3.00 | 0.53–37.69 | 0.222 | 2.47 | 0.41–26.01 | 0.336 |
| Garment worker | 3.00 | 0.29–404.69 | 0.407 | 2.12 | 0.20–289.24 | 0.591 |
| Job holder | 9.32 | 0.96–1246.49 | 0.055 | 8.01 | 0.81–1075.05 | 0.080 |
| Others | 0.60 | 0.16–1.99 | 0.408 | 6.21 | 0.15–2.32 | 0.477 |
| Use of family planning method | ||||||
| Yes | 16.15 | 2.47–93.09 |
| 1.21 | 1.58–8.81 |
|
| No | Ref | — | — | Ref | — | — |
| Knowledge score | 0.31 | 0.10–1.00 | 0.051 | 0.26 | 0.08–0.95 |
|
| Characteristic∗ |
|
|---|---|
| Fear of pain | 236 (98.33) |
| Feels shy | 126 (52.50) |
| Feels healthy and does not see the necessity of vaccination | 22 (9.17) |
| Not informed about the cervical screening program | 6 (2.50) |
| Thinks the test is expensive | 3 (1.25) |
| Husband would disagree | 1 (0.42) |
| Undecided about screening | 1 (0.42) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCervical Cancer and HPV Research · Global Cancer Incidence and Screening · Reproductive tract infections research
1. Introduction
In 2020, cervical cancer accounted for 604,127 cases and 341,831 deaths [1], making it the fourth most common cancer among women around the world [2]. Bangladesh experienced an estimated 156,775 cervical cancer cases and 108,990 cancer deaths during the same year [3]. The cancer is predicted to cause the deaths of more than 500,000 women by the year 2070 at the current rate [4]. Cervical cancer is caused by persistent human papillomavirus (HPV) infection, making it one of the few cancers that can be prevented through vaccination. Moreover, through screening and early detection, it can be cured completely through surgical options like radical hysterectomy [5].
With the availability of the HPV vaccine, governments are now planning to eradicate the disease in the next 2 decades [2] through nationwide vaccination of adolescent girls. Although vaccination could lead to the prevention of cervical cancer, it has been found to be less effective among women who are currently aged 27–45 years [6]. Therefore, screening and treatment of precancerous lesions remain the mainstay of prevention of cancer progression and associated deaths in a large number of women.
Although cervical cancer screening services are widely available in public health facilities, the utilization of the services is low in low‐ and middle‐income countries (LMICs). The screening coverage was found, on average, to be 19% in LMICs compared with 63% in high‐income countries [7]. In Bangladesh, the coverage rate was estimated to be 11.30% [3], a figure much lower than average estimates of LMICs. In general, the lack of knowledge and awareness has been identified as the most prevalent individual‐level barrier to the low utilization of screening programs in low‐resource settings [8]. Fear of pain, fear of being diagnosed with cancer, procedure cost, and embarrassment were some other reported reasons for not using screening services in LMICs [8–11].
In Bangladesh, cervical cancer screening through the visual inspection with acetic acid (VIA) method is provided from primary to tertiary level hospitals through trained health care providers [12]. However, the VIA service remained predominantly an opportunistic service [13], with screening uptake mostly based on doctors’ advice, referral, or awareness. Previous studies found a low level of utilization of cervical cancer screening in different areas of Bangladesh [14–16], with a regional variation in cervical cancer awareness and utilization of screening services within the country. However, the extent of cervical cancer screening uptake and its determinants have not been explored in Gazipur, a densely populated district located in the north‐central part of the country. Moreover, the HPV vaccination was started in Gazipur by the government through a pilot program in 2015, which can be expected to raise awareness among adult women regarding cervical cancer in this area [11]. Therefore, the present study aimed to examine the extent of screening service uptake among women attending a tertiary care public hospital in the Gazipur district. In addition, it tried to find out the factors influencing utilization and the reasons for nonutilization. Our study findings could shed light on regional variations in cervical screening utilization and aid in planning targeted health education campaigns to improve utilization.
2. Materials and Methods
2.1. Study Design, Setting, and Population
This was a cross‐sectional study conducted in the outpatient department (OPD) of the Department of Gynecology and Obstetrics at Shaheed Tajuddin Ahmed Medical College Hospital (STAMCH) in Gazipur, Bangladesh, between May 2022 and October 2022. The district has an estimated 5,263,450 population, with nearly half of them being women [17]. Out of the five primary‐level healthcare centers, only one provides cervical cancer screening services. Hence, most of the eligible women in this area have to take the service from STAMCH, which is the public tertiary care hospital in the district. We approached married women aged 30–60 years seeking health from STAMCH for inclusion. Women with a history of cervical cancer or hysterectomy, any critical illness, and those unwilling to participate were excluded from the study. The sample size was calculated based on the formula n = z ^2^pq/d ^2^. Taking z = standard normal deviates at 95% confidence interval = 1.96, p = proportion of cervical cancer screening utilization among women aged 30–65 years = 21.2% [18], q = 1–p, and d = margin of error = 5%, and the total sample size was calculated to be 257. Finally, within the stipulated time, a total of 252 participants were consecutively recruited. See Figure 1 for a flow diagram of participant selection.
Participant selection diagram.
2.2. Data Collection Technique
Face‐to‐face interviews were conducted for data collection by two trained data collectors using a semistructured pretested questionnaire (S1 File). They consecutively approached female patients and their attendees who come to the outdoors for consultation. However, they were approached only after they have completed their consultation with a physician at outdoors.
2.3. Research Instrument
A semistructured questionnaire was developed based on previously published articles [3, 5, 15, 19, 20] and discussion with experts. It was pretested on 20 women to assess its adaptability. The questionnaire consisted of sections on sociodemographic characteristics, menstrual health, reproductive health, and knowledge, attitude, and practice related to cervical cancer screening.
2.4. Scoring
The scoring pattern of the knowledge and attitude‐related questions is tabulated in the S2 File.
2.4.1. Scoring of Knowledge‐Related Questions
A total of nine questions were asked to explore knowledge of cervical cancer and its screening covering symptoms, risk factors, prevention strategies, treatments, and cervical cancer screening frequency, age, and procedure. Scores were assigned as follows. A score of “1” was assigned for “yes” and “0” for “no” in questions with these two responses (K1, K2, and K3). The question on prevention methods (K4) had multiple‐choice options. However, a score of “1” was given for the selection of at least one choice, “0” was assigned for nonresponse. For the questions on the knowledge of whether cervical cancer can be treated or not, “1” was assigned for “yes” and “0” for either “no” or “do not know.” For treatment types (K6), “1” score was given for a choice of “surgery” and/or “radiotherapy,” “0” was assigned for selecting herbal remedies. For questions on frequency of screening (K7), “1” was assigned for the right answer only (every 5 years), the rest of the answers were assigned “0.” Although some places recommend screening every 3 years, we did not consider it a correct answer within the context of Bangladesh, where every 5 years is recommended and conventional knowledge. Similarly, for the question on who should be screened (K8), “1” was assigned for selecting “all women ≥ 25 years,” for the rest “0” was assigned. In procedures used in cervical screening, “1” was assigned for the selection of either “VIA” and/or “Pap smear,” and “0” was assigned for biopsy. Hence, the total score ranged between 0 and 9. A score of 80% or more (i.e., ≥ 8) was considered as having “good” knowledge; otherwise, “poor” knowledge.
2.4.2. Scoring of Attitude‐Related Questions
A total of five attitude‐related questions were asked, covering consequences, risks, and role of screening in the prevention of cervical cancer as well as willingness to screen. Each attitude‐related question had a response comprising a three‐point Likert scale: “Agree,” “Neither agree nor disagree,” and “disagree.” A score of “3,” “2,” and “1” was assigned for each response, respectively. Therefore, the total score ranged between 5 and 15. A score of 80% or more (≥ 12) was considered “positive” attitude; otherwise, “negative” attitude.
2.4.3. Screening Practice
For determining screening practice, a self‐reported question was asked on whether the participant ever screened for cervical cancer (i.e., used the service provided by the government for screening in the hospital). If the answer was yes, it was verified using the respective screening IDs provided by the hospital’s cervical cancer screening center. If the answer was “no,” a further question was asked to select from a list of eight reasons. These reasons were selected considering the context of the country, literature review [7], and discussion with experts.
2.5. Data Analysis
Data were analyzed using the statistical software RStudio 2023.12.1 + 402. As there were no missing data, no imputations were made. Descriptive statistics were expressed through frequency (proportion) and mean ± standard deviation for categorical and continuous variables, respectively. Pearson’s chi‐square test and Fisher’s exact test were used to assess associations between categorical factors and cervical cancer screening practice. Welch’s two‐sample t‐tests were used to explore differences in continuous variables across screening practice. Factors that became significant at bivariate screening were considered for exploration through logistic regression analysis. As one of the variables had complete separation across screening practice categories, we used Firth logistic regression [21] for the determination of independent factors behind “never screening” for cervical cancer. A p value of < 0.05 was considered significant for all statistical tests.
2.6. Ethical Considerations
Ethical approval was obtained from the Institutional Review Board of North South University. Permission was obtained from the hospital authorities. Written informed consent was obtained from all participants after explaining the study objectives. Participation was voluntary, and confidentiality was maintained throughout the study period. All procedures were conducted following the updated guidelines of the Declaration of Helsinki. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines was used to report the findings of this study. The check list can be found in S3 File. The artificial intelligence model Claude Sonnet 4.0 was used to enhance the writing of the manuscript as the authors are not native English speakers.
3. Results
The average age of patients was 38.59 ± 6.91 years (±SD). The majority were aged 31–40 years (57.54%), were housewives (82.14%), and had primary (37.30%) or secondary (34.52%) education. Most had a low family income of 10,001–20,000 BDT (53.17%), lived in rural areas (83.33%), and got married before age 18 (86.90%) (see Table 1).
Table 2 shows that only 12 women (4.76%) had ever been screened for cervical cancer. Those ever screened had significantly higher mean knowledge scores of 8.25 versus 7.94 (p = 0.047). Attitude was not found to be associated with screening practice. Women whose husbands had “other” occupations were more likely to be screened (11.29%) compared with business (6.78%), farming (1.79%), garment work (none), and jobs (none) (p = 0.024). However, the use of family planning methods was also significantly associated with never being screened (4.05% vs. 40.00%, p = 0.019).
On multivariable analysis, using any family planning method remained significantly associated with higher odds of never being screened (OR: 1.21, 95% CI: 1.58–8.81, and p = 0.018) compared with not using a method. Lower knowledge scores were significantly associated with higher odds of never being screened (OR: 0.26, 95% CI: 0.08–0.95, and p = 0.042) for each unit increase in knowledge score (see Table 3).
Table 4 shows the major reasons for not getting screened were fear of pain (98.33%), feeling shy (52.50%), and perceiving no necessity as they felt healthy (9.17%). Lack of information (2.50%) and perceiving the test as expensive (1.25%) were minor reasons.
The responses to different knowledge and attitude‐related questions are listed in Supporting Tables 1 and 2. Nearly all could identify vaginal bleeding (99.60%), foul smell (99.21%), and multiple sexual partners (99.21%) as symptoms and risk factors, respectively. However, only 15.08% knew screening prevents cervical cancer, and 75.40% did not think it could be treated, despite 85.32% recognizing radiotherapy as a treatment option. While 90.08% correctly stated the recommended 5‐year screening interval and 99.21% knew all women ≥ 25 years should be screened, awareness of screening procedures like Pap smear (0.79%) was very low compared with visual inspection with acetic acid (98.81%). Regarding attitudes, although most neither agreed nor disagreed that cervical cancer causes death (92.86%) or that any woman can acquire it (73.81%), 48.81% agreed screening is preventive. Encouragingly, willingness to get screened was high at 86.51% regardless of fee and 92.46% if free, suggesting costs and lack of access could be barriers.
4. Discussion
This cross‐sectional study explored the extent of cervical cancer screening utilization and associated factors among women aged 30–60 years attending a tertiary care hospital in Gazipur, Bangladesh. The key findings were the very low screening rate of only 4.76%, lower knowledge scores being associated with never being screened, and the use of family planning methods also being associated with never being screened. Fear of pain and shyness were the main reasons cited by the participants for nonutilization of cervical cancer screening service.
The screening rate of 4.76% is alarmingly low compared with the estimated national average of 11.30% [3] and far below the rates in high‐income countries (over 60%) [7]. It also falls far below the expected coverage of 40% of the target population in Bangladesh [12] and the World Health Organization recommended target of 70% [22]. Although our study was hospital based, as the majority of the women in this region were taking the service from our study center, the low utilization rate gives a good reflection of the community coverage. Hence, the utilization rate found in our study underscores major gaps in cervical cancer prevention efforts by the health authorities in this industrialized district of Bangladesh. A region‐focused approach to raise awareness regarding cervical cancer screening service availability and the benefits of using the service should be considered.
We found that the lower the knowledge scores, the higher the odds of never being screened. These findings relay a similar association observed in the community‐based study in Dhaka [15], the Capital of Bangladesh. Likewise, studies conducted in other countries like Ethiopia [23–25] and Iran [26] have also repeatedly shown this association, highlighting the pivotal role of educating women about cervical cancer screening.
While awareness of cervical cancer symptoms, risk factors like multiple partners, and the need for all women over 25 to be screened was quite high, knowledge of screening procedures like the Pap smear was extremely poor. The latter finding could be expected as the screening method used in Bangladesh is VIA, and hence, participants could be unaware of the Pap smear method. Disturbingly, most women did not think cervical cancer was treatable despite recognizing radiotherapy as a treatment option. One possibility could be that respondents linked radiotherapy with cancer in general, as the term “radiotherapy” is commonly heard as a treatment for malignancies, while “surgery” is less often heard as a treatment option for malignancies in general. Perhaps this is the reason for choosing radiotherapy as a therapeutic option by the participants.
Awareness that screening can actually prevent cervical cancer was lacking in over 80% of the participants. Studies have shown that the lack of knowledge and awareness about cervical cancer and its screening program is the most common reason for the low utilization of screening services in LMICs [8, 10]. As many potentially treatable cases are missed due to a lack of screening, this crucial gap in knowledge could be linked to low utilization and, thereby, to the increasing morbidity and mortality associated with cervical cancer in Bangladesh [3, 14].
Intriguingly, using family planning methods was strongly associated with never being screened in this study. One could hypothesize that women relying on family planning may have lower risk perceptions for gynecological cancers. One study found that less than 10% of married women who lived apart from their spouse ever had extramarital sex [27], and in the presence of a spouse, the practice would be much lower. This fact, when considered in the context that more than 98% of our participants were using one of the family planning methods, plausibly gave our participants a sense of security from the risk of cervical cancer.
Considering the experiences of experts and from piloting and reviewing the literature, we enlisted several reasons for the nonutilization of screening services to be explored among our participants. These were in addition to the questions for awareness and attitude. The reasons vary widely in distribution throughout the world [8, 10]. However, we observed that fear of pain and shyness were cited as the top reasons for not getting screened by the vast majority of participants in this study. Fear of pain has been reported as one of the reasons by women in Malawi [28] and South Africa [29] as well. Although none of the cervical cancer screening methods should cause pain, some women might experience pain due to the inexperienced handling of the speculum [30]. VIA, the method commonly used in our settings, is usually well received by the women [31]. Hence, the fear of pain might be expressing the fear of discomfort often felt by women undergoing cervical cancer screening [30]. Likewise, feeling embarrassed is often described as one of the main reasons for nonparticipation in screening programs. For example, a sample of Bruneian women [9] shared such a feeling. It has also been reported by many women who have undergone the procedure [30]. Hence, Qayum and colleagues [15] have highlighted the necessity of ensuring privacy during the screening procedure.
A small proportion of participants also perceived no necessity of cervical screening as they felt healthy. This probably indicates a lack of awareness about the purpose of cancer screening. Lack of information about the service and cost, although cited as the main reason for nonutilization [10] in other studies, appeared as a minor reason in our exploration.
Unlike findings from Iran [26], Tanzania [32], or Ethiopia [24, 25, 33], we did not find any association of low utilization of screening services with age, education, monthly income, parity, or residence, which probably could be a limitation due to a low proportion of women having screening services. However, this may also indicate that the low utilization behavior was similar irrespective of the sociodemographic and reproductive characteristics of women in the Gazipur district.
Based on the findings of the questions, we noted that a majority of participants believed that cervical cancer is untreatable, and a few mentioned herbal remedies. These findings suggest a need for stronger public education emphasizing that cervical cancer is treatable, especially if detected early. Recommended medical treatments, for example, surgery, radiotherapy, and chemotherapy, should be clearly communicated through health messaging. Also, knowledge appears limited to VIA, with almost no recognition of Pap smears or HPV testing. While this could be due to the availability of VIA as the most accessible and practiced option in this context, the health education materials should still present a full picture of available screening methods, particularly in better‐resourced or urban settings. Also, the belief that only certain groups (e.g., sex workers) are at risk persists. Educational strategies must clarify that all women ≥ 25 years are at risk and should be screened. The fatal consequences of untreated cervical cancer should also be more strongly emphasized to convey urgency and relevance.
Despite the knowledge and practice gap and the reasons behind it, an encouraging finding was that nearly half the participants agreed cervical cancer screening is preventive, and more than four‐fifths were willing to get screened despite fees, a figure concordant with the pooled acceptance of screening service of 89.5% across the globe [34]. This positive attitude could be leveraged by the health authorities to motivate women to come to the screening centers and increase the screening coverage in this region.
The study’s strengths include being one of the earliest to explore cervical cancer utilization practice and reasons behind nonpractice in Gazipur, Bangladesh. Moreover, the utilization of cervical cancer screening was confirmed through records of the patients. Limitations are the relatively small sample size from a single tertiary care center and the consecutive sampling approach. However, women coming from the community to consult for their problems in the outdoors and indoors of hospitals have an inherent randomness in the sense that for any consecutive sample of them would be random, and their reasons for consultation do not follow any specific pattern and are not related to cervical cancer screening. Also, the accompanying female attendees are apparently healthy. Hence, a consecutively taken sample from both female patients and attendees could be considered representative of the community living in Gazipur. The potential recall bias associated with self‐reporting of practice was minimized through confirmation of screening from records for those giving an affirmative answer. For participants giving a negative answer, the possibility of recall bias was expected to be low because of the sensitivity of the method used in the screening process. To avoid self‐selection bias, we ensured consecutive sampling of participants coming to the outdoors irrespective of their reasons and that they were not conveniently included. However, the possibility of a desirability bias, demonstrated through a high proportion of correct answers despite poor practice, could not be avoided.
In conclusion, this study flags an alarmingly low cervical cancer screening rate in an area of Bangladesh and highlights critical gaps in knowledge that need to be addressed through educational interventions to improve screening uptake. Innovative measures to alleviate fear, embarrassment, and other barriers are essential for an effective screening program. On this point, patient education programs explaining the objectives and process of screening could be arranged, and screening provisions maintaining strict privacy by female health workers should be ensured.
Conflicts of Interest
The authors declare no conflicts of interest.
Funding
The study did not receive any funds.
Supporting Information
Additional supporting information can be found online in the Supporting Information section.
Supporting information
Supporting Information 1 Supporting Table 1. Participant’s responses to questions related to knowledge of cervical cancer screening.
Supporting Information 2 Supporting Table 2. Participant’s responses to questions related to attitude towards cervical cancer screening.
Supporting Information 3 S1 File. Questionnaire.
Supporting Information 4 S2 File. Knowledge and Attitude Question Scoring Codebook.
Supporting Information 5 S3 File. STROBE Checklist for Cross‐sectional Study.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Singh D. , Vignat J. , Lorenzoni V. et al., Global Estimates of Incidence and Mortality of Cervical Cancer in 2020: A Baseline Analysis of the WHO Global Cervical Cancer Elimination Initiative, Lancet Global Health. (2023) 11, no. 2, e 197–e 206, 10.1016/S 2214-109X(22)00501-0.36528031 PMC 9848409 · doi ↗ · pubmed ↗
- 2World Health Organization , Cervical Cancer, 2024.
- 3Uddin A. F. M. K. , Sumon M. A. , Pervin S. , and Sharmin F. , Cervical Cancer in Bangladesh, South Asian J Cancer. (2023) 12, no. 01, 036–038, 10.1055/s-0043-1764202.PMC 996615836851938 · doi ↗ · pubmed ↗
- 4Canfell K. , Kim J. J. , Brisson M et al., Mortality Impact of Achieving WHO Cervical Cancer Elimination Targets: A Comparative Modelling Analysis in 78 Low-income and Lower-middle-income Countries, The Lancet. (February 2020) 395, no. 10224, 591–603, 10.1016/s 0140-6736(20)30157-4.PMC 704300632007142 · doi ↗ · pubmed ↗
- 5Cohen P. A. , Jhingran A. , Oaknin A. , and Denny L. , Cervical Cancer, The Lancet. (2019) 393, no. 10167, 169–182, 10.1016/S 0140-6736(18)32470-X, 2-s 2.0-85059683482.30638582 · doi ↗ · pubmed ↗
- 6Center for Disease Control and Prevention , HPV Vaccination Recommendations, 2021, https://www.cdc.gov/vaccines/vpd/hpv/hcp/recommendations.html.
- 7Gakidou E. , Nordhagen S. , and Obermeyer Z. , Coverage of Cervical Cancer Screening in 57 Countries: Low Average Levels and Large Inequalities, P Lo S Medicine. (2008) 5, no. 6, 0863–0868, 10.1371/journal.pmed.0050132, 2-s 2.0-46349083323.PMC 242994918563963 · doi ↗ · pubmed ↗
- 8Petersen Z. , Jaca A. , Ginindza T. G et al., Barriers to Uptake of Cervical Cancer Screening Services in Low-and-middle-income Countries: A Systematic Review, BMC Women′s Health. (2022) 22, no. 1, 10.1186/s 12905-022-02043-y.PMC 971669336461001 · doi ↗ · pubmed ↗