Universal Utilization of Optimally Timed First Obstetric Ultrasound Among Pregnant Women in a Low‐Middle Income Country: A Multicenter Prospective Study
Sisay Kirba, Abdulfetah Abdulkedir Abdosh, Ekram Muhammedasrar, Abraham Fessehaye Sium

TL;DR
This study found that about two-thirds of pregnant women in Ethiopia received optimally timed first obstetric ultrasounds, with private clinics and prior complications increasing the likelihood.
Contribution
The study provides new evidence on ultrasound utilization in low-middle income countries, focusing on Ethiopia.
Findings
Approximately 67.5% of pregnant women had optimally timed first obstetric ultrasounds.
Women starting antenatal care at private clinics were more likely to have timely ultrasounds.
Prior major obstetric complications increased the likelihood of timely ultrasound use.
Abstract
Currently, the World Health Organization guidelines recommend universal utilization of optimally timed first obstetric ultrasound (defined as ultrasound before 24 weeks) in low‐middle income countries. However, there is inadequate evidence on this topic from these countries. Our study aimed to determine the rate of utilization of optimally timed first obstetric ultrasound among pregnant women who gave birth at three public hospitals in Ethiopia. This was a multicenter prospective cross‐sectional study conducted on the utilization of optimally timed first obstetric ultrasound among pregnant women who delivered at public hospitals in Ethiopia in 2020. Data were collected prospectively using a structured questionnaire. Data were analyzed using SPSS Version 20. Simple descriptive statistics, chi‐squared test, and multiple regression analysis were performed as appropriate. p value less than…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
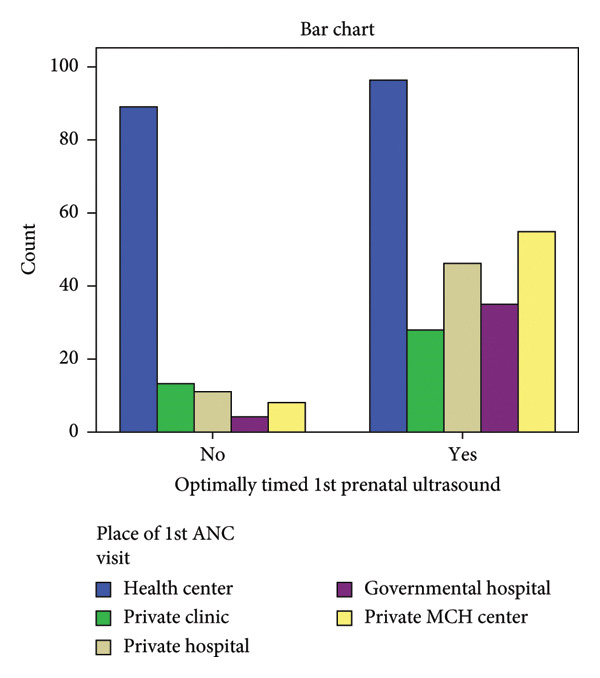 Figure 1
Figure 1| Variable | Number | Percent | |
|---|---|---|---|
| 1. Address | Addis Ababa | 293 | 76.1 |
| Outside Addis Ababa | 92 | 23.9 | |
| 2. Marital status | Single | 43 | 11.2 |
| Married | 342 | 88.8 | |
| 3. Religion | Orthodox Christian | 155 | 40.3 |
| Protestant Christian | 107 | 27.8 | |
| Muslim | 116 | 30.1 | |
| Other | 7 | 1.8 | |
| 4. Level of education | Uneducated | 55 | 14.3 |
| Completed primary school | 66 | 17.1 | |
| Completed secondary school | 107 | 27.8 | |
| College diploma | 91 | 23.6 | |
| College degree | 57 | 14.8 | |
| Master’s degree | 9 | 2.3 | |
| Doctorate degree | 0 | 0 | |
| 5. Employment status | Unemployed | 158 | 41 |
| Government employee | 153 | 39.7 | |
| Private employee | 59 | 15.3 | |
| Run self‐business | 15 | 3.9 | |
| 6. Total monthly income in birr | < 5000 | 95 | 24.7 |
| 5000–10,000 | 103 | 26.8 | |
| 10–20,000 | 161 | 41.8 | |
| 20–50,000 | 24 | 6.2 | |
| > 50,000 | 2 | 0.5 | |
| Variable | Number | Percent | |
|---|---|---|---|
| 1. Parity | Primigravid | 155 | 40.3 |
| Multigravid | 230 | 59.7 | |
| 2. Known health problems before this pregnancy | Yes | 187 | 48.5 |
| No | 198 | 51.5 | |
| 3. Health problems during this pregnancy | Yes | 220 | 57.1 |
| No | 165 | 42.9 | |
| 4. Previous history of major obstetric problem during pregnancy | Yes | 130 | 33.5 |
| No | 100 | 26.5 | |
| 5. Planned pregnancy | Yes | 311 | 80.8 |
| No | 74 | 19.2 | |
| 6. Place of 1st ANC visit | Health center | 185 | 48.1 |
| Private clinic | 41 | 10.6 | |
| Private hospital | 57 | 14.8 | |
| Government hospital | 39 | 10.1 | |
| Private MCH center | 63 | 16.4 | |
| Variable | No. | Percent | COR (95% CL) | AOR (95% CI) | |
|---|---|---|---|---|---|
| 1. Parity | Primigravid | 155 | 40.3 | 0.56 (0.2–1.08) | |
| Multigravid | 230 | 59.7 | 1 | ||
| 2. Known health problems before this pregnancy | Yes | 187 | 48.5 | 0.98 (0.6–1.4) | |
| No | 198 | 51.5 | 1 | ||
| 3. Health problems during this pregnancy | Yes | 220 | 57.1 | 0.8 (0.5–1.3) | |
| No | 165 | 42.9 | 1 | ||
| 4. Previous history of major obstetric problem during pregnancy | Yes | 130 | 33.5 | 6.6 (3.5–12.2) | 5.2 (2.7–9.9) |
| No | 100 | 26.5 | 1 | 1 | |
| 5. Planned pregnancy | Yes | 311 | 80.8 | 1.1 (0.6–1.9) | |
| No | 74 | 19.2 | 1 | ||
| 6. Place of 1st ANC visit | Health center | 185 | 48.1 | 1 | 1 |
| Private clinic | 41 | 10.6 | 1.99 (0.9–4) | 1.7 (0.8–3.7) | |
| Private hospital | 57 | 14.8 | 3.8 (1.8–7.9) | 3.2 (1.5–6.8) | |
| Government hospital | 39 | 10.1 | 8.1 (2.7–23.7) | 7.4 (2.5–22.3) | |
| Private MCH center | 63 | 16.4 | 6.3 (2.8–14) | 4.9 (2.1–11.2) | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUltrasound in Clinical Applications · Pregnancy and preeclampsia studies · Global Maternal and Child Health
1. Introduction
Antenatal care (ANC) is a basic health care that is provided to pregnant mothers during pregnancy. ANC is a time proven important tool that decreases fetomaternal morbidity and mortality [1]. It has three core scopes: early detection of risks that increase morbidity and mortality both in the fetus and the mother, preventing and managing pregnancy‐related complications with treatments and immunizations, and promoting health through nutrition guidance, lifestyle modification, and education on birth preparedness and danger signs [2]. In the first scope, elevated risk is identified by basic history and physical examination and by doing some basic and some specialized investigation [3]. This is very important objective of ANC, and it is preferably to be done as early in the pregnancy as possible so that the pregnant mother can get specialized care that minimizes the increased morbidity and mortality in the fetomaternal condition. The other reason it has to be done as early as possible is that in the event of fetal conditions that have no acceptable and available therapy and or fetal conditions that are lethal, pregnancy termination can be provided safely [4]. This is also important in the event of maternal conditions which are worsened by pregnancy and endangering the life of the mother [5]. Evaluations and workups done early in pregnancy are classified as basic and specialized [6].
The woman that needs specialized care is identified by appropriate history and physical examination and baseline workup [7]. Among the basic evaluations that should be carried out early during the course of the pregnancy is obstetric ultrasound (US). Obstetric US early in the pregnancy has basic objective of dating the pregnancy, localizing the pregnancy, and assessing the viability of the pregnancy. Another simple noninvasive diagnostic evaluation during ANC is doing fetal anatomic scanning. Fetal anatomic scan can diagnose most of the major congenital anomalies when done at the appropriate GA (18–20 weeks) [8, 9]. In its latest recommendation, WHO recommends all pregnant woman should have the first obstetric US before 24 weeks [5].
In Ethiopia, the first ANC visit is usually done at health centers, and the risk identification evaluation and workup are done by obstetric healthcare providers at health centers who are almost always midwives, health officers, or nurses [7, 10–12].
In the current practice in Addis Ababa (the capital city of Ethiopia), early obstetric US is mostly done by obstetricians and radiologists. Although multiple studies have documented the timing of first ANC follow‐up and the quality of ANC follow‐up [13–17], there is no prior study that looked into the utilization of optimally timed first obstetric US among Ethiopian pregnant women. The objective of this study was to determine the mean timing of first obstetric US among pregnant women who attended ANC at the abovementioned public hospitals and factors associated with late timing of first obstetric US (first US beyond 24 weeks of gestation).
2. Methods
2.1. Study Design, Setting, and Period
This was a cross‐sectional study conducted on the timing of first obstetric US among women who gave birth at three public hospitals (St. Paul’s Hospital Millennium Medical College [SPHMMC], Ras Desta Damtu Hospital, and Menellik‐II hospital) in Addis Ababa, Ethiopia. The study was conducted over a period of 3 months (October to December 2020). SPHMMC is a leading medical college in Ethiopia that provides various specialty and subspecialty care and training in Ethiopia. The Department of Obstetrics and Gynecology at this hospital runs the biggest maternal–fetal medicine unit in the country providing advanced care for high‐risk pregnant women including screening for congenital anomalies, genetic counseling and testing, and fetal diagnostic and therapeutic interventions including intrauterine transfusion. The other two hospitals (study sites) are affiliates of St. Paul’s Hospital, and the majority of the obstetric service deliveries at these hospitals are carried out by SPHMMC Ob‐Gyn residents and faculty.
We included both high‐risk and low‐risk pregnant women who had their deliveries attended at the three public hospitals and volunteered to participate in the study. We excluded those with incomplete data and missing key variables (such as timing of first US, undocumented status of presence of prior serious medical conditions, and undocumented place of first ANC contact).
2.2. Sample Size and Sampling Procedure
Using single proportion formula by assuming a 50% prevalence of optimally timed first obstetric US, 5% error of margin, and 95% confidence interval, the calculated sample size was N = 385. No systematic sampling technique was employed.
2.3. Data Collection
Data were collected using a structured questionnaire prepared in English. The questionnaire was pretested before data collection and modified accordingly. We collected sociodemographic data and obstetric characteristics including timing of first obstetric US.
2.4. Data Analysis
Data were analyzed using SPSS 20 statistical software. Simple descriptive statistics with mean and SD were used for numerical variables. Bivariate regression analysis was carried out, and variables with p value less than 0.2 (considered potential confounders) were entered into multivariate regression analysis; factors associated with late timing (which is not optimal timing) of first obstetric US were further analyzed. p value less than 0.05 and adjusted odds ratio (AOR) with 95% CI were used to present result significance.
2.5. Ethical Consideration
This research was approved by the Ethical Review Committee of SPHMMC with Ref. No. PM23/232. Written informed consent was obtained from study participants. Confidentiality and data anonymity were maintained throughout the data collection.
3. Results
A total of 385 women were included in the final analysis. The mean gestational age for the 1^st^ ANC was 3.1 months with SD of 1.3. Approximately 67.5% of pregnant mothers had optimally timed 1^st^ US (32.5% of pregnant mothers did not have optimally timed 1^st^ prenatal US).
The mean age of respondents was 28.3 years with the youngest age being 18 years and the oldest being 40 years (Table 1). From the study participants, 76.1% of them were from Addis Ababa and 23.9% were from outside Addis Ababa. When it comes to educational status, 14.3% of respondents did not go to school while 41% were unemployed. Approximately 40.3% of the pregnant mothers were primigravida. The majority (48.1%) of respondents started their ANC at health centers (Table 2).
From pregnant mothers who started their ANC at health centers, 48.1% did not have optimally timed 1^st^ prenatal US (Figure 1). 87.3% of those who started their ANC at private MCH centers and 89.7% of those who started their ANC at government hospitals had optimally timed 1^st^ prenatal US.
Proportion of optimally dated first ultrasound utilization according to place of 1st prenatal contact.
Multivariate regression analysis (Table 3) revealed that first place of ANC and the presence of prior major obstetric problem in prior pregnancies were associated with optimal timing of 1^st^ prenatal US. Compared to those having ANC at health centers, those who started their ANC at private clinic were 1.7 times (95 CI: 1.8–7.9) more likely to have optimally timed ANC. Those who had their 1^st^ ANC at private hospital were 3.2 times (95 CI: 1.8–7.9) more likely to have optimally timed 1^st^ prenatal care. Those who had their first ANC at private health institutions and government hospitals were much more likely to have optimally timed 1^st^ prenatal US with the following AOR for government hospital and private MCH centers: AOR = 7.4 (95 CI: 2.7–23) and AOR = 4.9 (95 CI: 2.8–14.1), respectively. Those who had previous major obstetric problem were 5.2 times (95 CI: 2.7–9.9) more likely to have optimally timed US than those without major previous obstetric problem.
4. Discussion
The primary objective this study was to determine the proportion of pregnant women who had optimal timing of first prenatal obstetric US and factors associated with it. We found that only two‐third of the study participants had optimally timed 1^st^ obstetric US. Place of first ANC contact (women who had their first ANC contact in private and government hospitals) and the presence of prior major obstetric problem were associated with optimally timed 1^st^ obstetric US.
WHO recommends every pregnant woman should have the 1^st^ obstetric US before 6^th^ month which corresponds to 24 weeks [18]. This criterion is clear and easy to implement as most of pregnant mothers in low‐middle income countries like Ethiopia count the duration of the pregnancy in months and most have difficulty remembering it in weeks. In our study, although most (67.5%) participants in our study had optimally timed 1^st^ US, significant number of mothers (32.5%) had no optimally timed 1^st^ prenatal US. This finding is similar to the findings of prior similar study conducted in Canada by Abdullah et al. [1]. However, there is difference between the two studies in the definition of optimally timed 1^st^ obstetric US: while Abdullah et al. defined optimally timed US as an US done between 11 and 22 weeks based on Society of Obstetricians and Gynaecologists of Canada (SOGC) recommendation, we defined optimally timed 1^st^ US based on WHO recommendation as an US done before 6^th^ month in our study. Although we could not compare our findings to the findings from other similar studies conducted in Africa, as there are no prior studies that looked into optimally timed first obstetric US as primary outcome, our main finding (one‐third of the participants did not utilize optimally timed first obstetric US) is alarming. Suprisingly, obstetric US services are available, free of charge, at public health institutions in Addis Ababa, where our study was conducted. We recommend proactive measures to be taken at different levels for improving early obstetric US utilization, including at patient level through creating awareness on the importance of having optimally timed first obstetric US.
Currently, there is strong evidence that supports the importance of US in enhancing fetomaternal health during pregnancy in low‐middle income countries [19, 20]. However, in most parts of the world, antenatal US is available only to a privileged few in urban centers, while the majority of the population living in rural areas have little or no access to diagnostic imaging services [21]. In Africa, a moderate utilization of obstetric US among pregnant mothers is on an increasing trend only after 2020 with patients’ good knowledge being among the factors associated with good utilization [22]. According to Ethiopia Demographic Health Survey (EDHS) 2019, 74% of women aged 15–49 with a live birth in the 5 years before the survey received ANC from a skilled provider for their most recent birth [23]. A study on utilization of prenatal US among pregnant women in public health institution in Ethiopia showed that 60.7% used prenatal US during their pregnancy [24]. Another similar study conducted in the capital Addis Ababa (Ethiopia) in public health institution showed that the utilization of prenatal US among pregnant women was 70.3% [25]. In the present study, of the factors which significantly affected the timing of optimally timed 1^st^ prenatal is the place of 1^st^ ANC: compared to those who started their ANC at health centers, those who started their ANC at private clinic were 1.7 times (95% CI: 1.8–7.9) more likely to have optimally timed ANC. Those who had their 1^st^ ANC at private hospital were 3.2 times (95% CI: 1.8–7.9) more likely to have optimally timed 1^st^ US. Similarly, those that had first ANC at government hospital (AOR = 7.4, 95% CI: 2.7–23) and private MCH centers (AOR = 4.9, 95% CI: 2.8–14.1) were more likely to utilize optimally dated first US.
Being among the first studies to report data on optimally dated first obstetric US from low‐income countries with proper sample size allocation and muticenter study design are the strengths of our study. Lack of random sampling technique and comparative analysis of perinatal outcomes between those who had optimally dated first obstetric US and those had are the main limitations of our study. The other limitation of this study is not considering the prevalence (p) in other international studies during sample size calculation, though there are no similar local or regional studies.
5. Conclusion
In this study, we found that one‐third of pregnant women did not utilize optimally timed first obstetric US despite obstetric US services being available at public health institutions. Place of first ANC contact and presence of prior major obstetric complication were associated with utilization of optimally dated first obstetric US. This findings demonstrates that availing US services alone even at no charge is not effective in ensuring universal utilization of early US by pregnant women unless and otherwise it is complemented with elevating patients’ awareness on the importance of having optimally dated obstetric US and improving practice of recommending early US by prenatal providers mainly midlevel health professionals, as they share a significant burden of providing ANC in public institutions in low‐middle income countries.
Disclosure
All authors critically revised the article for intellectual content and gave final approval for submission for publication.
Conflicts of Interest
The authors declare no conflicts of interest.
Author Contributions
S.K. and A.A.A. were responsible for conception and development of the study project. S.K. and A.A.A. were responsible for data collection and data analysis. A.F.S., S.K., and E.M. were responsible for manuscript write‐up. The final manuscript was edited by A.F.S.
Funding
No funding was received for this study.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abdullah , Landy C. K. , Mc Cague H. , Macpherson A. , and Tamim H. , Factors Associated with the Timing of the First Prenatal Ultrasound in Canada, BMC Pregnancy and Childbirth. (2019) 19, no. 1, 10.1186/s 12884-019-2309-4, 2-s 2.0-85065605473.PMC 650985931077167 · doi ↗ · pubmed ↗
- 2Mc Cauley H. , Lowe K. , Furtado N. , Mangiaterra V. , and van den Broek N. , What are the Essential Components of Antenatal Care? A Systematic Review of the Literature and Development of Signal Functions to Guide Monitoring and Evaluation, BJOG: An International Journal of Obstetrics and Gynaecology. (2022) 129, no. 6, 855–867, 10.1111/1471-0528.17029.34839568 · doi ↗ · pubmed ↗
- 3Timing of First Antenatal Care Attendance and Associated Factors Among Pregnant Women in Arba Minch Town and Arba Minch District, Gamo Gofa Zone, South Ethiopia, 2015, Hindawi.10.1155/2015/971506 PMC 462025326543485 · doi ↗ · pubmed ↗
- 4Late Initiation of Antenatal Care and Associated Factors Among Pregnant Women in Addis Zemen Primary Hospital, South Gondar, Ethiopia, Reproductive health journal. (2019) .10.1186/s 12978-019-0745-2PMC 654498231151402 · doi ↗ · pubmed ↗
- 5WHO Handbook for Guideline Development, 2014, World Health Organization, http://www.who.int/kms/handbook_2nd_ed.pdf.
- 6WHO, Trends in Maternal Mortality 1990–2013, Estimates by WHO, UNICEF, UNFPA, the World Bank, and the United Nations Population Division, 2014, World Health Organization.
- 7Timing of First Antenatal Care Visit and its Associated Factors Among Pregnant Women Attending Public Health Facilities in Addis Ababa, Ethiopia, 2017, EJHS.10.4314/ejhs.v 27i 2.6PMC 544082828579709 · doi ↗ · pubmed ↗
- 8Al Suwaidi H. H. , Abdelhalem R. M. , and Agten A. K. , The Fetal Anomaly Screening Scan: an International Perspective, Obstetrics, Gynaecology and Reproductive Medicine. (2024) 34, no. 8, 213–217, 10.1016/j.ogrm.2024.05.002. · doi ↗