A meta-analysis of the effects of dual-task training on cognitive function in stroke patients
Ruolin Shi, Weibo Li, Xiaolu Liu, Zengxin Sun, Xinjing Ge, Peiyuan Lv, Yu Yin

TL;DR
This study finds that dual-task training improves cognitive function in stroke patients more than usual care, but results depend on training duration and study quality.
Contribution
The paper provides a meta-analysis showing dual-task training's cognitive benefits in stroke patients, with insights on duration effects.
Findings
Dual-task training significantly improved mini-mental state examination scores compared to controls.
Longer intervention durations (>4-6 weeks) led to better performance in memory and attention tests.
Improvements were observed in both patients with and without significant cognitive deficits post-stroke.
Abstract
Post-stroke cognitive impairment (PSCI) affects ~40% of survivors, hindering recovery. Dual-task training (combining cognitive and motor tasks) may help, but its superiority over single-task training or usual care remains unclear. This study examines whether dual-task training improves cognitive function more than (1) single-task training or (2) usual rehab/control, and whether effects vary by intervention duration. Keywords were used to search Chinese and English databases. The search period was up to 15 October 2023. Randomized controlled trial (RCT) studies comparing the effects of dual-task training and single-task training or blank control on improving cognitive impairment in stroke patients were included and the quality of the included studies was evaluated using the Cochrane collaboration’s risk assessment tool. The effect indicators were evaluated based on fixed-effects or…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
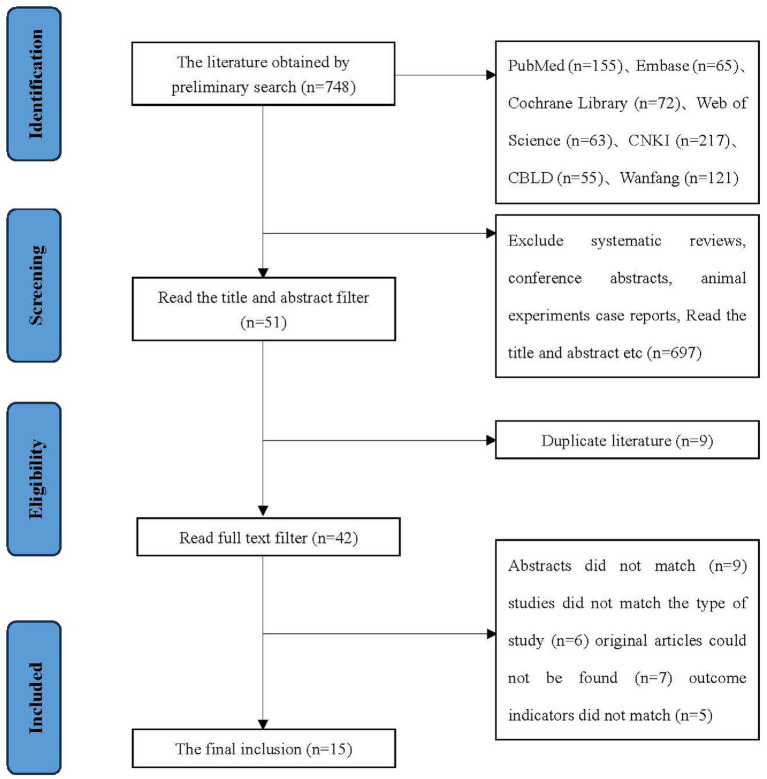 Figure 1
Figure 1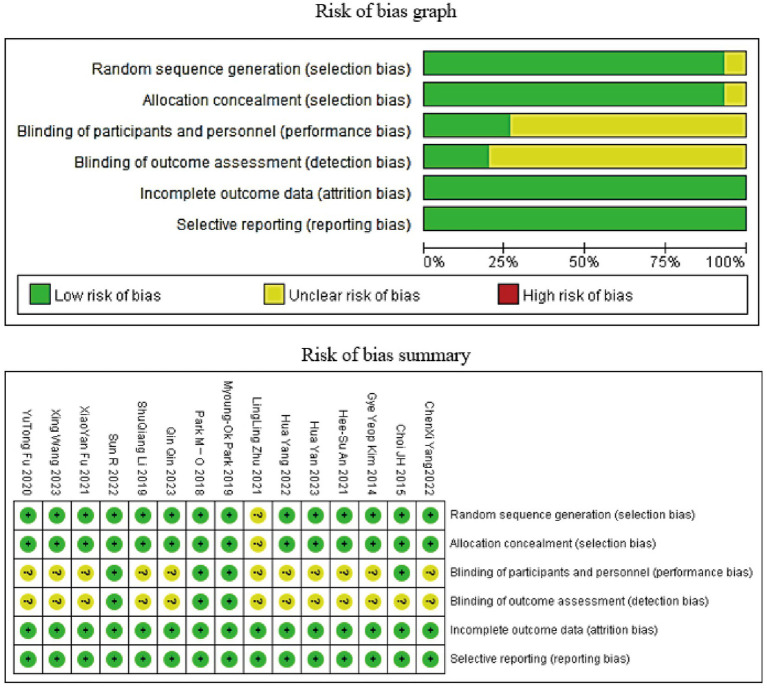 Figure 2
Figure 2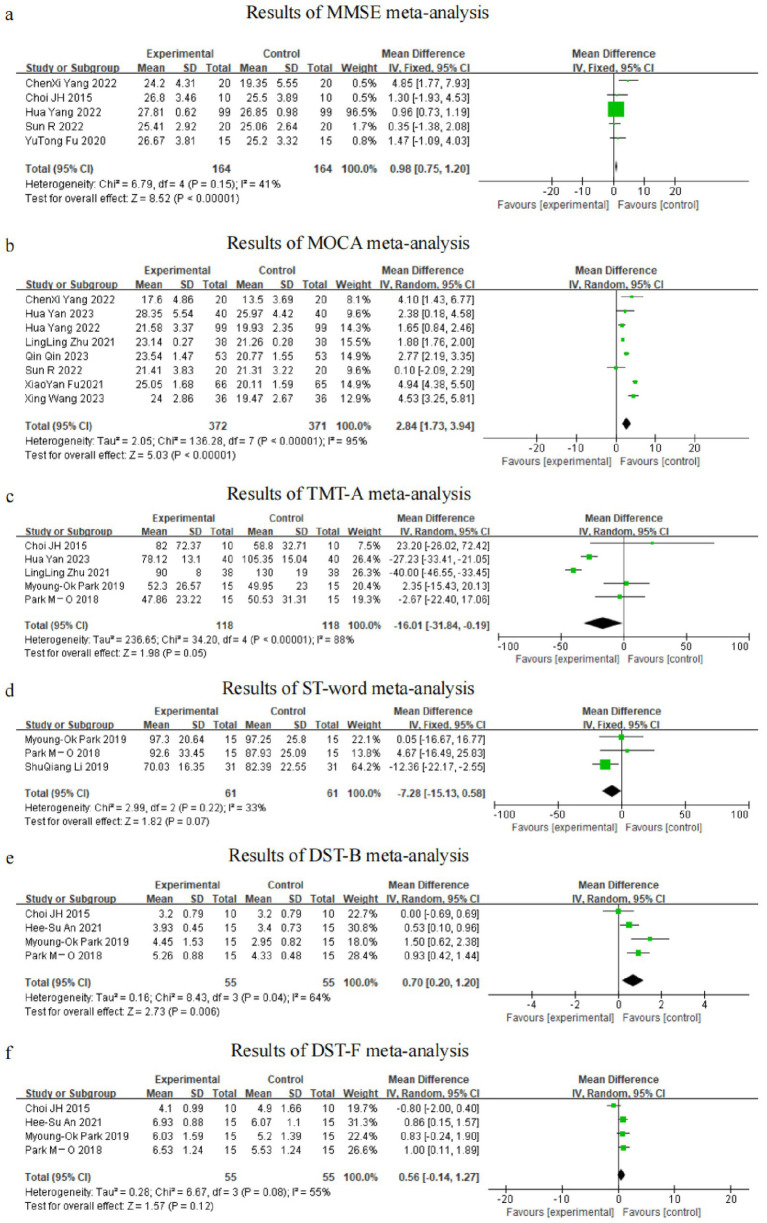 Figure 3
Figure 3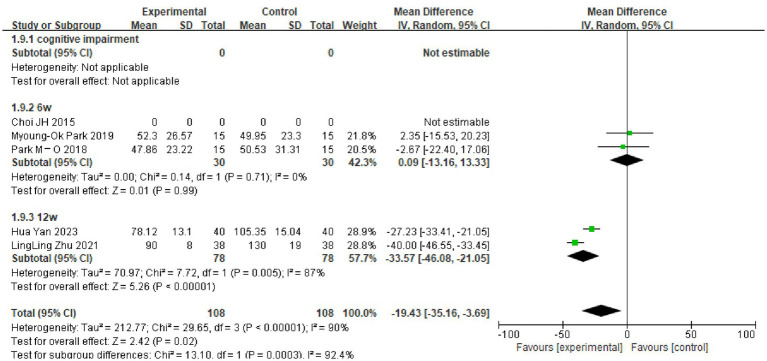 Figure 4
Figure 4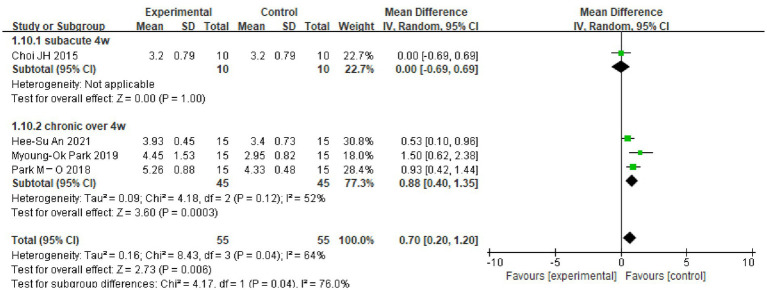 Figure 5
Figure 5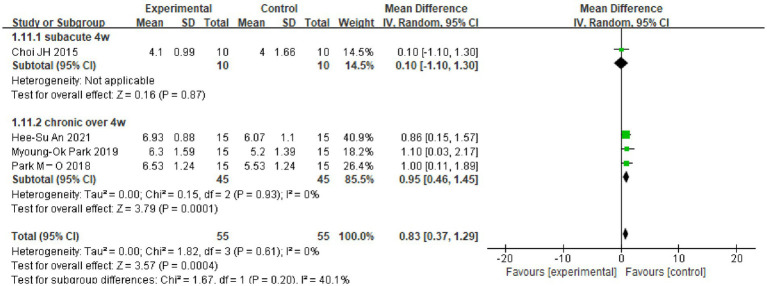 Figure 6
Figure 6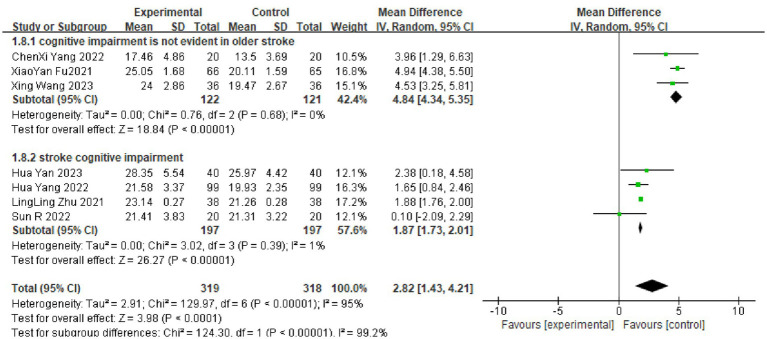 Figure 7
Figure 7| Scale | Domains assessed | Score range/cut-off | Interpretation | References |
|---|---|---|---|---|
| Mini-Mental State Examination (MMSE) | Orientation, memory, attention, language, visuospatial | 0–30; < 24 indicates cognitive impairment | Global cognitive screening | ( |
| Montreal Cognitive Assessment (MoCA) | Executive function, memory, language, visuospatial, attention | 0–30; < 26 indicates mild cognitive impairment | More sensitive than MMSE for mild deficits | ( |
| Trail Making Test-A (TMT-A) | Processing speed, visual attention | Time to completion (seconds); higher = worse | Measures cognitive flexibility and attention | ( |
| Stroop Color–Word Test (word sub-task) | Selective attention, inhibition | Seconds or errors; higher = worse | Assesses executive inhibition | ( |
| Digit Span Test-Backward (DST-B) | Working memory | 0–14 digits recalled; higher = better | Verbal working memory capacity | ( |
| Digit Span Test-Forward (DST-F) | Short-term memory | 0–16 digits recalled; higher = better | Verbal short-term memory | ( |
| Inclusion of studies | Sample size | Intervention | Frequency | Times | Outcome indicator | ||
|---|---|---|---|---|---|---|---|
| EG | CG | CG | EG | ||||
| Wang et al. ( | 36 | 36 | Routine rehabilitation and proprioceptive training | Cognitive-motor dual-task training. | 40 min/times, 5 times/w | 8w | MoCA |
| Fu et al. ( | 66 | 65 | Repetitive transcranial magnetic stimulation and basic cognitive training | Addition of cognitive-motor control dual-task training to control group treatment | rTMS:15 ~ 20 min, Once a day, 4–5 days a week exercise: Once a day for an hour. | 4w | MoCA, Rivermead Behavioural Memory Test (RBMT) |
| Yan ( | 40 | 40 | Resistance-based rehabilitation | Addition of cognitive-motor control dual-task training to control group treatment | 30 min at a time, once a day, 5 times a week | 12w | MoCA, Trail Marking Test (TMT) |
| Yang ( | 99 | 99 | Dual Task Training Therapy | Trained in hyperbaric-assisted dual-tasking | One hour at a time, once a day, 5 times a week | 4w | MMSE, MoCA |
| Yang and Wang ( | 20 | 20 | Routine single-task rehabilitation | Cognitive-motor dual-task training | 2 times a day, 5 times a week | 2w | MMSE, MoCA, DS, SDMT, TMT-A |
| Qin et al. ( | 53 | 53 | Routine treatment and routine neurosurgical care | Cognitive-Otago motor control dual task training | 90 min a day, once a day, 7 times a week | 90d | MoCA |
| Zhu et al. ( | 38 | 38 | Health education and routine treatment | Perform a simplified version of Otago’s cognitive-motor dual-task training that combines movement and music. | One hour at a time. 2 times per week | 90d | MoCA-BJ and Trail Marking Test, (TMT-A) |
| Fu et al. ( | 15 | 15 | General rehabilitation training such as balance, | Dual-task training | 6 times/week, 40–50 min/time. | 3w | MMSE |
| Li et al. ( | 31 | 31 | Exercise Rehabilitation Therapy and Cognitive Rehabilitation Training | Motor rehabilitation therapy and cognitive rehabilitation dual-task training plus AMST training: using an interactive metronome | 3 times per week, 30 min/trip. | 6w | TMT, Digital Span Test (DST), Stroop test |
| Kim et al. ( | 10 | 10 | Routine rehabilitation training | Dual-task gait training and cognitive tasks | 5 days a week | 4 w | Stroop test |
| Choi et al. ( | 10 | 10 | Balance training with balance boards | Dual Task is simultaneous balance and cognitive training using BioRescue | 30 min per day, 5 days per week, | 4w | MMSE |
| Park and Lee ( | 15 | 15 | Only 3 CMDTs per week | Received CMDT + AMST 3 times per week | 3 times per week | 6w | TMT, DST, Stroop test (ST) |
| An and Kim ( | 15 | 15 | Perform 20 min of single-task training and receive 10 min of regular occupational therapy | 20 min of dual-task training and receive 10 min of regular occupational therapy | 30 min each time, 5 times a week | 5w | DST-B, DST-F, EFPT-K, K-TMT-e B |
| Park and Lee ( | 15 | 15 | Traditional occupational therapy | Dual-task training using different cognitive tests | 18 interventions of 30 min each, 3 times per week | 6w | TMT-A, TMT-B DST-F, DST-B, Stroop test (ST) |
| Sun et al. ( | 20 | 20 | Individualised multi-disciplinary progressive training programme | Patients in the CMDT group received both cognitive and motor training | Complete 40 min of training per day, 5 days per week | 4w | MMSE, MoCA |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsStroke Rehabilitation and Recovery · Spatial Neglect and Hemispheric Dysfunction · Older Adults Driving Studies
Introduction
As one of the common chronic diseases, stroke has an acute onset, progresses rapidly and leaves behind various degrees of functional impairment, bringing a significant burden to the patient’s family and even society (1). Research suggests that around 40% of stroke patients will have cognitive impairment (2). Cognitive dysfunction following a stroke affects progress in rehabilitation of other functions and increases the difficulty of care and rehabilitation at home and in hospitals (3).
Currently, conventional cognitive training and exercise aerobic training are inefficient because they require an exclusive programme tailored to the patient’s own medical characteristics (4). Kumar et al. (5) showed that the transcranial magnetic stimulation technique can help in post-stroke cognitive deficits by modulating the functional areas of the patient’s brain through cortical stimulation, but the therapeutic effect is unstable. Computer-assisted cognitive training and virtual reality technology are not widely used in clinical applications due to their need for a certain amount of capital investment.
Dual-task training is a new training modality applied to stroke patients in recent years, which involves performing one functional training task along with two or more other tasks (6). Studies by Choi et al. (7) and De Luca et al. (8) suggest that a dual task of cognitive–motor training combined with audio synchronization may be more effective in improving attention, cognitive flexibility and executive performance.
Previous systematic reviews have examined dual-task training primarily for its impact on motor outcomes, such as gait parameters (9) or combined motor–cognitive effects (10). These reviews focused on motor function rather than cognitive recovery per se, and none specifically isolated the cognitive benefits of dual-task training versus single-task or usual care in stroke survivors. However, the current study does not analyze single-task training or blank control studies separately to clarify whether the effect of dual-task training is superior to single-task training or to a blank control. The purpose of this study is to investigate whether dual-task training is better than single-task training and blank control in improving cognitive impairment in stroke patients using a meta-analysis. The aim is to provide an evidence-based reference for clinical, dual-task training in the treatment of cognitive dysfunction in stroke patients.
Stroke phase was not an exclusion criterion. Seven of the 15 included trials enrolled participants in the subacute phase (<6 months post-stroke), three recruited chronic patients (>6 months) and five did not specify disease duration. We deliberately retained studies across all phases because (1) the overall literature pool was small and further exclusion would compromise statistical power and generalisability, and (2) our primary objective was to determine whether cognitive–motor dual-task training improves cognitive outcomes relative to usual care or single-task training irrespective of stroke chronicity. Nevertheless, the predominance of participants at a subacute phase should be noted as this window is considered critical for cognitive recovery.
Methods
Literature search
The search strategy followed the PRISMA 2020 statement. Computer searches were conducted using the PubMed, Embase, Cochrane Library, Web of Science, China National Knowledge Infrastructure, China Biomedical Literature Database and Wanfang Data databases. The search was available until June 1, 2023, in both Chinese and English. The intervention was dual-task training, the disease type was stroke and the study type was randomized controlled trials (RCTs). The search strategy included both the Chinese and the English languages.
The search terms were as follows: (Strokes OR Cerebrovascular Apoplexy OR Apoplexy, Cerebrovascular OR Cerebrovascular Stroke OR Cerebrovascular Strokes OR Stroke, Cerebrovascular OR Strokes, Cerebrovascular OR Apoplexy OR Cerebral Stroke OR Cerebral Strokes OR Stroke, Cerebral OR Strokes, Cerebral) AND (Cognitions OR Cognitive Function OR Cognitive Functions OR Function, Cognitive OR Functions, Cognitive) AND (dual task OR dual-task OR cognitive task OR cognitive-task OR concurrent task OR cognitive motor OR cognitive-motor OR motor cognitive OR motor-cognitive OR second task OR additional task).
Inclusion and exclusion criteria
The inclusion criteria were as follows:
Participants: Diagnosed with stroke and confirmed by computed tomography or magnetic resonance imaging; age and gender were not limited.Intervention: Dual-task training (including a cognitive task) in the experimental group.Control: Other conventional rehabilitation treatments, also combined with physical physiological factor therapy.Outcome indicators: These included the mini-mental state examination (MMSE) (11), Montreal Cognitive Assessment (MoCA) (11), Trail Making Test-A (TMT-A), Stroop Color and Word Test (SCWT) and Digit Span Test (DST). For details see Table 1 (11–15).Research method: RCT.Language: Chinese and English.
The exclusion criteria included the following:
Conference papers.Inability to extract valid ending data from the text.Duplicate literature.Systematic reviews.
Seven records were excluded because their full texts could not be accessed. These comprised conference abstracts with image-only PDFs lacking selectable text, subscription-protected journal articles for which our library has no license, one Wanfang Data record with a URL that returned a persistent 404 error, a Journal of Physical Therapy Science paper with an online appendix hosting the required data that was no longer available and two Korean conference papers that were only available in print.
Literature screening and data extraction
Two investigators independently screened the literature, extracted data and cross-checked against the inclusion and exclusion criteria. If disagreements emerged, they were resolved through discussion or negotiation with a third party. Data extracted in this meta-analysis included title, first author, year of publication, sample size, intervention, duration of intervention and relevant outcome indicators.
Literature quality evaluation
Two researchers independently assessed the risk of bias of the included studies using the Cochrane-recommended RCT risk of bias assessment tool and cross-checked the results. The evaluation items of the tool include the following seven areas: generation of randomized sequences; allocation concealment; blinding of participants and implementers; blinding of outcome assessments; completeness of outcome data; selective reporting of findings; and other sources of bias (other sources of bias items were excluded from this study).
Statistical analysis
The data included in the study were quantitatively analyzed using RevMan v5.4 software. Successive results in the same units were analyzed using mean difference (MD); in all other cases, standardised mean difference (SMD) was used. Uncertainties are presented as 95% confidence intervals (95%CI). Heterogeneity was assessed using I^2^; for I^2^ ≤ 50%, p ≥ 0.1, heterogeneity was small and a fixed-effects model was used; for I^2^ > 50%, p < 0.1, a random-effects model was used; and for I^2^ > 75%, p < 0.1, heterogeneity was large and sensitivity or subgroup analysis was used. The Egger and Begg tests were used for publication bias. The level of significance α = 0.05. The sample size of this study was less than 10 articles, meaning only subjective publication bias analysis was conducted.
Results
Literature screening process and results
A total of 748 pieces of related literature were obtained, and 15 articles were finally included by screening the literature quality, language, type, title, abstract, outcome indicators, duplication or not and access to the original text. The literature screening process and results are shown in Figure 1.
Literature screening process.
Basic characteristics of included studies and risk of bias results
The basic characteristics of the included studies are shown in Table 2 (16–30). The Cochrane risk of bias assessment tool was used to evaluate the quality of the literature, with the results shown in Figure 2.
Cochrane risk of bias assessment results map.
Meta-analyzes results
A total of five RCTs used the MMSE as an outcome indicator, including 328 patients. Since I^2^ = 41%, a fixed-effects model was selected for meta-analysis, which showed better improvement in MMSE scores in the dual-task group relative to the control group (MD = 0.98, 95%CI: 0.75, 1.20, p < 0.0001) (see Figure 3a).
Graph of meta-analysis results (a) MMSE, (b) MOCA, (c) TMT-A, (d) ST-word, (e) DST-B, (f) DST-F.
A total of eight RCTs used the MoCA as an outcome indicator, including 743 patients. Given that I^2^ = 95%, with large heterogeneity among the results, a random-effects model was used for meta-analysis. The results showed higher scores in the dual-task group compared with the control group (MD = 2.84, 95%CI: 1.73, 3.94, p < 0.0001) (see Figure 3b).
A total of five RCTs used the TMT-A trial as an outcome indicator, including 236 patients. Since I^2^ = 88%, with large heterogeneity among the results, a random-effects model was used for meta-analysis. The results showed better improvement in the dual-task group compared with the control group (MD = −16.01, 95%CI: −31.84, −0.19, p = 0.05) (see Figure 3c).
A total of three RCTs used the ST-word test as an outcome indicator, including 122 patients. Given that I^2^ = 33%, a fixed-effects model was chosen for meta-analysis, which showed that there was no significant difference in ST-word test scores of the dual-tasking group relative to the control group (MD = −7.28, 95%CI: −15.13, 0.58, p = 0.07) (see Figure 3d).
A total of four RCT trials used the DST-backward (DST-B) test as an outcome indicator, including 110 patients. Since I^2^ = 64%, a random-effects model was selected for meta-analysis, which showed that there was a significant difference in DST-B scores of the dual-tasking group relative to the control group (MD = 0.70, 95%CI: 0.20, 1.20, p = 0.006) (see Figure 3e).
A total of four RCTs used the DST-forward (DST-F) test as an outcome indicator, including 110 patients. Here, I^2^ = 55%, and a random-effects model was thus used for meta-analysis, which showed no significant difference in DST-F scores of the dual-tasking group relative to the control group (MD = 0.56, 95%CI: −0.14, 1.27, p = 0.12) (see Figure 3f).
Subgroup analysis
Due to the high heterogeneity of the results for the MoCA scores (I^2^ = 95%), the TMT-A test (I^2^ = 88%) and the DSTs (I^2^ = 64%, I^2^ = 55%), the sources of heterogeneity were further analyzed to consider possible reasons, such as the type of disease, the degree of cognitive impairment, the duration of the disease and the timing of the intervention. The TMT-A and DSTs were analyzed in subgroups according to the duration of the dual-task intervention, and the MoCA scores were analyzed in subgroups according to the type of disease and the degree of cognitive impairment. The results showed the following. (1) There was no significant difference in TMT-A scores between the dual-task group and the control group at 6 weeks of intervention time (MD = 0.09, 95%CI: −13.16, 13.33, p = 0.99), but at >6 weeks of intervention time (MD = −33.57, 95%C1: −46.08, −21.05, p < 0.00001), the TMT-A scores were lower compared with the control group (see Figure 4). (2) The dual-task group had a significant difference in DST-B scores compared with the control group after >4 weeks of intervention (MD = 0.88, 95%CI: 0.40, 1.35, p = 0.0003) (see Figure 5). (3) The dual-task group had a significant difference in DST-F scores compared with the control group after >4 weeks of intervention (MD = 0.95, 95%CI: 0.46, 1.45, p = 0.0001) (see Figure 6). (4) In elderly patients with minor cognitive impairment post-stroke, there was a significant difference in the MoCA score dual-task group compared with the control group (MD = 4.84, 95%CI: 4.34, 5.35, p < 0.00001). In patients with significant cognitive impairment post-stroke, the MoCA score was higher in the dual-task group compared with the control group (MD = 1.87, 95%CI: 1.73, 2.01, p < 0.00001) (see Figure 7).
Graph of the results of TMT-A subgroup analyzes.
Plot of DST-B test subgroup analysis results.
Plot of DST-F test subgroup analysis results.
Graph of results of MOCA scale subgroup analyzes.
Publication bias
When there are fewer than 10 included studies for meta-analysis of outcome metrics, publication bias analyzes using funnel plots are not recommended, and only subjective publication bias analyzes were, therefore, performed. The small sample size of the included RCTs in this study may have led to a greater risk of publication bias. The inclusion of studies in Chinese and English only, and the exclusion of studies in other languages may also have resulted in some publication bias.
Discussion
This meta-analysis shows that cognitive–motor dual-task training consistently improves global cognition, executive function and working memory in stroke survivors compared with usual rehabilitation or single-task training, with benefits becoming apparent after 4–6 weeks of intervention.
Post-stroke cognitive impairment (PSCI) is an important cause of long-term disability and reduced quality of life in stroke patients, with approximately half of patients experiencing cognitive impairment in the first year following a stroke (31). Impairments may affect multiple cognitive domains, including information processing, working memory, executive functioning and attention (32, 33). Currently, medication and rehabilitation are the main clinical treatments for cognitive decline associated with PSCI (34). The effects of dual-task training on PSCI were examined. Due to the small sample size and the lack of clarity regarding the results of the intervention, this study aimed to clarify the therapeutic effect of dual-task training on PSCI.
The results of the meta-analyzes showed significant differences in MMSE scores, MoCA scores, TMT-A test scores and DST-B scores in the dual-task group compared with the conventional group. This suggests that cognitive–motor dual-task training is more effective than conventional cognitive training in improving cognitive deficits post-stroke.
The MoCA scale is suitable for screening for mild cognitive impairment post-stroke and has a good ability to detect aspects of executive functioning that are consistent with the cognitive impairment characteristics of PSCI (35). The MMSE is comparable to the MoCA scale for the detection of PSCI, but the MMSE lacks sensitivity for the detection of mild cognitive dysfunction (36) and does not cover a comprehensive enough cognitive domain (37). This study found that both dual-task groups scored better than the control group. It has been shown that the main mechanism of PSCI is caused by stroke leading to lesions such as microhaemorrhage and edema in key areas, such as the hippocampus or cerebral white matter, which causes disruption of neuronal synaptic structure and function in brain regions (38). Park and Lee (27) showed that cognitive–motor dual-task training shortened the reaction time of central nervous system neurons and significantly increased the oxygenation rate of the frontal lobe, thereby improving cognitive performance.
Learning memory impairment is the main symptom of impaired cognitive function post-stroke (39). The DST is commonly used to measure verbal short-term memory and working memory. Studies have applied cognitive–motor dual-task training to the functional training of stroke patients and found that this method not only improved the patients’ walking resistance but also improved executive and memory functions (24, 40). This is in line with the results of the present study, with the DST-F and DST-B scores significantly different in the dual-task group compared with the conventional group after >4 weeks of intervention. The development of cognitive deficits post-stroke is associated with a reduction in the number of synapses and a decrease in the density of connections in hippocampal neurons (41). Dual-task executive function training increases not only hippocampal volume but also cortical area, especially in the prefrontal lobe, through high-intensity training (39).
Executive function is a control mechanism of the brain that includes processes such as planning, initiating, organising, inhibiting, problem solving, self-monitoring and error correction. Approximately 75% of stroke survivors experience executive dysfunction (4). Executive dysfunction reduces the ability to regain independence in activities of daily living. The TMT is a test of executive functioning and attention that focuses on rapid visual search, visuospatial ordering and cognitive orientation transfer. The Stroop Colour and Word Test (SCWT), a widely used measure of executive function, and its operation requires the synergistic action of multiple cognitive functions of the patient, including short-term memory, stereotype switching and attention (42, 43). The effectiveness of conventional cognitive rehabilitation methods in the treatment of patients with executive dysfunction is controversial. Chung et al. (4) found that cognitive rehabilitation intervention was not effective in patients with executive dysfunction. The results of the present study. Showed a difference in TMT-A results compared with the control group at >6 weeks of intervention. Danneels et al. (44) found that dual-task training had an effect on the executive function, memory and visuospatial ability of patients through a dual-task training study combining two forms of postural control with different cognitive tasks, both static and dynamic. This difference may be related to the timing of the intervention, and the specific execution of the cognitive–motor dual-task, including different cognitive activities, with the choice of motor activities also affecting the dual-task training effect due to the different effects of the dual-task interference they create (45, 46). In examining the immediate effects of dual-task obstacle crossing and single-task obstacle crossing training on the functional and cognitive abilities of chronic ambulatory participants with spinal cord injury, Amatachaya et al. (47) found that there was no significant difference in the percentage of errors in SCWT tasks in the dual-task group as compared with the conventional group, which is in line with the results of the present study. Due to the limitations of the number of participants and the duration of the intervention, the results need to be further validated in a large number of clinical trials.
Conclusion
In summary, cognitive–motor dual-task training is not only a promising adjunct but a clinically superior approach for remediating PSCI when compared with conventional single-task or usual care. The evidence indicates that commencing dual-task programmes within the subacute phase, and continuing them for at least 6 weeks, yields meaningful gains across global cognition, executive function and working memory. These benefits are robust, independent of stroke chronicity and attainable with readily available clinical resources. We therefore recommend that dual-task protocols be routinely integrated into standard stroke rehabilitation pathways and prioritised in future clinical guidelines.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Liu K Yin M Cai Z. Research and application advances in rehabilitation assessment of stroke. J Zhejiang Univ Sci B Biomed Biotechnol. (2022) 23:625–41. doi: 10.1631/jzus.B 2100999 PMC 938133035953757 · doi ↗ · pubmed ↗
- 2Mc Kevitt C Fudge N Redfern J Sheldenkar A Crichton S Rudd AR . Self-reported long-term needs after stroke. Stroke. (2011) 42:1398–403. doi: 10.1161/STROKEAHA.110.59883921441153 · doi ↗ · pubmed ↗
- 3Gibson E Koh CL Eames S Bennett S Scott AM Hoffmann TC . Occupational therapy for cognitive impairment in stroke patients. Cochrane Database Syst Rev. (2022) 3:CD 006430. doi: 10.1002/14651858.CD 006430.pub 335349186 PMC 8962963 · doi ↗ · pubmed ↗
- 4Chung CS Pollock A Campbell T . Cognitive rehabilitation for executive dysfunction in adults with stroke or other adult non-progressive acquired brain damage. Cochrane Database Syst Rev. (2013) 2013:CD 008391. doi: 10.1002/14651858.CD 008391.pub 223633354 PMC 6464714 · doi ↗ · pubmed ↗
- 5Kumar S Singh S Chadda RK Durward BR Hagen S. The effect of low-frequency repetitive transcranial magnetic stimulation at orbitofrontal cortex in the treatment of patients with medication-refractory obsessive-compulsive disorder: a retrospective open study. J ECT. (2018) 34:e 16–9. doi: 10.1097/YCT.000000000000046229053484 · doi ↗ · pubmed ↗
- 6He Y Yang L Zhou J Yao L Pang MYC. Dual-task training effects on motor and cognitive functional abilities in individuals with stroke: a systematic review. Clin Rehabil. (2018) 32:865–77. doi: 10.1177/026921551875848229473480 · doi ↗ · pubmed ↗
- 7Choi W Lee G Lee S. Effect of the cognitive-motor dual-task using auditory cue on balance of survivors with chronic stroke: a pilot study. Clin Rehabil. (2015) 29:763–70. doi: 10.1177/026921551455609325394396 · doi ↗ · pubmed ↗
- 8De Luca R Lo Buono V Leo A Russo M Aragona B Leonardi S . Use of virtual reality in improving poststroke neglect: promising neuropsychological and neurophysiological findings from a case study. Appl Neuropsychol Adult. (2019) 26:96–100. doi: 10.1080/23279095.2017.136304028937807 · doi ↗ · pubmed ↗