Evaluating the efficacy and tolerability of the oral combination of alpha lipoic acid and vitamin B complex preparation in carpal tunnel syndrome: a single center, randomized, double-blind, placebo-controlled trial
Nur Alya Zainal, Anna Misya’il Abdul Rashid, Adnan Lutfi A Rauf, Abdul Hanif Khan Yusof Khan, Wan Aliaa Wan Sulaiman, Hamidon Basri

TL;DR
A study tested a supplement containing alpha-lipoic acid and vitamin B complex for carpal tunnel syndrome and found it may help with pain but not other symptoms.
Contribution
This is the first randomized, double-blind, placebo-controlled trial evaluating the combination of alpha-lipoic acid and vitamin B complex for carpal tunnel syndrome.
Findings
The treatment group showed significant improvement in pain scores (VAS) compared to baseline.
The supplement was well tolerated with minimal and self-limiting side effects.
No significant differences were found in quality of life or nerve conduction study outcomes between groups.
Abstract
Carpal Tunnel Syndrome (CTS) is the most common type of nerve entrapment and can cause significant disability by impairing hand functionality. This study aims to evaluate the efficacy and tolerability of an oral combination of alpha-lipoic acid (ALA) and vitamin B complex in alleviating CTS symptoms and improving the quality of life in patients with mild to moderate CTS. A total of 70 patients with mild to moderate CTS were enrolled in this study at Hospital Sultan Abdul Aziz Shah, Selangor, Malaysia. Using a double-blind Randomized Controlled Trial (RCT) design, participants were randomly assigned to either the treatment group (n = 37) or the placebo group (n = 33). The treatment group received two tablets once daily containing alpha-lipoic acid (300 mg), methylcobalamin (500 mcg), vitamin B1 (39 mg), and vitamin B6 (8 mg) i.e. Bionerv while placebo group received combination of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
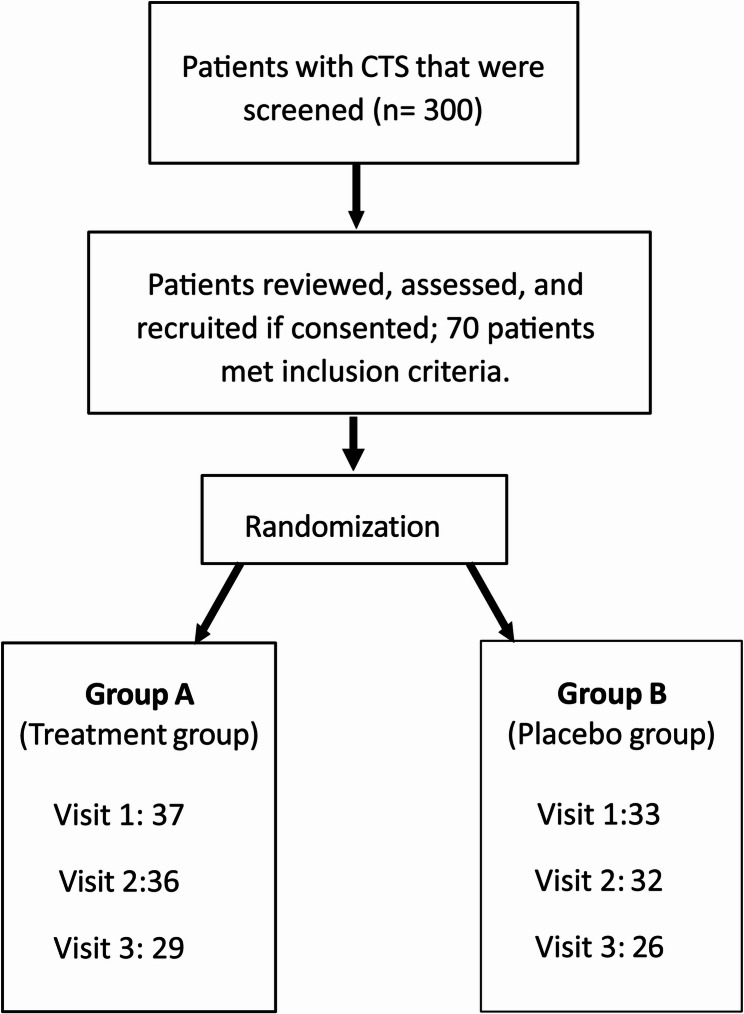 Figure 1
Figure 1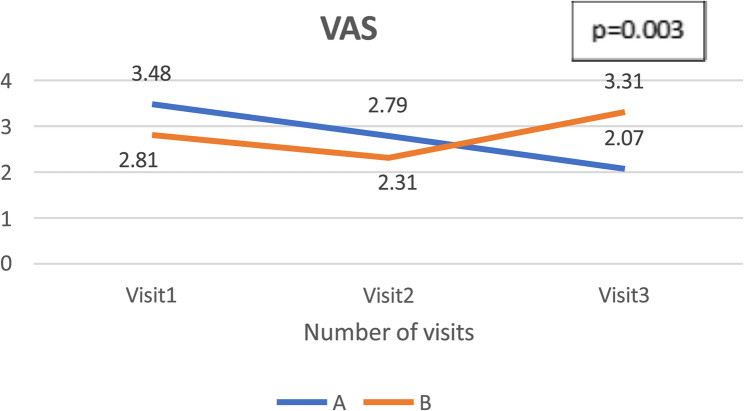 Figure 2
Figure 2- —Brego Life Sciences
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBiochemical Acid Research Studies · Peripheral Nerve Disorders · Pregnancy-related medical research
Background
Carpal tunnel syndrome (CTS) is the most common form of nerve entrapment neuropathy in the hand, and it has a high global prevalence, including in Malaysia, where an estimated 20–60% of the population is diagnosed with CTS [1, 2]. CTS significantly impairs hand functionality, leading to substantial disability. A study in the United States reported CTS-related disability incidence rates per 100 person-years as 33.2 for work pace or quality changes, 16.3 for lost time, and 20.0 for job changes, emphasizing its impact on occupational productivity [3]. Lost time, defined as workdays missed due to CTS, averaged 28 days in 2015—comparable to fractures and exceeding amputations [4, 5]. The substantial economic and functional burden of CTS underscores the necessity for effective therapeutic strategies to mitigate its impact.
Current treatment options for CTS include surgical decompression for severe cases and multimodal therapy for mild to moderate cases, consisting of conservative treatments such as oral medications (vitamin B complex, analgesia), splinting, physiotherapy, and injections (steroids or platelet-rich plasma) [6]. However, local steroid and anaesthetic injections are costly and invasive, thus not preferred by patients, while long-term analgesia use poses sedative risks [7]. Alpha-lipoic acid (ALA), known for its benefits in diabetic neuropathy, is hypothesized to aid in CTS by promoting nerve regeneration and reducing pain, though its impact on functional outcomes remains limited [8]. Previous studies on alpha-lipoic acid (ALA) have reported mild side effects such as nausea, abdominal discomfort, dizziness, and skin reactions thus it is important also to reassess the tolerability of the ALA and vitamin B complex combination in the local population [9].
Alpha-lipoic acid has shown promise in peripheral nerve disorders and is increasingly explored for carpal tunnel syndrome (CTS) due to its potent antioxidant properties. CTS pathophysiology involves ischemia-reperfusion injury, which elevates oxidative stress and impairs nerve regeneration [10]. ALA mitigates oxidative damage by neutralizing free radicals, restoring antioxidant activity (e.g., vitamins E and C), and boosting glutathione levels essential for tissue repair [11]. Clinical studies and meta-analyses have demonstrated ALA’s efficacy in reducing pain and improving symptoms, particularly in postoperative CTS management ([9, 12]– [13]). However, local data remain limited, highlighting the need for further research in the Malaysian population.
Methodology
Study design and participants
This was a double-blind, placebo-controlled randomized controlled trial, from December 2023 to September 2024 in a tertiary center in Malaysia. Relevant national regulatory authorities and ethics committees approved the study protocol (JKEUPM-2022-98) and the protocol was registered with Clinical Trial Gov (NCT06940557) retrospectively. We recruited patients aged 18 years and above who were diagnosed with CTS. The inclusion criteria included anyone with numbness and tingling sensation at the first finger until the radial site of the 4th finger and/or fulfil the electrodiagnostic criteria of mild to moderate CTS, based on the Padua Scale as defined below [14]:
• Mild: abnormal digit/wrist Sensory Nerve Conduction Velocity (CV) and normal Distal Motor Latency (DML).
- Moderate: abnormal digit/wrist Sensory Nerve Conduction Velocity (SNCV) and abnormal Distal Motor Latency (DML).
We excluded patients who were pregnant or breastfeeding, with symptoms of CTS but have normal NCS, taking traditional or complementary medication for CTS or patients with electrodiagnostic criteria of severe or extreme CTS as defined in the Padua scale:
• Severe: Absence of sensory response (SNAP) and abnormal Distal Motor Latency (DML).
- Extreme: Absence of motor (CMAP) and sensory responses (SNAP).
Study treatment and procedures
The patients were randomized to receive oral combination of alpha lipoic acid and vitamin B; Bionerv (alpha lipoic acid; 300 mg, methylcobalamin; 500mcg, vitamin B1; 39 mg and vitamin B6; 8 mg), 2 tablets once daily or placebo drug (maltodextrin, microcrystalline cellulose, tricalcium phosphate, silicon gioxide, magnesium stearate), 2 tablets once daily for 6 months. Randomization sequence was done by using an online random number generator program using a mixed block randomization technique at a ratio of 1:1. In cases of serious adverse event, unblinding process was incorporated where the identity of the drug was revealed to manage the subject’s condition. This was done by intruding the emergency code key by the researcher. All patients provided a written consent for the study.
During Visit 1, a thorough history and physical examination were performed, and demographic data were collected. Patients then completed three validated, self-administered questionnaires: the Boston Carpal Tunnel Questionnaire (BCTQ), Visual Analogue Scale (VAS), and SF-36. The BCTQ is a disease-specific tool for assessing CTS severity, comprising two subscales: the Symptom Severity Scale (SSS) with 11 items and the Functional Status Scale (FSS) with 8 items. Each item is rated on a 5-point Likert scale (1 = no symptoms/difficulty, 5 = most severe symptoms/greatest difficulty). The total score for each subscale is calculated as the mean of its item scores, resulting in a final SSS and FSS score ranging from 1.0 to 5.0. Higher scores reflect worse symptoms or greater functional impairment. The BCTQ is widely used due to its strong cross-cultural adaptability and proven validity and reliability across multiple languages ([15]– [16]).
The VAS is a visual scale with 0 scored as “no pain” and 10 as “worst pain imaginable” and serves as an excellent tool for pain score with excellent validity and reproducibility ([17]– [18]). The SF-36 is a quality-of-life questionnaire that comprises of 36 questions covering eight domains of health which are; Physical Functioning (PF), Role Limitations due to Physical Health, Role Limitations (RL) due to Emotional Problems (RE), energy/fatigue, emotional well-being, social functioning, pain, and general health (GH) where a higher score indicates a better outcome [19]. After the administration of these questionnaires, they will be subjected for a nerve conduction study (NCS) to determine the severity of CTS. The NCS were performed by the same trained personnel to ensure consistency and accuracy.
The patients were reassessed at Visit 2 (3 months post-treatment) and Visit 3 (6 months post-treatment). During each visit, they underwent physical examination, NCS, and were required to complete the three sets of questionnaires (BCTQ, VAS, and SF-36). They were also required to fill in the form regarding the side effects of the treatments at Visit 2 and Visit 3. The investigators made a phone call and sent reminder message at the 6th and 18th week to ensure compliance, medication adequacy and follow up review. During the study, all participants received standard care, including nighttime wrist splinting and physiotherapy when indicated. Physiotherapy included tendon and nerve gliding exercises and ultrasound therapy, applied equally to both groups to ensure consistent care aside from the intervention.
Outcomes
The primary outcome was the electrodiagnostic improvement of the median nerve on NCS, assessed between baseline (Visit 1, prior to intervention), and compared to follow-up evaluations at three months (Visit 2) and six months (Visit 3) after the intervention. The NCS parameters that are analysed were: DSL (normal value for DSL < 3.5ms), SNAP (normal value for SNAP > 2.5 µV), CV (normal value for CV > 50 m/s), DML (normal value for DML < 4ms), CMAP (normal value for CMAP > 4.0 mV) [20]. The secondary outcomes measure were the changes in BCTQ, VAS and SF-36 scores between the intervention (visit 1) and at three-months (visit 2) and six- months (visit 3) of treatment as well as side effects of the treatment.
Statistical analysis
The data analysis was performed using the IBM SPSS Statistics for Windows, Version 27.0 (IBM Corp., Armonk, NY, USA). The descriptive statistics were expressed as numbers and percentages for categorical variables and as mean for numerical variables. Repeated measure ANOVA statistical analysis was used to assess the effect of intervention on the primary and secondary outcomes. The confidence level was set at 0.05 (α = 0.05) and significant finding was if the p-value is less than 0.05 (p < 0.05). Data normality was assessed using the skewness test, with normal distribution defined within the range of + 2 to −2. Mauchly’s sphericity test was conducted, with most results achieving p > 0.05, indicating that the assumption of sphericity was met. For data that violated sphericity, the Greenhouse-Geisser correction was applied.
Results
Baseline demographic
A total of 70 patients were recruited during the first visit. Of these, 37 patients were assigned to Group A (treatment group) and 33 to Group B (placebo group). During visit 2, a total of 68 patients came for evaluation: 36 patients from Group A and 32 from Group B. Two patients were absent due to logistic issues. Despite multiple reminder calls and messages, only 55 patients attended visit 3, 29 patients from Group A and 26 patients from Group B. The study flow chart is shown in Fig. 1.Fig. 1. Study flowchart
The baseline demographics and characteristics of patients showed that both groups were well-matched in age, gender, weight, hand involvement, race, and comorbidities (Table 1). The mean age was 50 years. Females were predominant in both groups, 78.4% (Group A) and 66.7% (Group B). Malays were the largest ethnic group in both groups, followed by Indians and Chinese. Most patients were overweight or obese, with mean weight of 74.1 kg (Group A) and 72.8 kg (Group B). Hypertension, diabetes and dyslipidemia were common comorbidities in both groups. Symptoms were mostly bilateral in both groups with moderate CTS being the most prevalent severity. Physiotherapy attendance was generally low (35.1% in Group A, 30.3% in Group B). Treatment compliance was higher in Group A (73%) compared to Group B (60.6%).Table 1. Baseline demographicFactorsGroupsP-valueABSample size (n)3733Age (mean, years)50.950.80.954GenderFrequency, n (%)Frequency, n (%)Male8 (21.6)11 (33.3)0.278Female29 (78.4)22 (66.7)Weight (mean, kg)74.172.80.76BMI range (kg/m^2^)Frequency, n (%)Frequency, n (%)18.5–22.93 (8.1)5 (15.2)23.0-26.912 (32.4)11 (33.3)0.715> 2722 (59.5)17 (51.5)RaceFrequency, n (%)Frequency, n (%)Malay33 (89.2)28 (84.8)Indian3 (8.1)5 (15.2)0.863Chinese1 (2.7)0Co-morbiditiesFrequency, n (%)Frequency, n (%)Hypertension9 (24.3)12 (36.4)0.279Diabetes10 (27)13 (39.4)0.278Dyslipidaemia15 (40.5)14 (42.4)0.875Rheumatoid arthritis02 (6.1)0.132Thyroid disorders2 (5.4)4 (12.1)0.323Hand involvementFrequency, n (%)Frequency, n (%)Right3 (8.1)6 (18.2)Left5 (13.5)3 (9.1)0.356Bilateral29 (78.4)24 (72.7)SeverityFrequency, n (%)Frequency, n (%)Mild11 (30)12 (36)0.583Moderate26 (70)21 (64)PhysiotherapyFrequency, n (%)Frequency, n (%)Yes13 (35.1)10 (30.3)0.673No24 (64.9)23 (69.7)ComplianceFrequency, n (%)Frequency, n (%)Yes27 (73)20 (60.6)0.278No10 (27)13 (39.4)
Primary outcomes
The primary outcomes for this study are the changes in the NCS findings after the intervention given. There were no significant different in DSL, SNAP, Velocity, DML and CMAP of both hands between the placebo and the treatment group (Table 2). Nevertheless, there were a relatively better improvement of CMAP in left hand among Group A where the subjects were able to achieve an increment of 0.666 mV. The mean was 8.31 mV at Visit 1 and it improve to 8.98 mV in Visit 2. In comparison, Group B only achieved a 0.025 mV of increment.Table 2. Summary of the NCS findings among group A and group BDependent variablesGroupMean ± SDMean differences (V3- V1)P- value (P < 0.05)Partial ETA squared (n^2^)1. Distal Sensory Latency (DSL), right hand (ms)AVisit 01: 4.04 ± 0.440.0060.4710.011Visit 02: 4.11 ± 0.12Visit 03: 4.05 ± 0.65BVisit 01: 4.56 ± 0.65−0.2768Visit 02: 4.42 ± 0.21Visit 03: 4.28 ± 0.972. Distal Sensory Latency (DSL), left hand (ms)AVisit 01: 4.37 ± 0.960.0380.9110.002Visit 02: 4.29 ± 0.97Visit 03: 4.41 ± 0.23BVisit 01: 3.99 ± 0.250.145Visit 02: 4.01 ± 0.55Visit 03: 4.15 ± 0.803. Sensory Nerve Action Potential (SNAP), right hand (µV)AVisit 01: 23.49 ± 0.765.6460.3530.019Visit 02: 28.11 ± 0.85Visit 03: 29.14 ± 0.36BVisit 01: 23.91 ± 0.161.664Visit 02: 25.56 ± 0.13Visit 03: 25.58 ± 0.954. Sensory Nerve Action Potential (SNAP), left hand (µV)AVisit 01: 28.90 ± 0.640.450.5830.011Visit 02: 29.29 ± 0.29Visit 03: 29.35 ± 0.43BVisit 01: 30.18 ± 0.95−0.449Visit 02: 33.19 ± 0.92Visit 03: 29.73 ± 0.915. Velocity of Right Hand (m/s)AVisit 01: 40.55 ± 0.243.17240.7030.006Visit 02: 41.22 ± 0.26Visit 03: 43.72 ± 0.51BVisit 01: 38.68 ± 0.971.16Visit 02: 39.04 ± 0.33Visit 03: 39.84 ± 0.646. Velocity of Left Hand (m/s)AVisit 01: 39.07 ± 0.241.2140.7830.004Visit 02: 39.30 ± 0.27Visit 03: 40.82 ± 0.81BVisit 01: 41.54 ± 0.832.417Visit 02: 41.29 ± 0.70Visit 03: 43.96 ± 0.937. Distal Motor Latency, right hand (ms)AVisit 01: 4.39 ± 0.15−0.3850.2680.024Visit 02: 4.08 ± 0.37Visit 03: 4.01 ± 0.28BVisit 01: 4.72 ± 0.37−0.197Visit 02: 4.73 ± 0.38Visit 03: 4.52 ± 0.188. Distal Motor Latency (DML), left hand (ms)AVisit 01: 4.44 ± 0.88−0.1650.4970.013Visit 02: 4.38 ± 0.57Visit 03: 4.27 ± 0.56BVisit 01: 4.36 ± 0.19−0.187Visit 02: 4.55 ± 0.57Visit 03: 4.17 ± 0.289. Compound Muscle Action Potential (CMAP), Right hand(mV)AVisit 01: 8.18 ± 0.640.8390.8880.002Visit 02: 8.79 ± 0.49Visit 03: 9.01 ± 0.63BVisit 01: 8.57 ± 0.720.842Visit 02: 8.94 ± 0.59Visit 03: 9.41 ± 0.1410. Compound Muscle Action Potential (CMAP), Left hand(mV)AVisit 01: 8.31 ± 0.740.6660.4380.015Visit 02: 8.60 ± 0.36Visit 03: 8.98 ± 0.14BVisit 01: 8.57 ± 0.500.025Visit 02: 9.05 ± 0.27Visit 03: 8.82 ± 0.39
Another component that showed a relatively a better outcome in NCS is SNAP in both hands. The mean SNAP of right hand in Group A at baseline was 23.50 µV and it increased to 29.14 µV in visit 3, a 5.65 µV difference. While in group B, the mean SNAP of the right only achieved a 1.66 µV of increment. The mean increased from 23.49 µV in Visit 1 to 25.58 µV in Visit 2. Similarly, the mean SNAP of the left hand in group A showed a slight improvement in Visit 2. The mean increased from 28.90 µV at baseline to 29.35 µV in Visit 2. On the other hand, group B show a slight decrement compared to its baseline in Visit 2. The mean decreased from 30.18 µV to 29.73 µV.
Overall, Group A demonstrated a significantly greater reduction in severity at Visit 2 compared to Group B. Specifically, Group A showed a 15% reduction in moderate severity at Visit 2 relative to Visit 1, whereas Group B only achieved a 6% reduction from baseline. Additionally, Group A recorded a higher increase in the proportion of patients with mild CTS, with a 15% increase from baseline, compared to a 6% increase in Group B (Table 3). This suggests that more patients in Group A experienced improved median nerve conduction, as a greater number transitioned from moderate to mild CTS compared to Group B.Table 3. The summary of severity changes of CTS in group A and group BGroupABP-valueSeverityMildModerateMildModerateVisit 1 (n,%)11 (30%)26 (70%)12 (36%)21 (64%)0.738Visit 2 (n,%)14 (39%)22 (61%)9 (28%)23 (72%)0.497Visit 3 (n,%)13 (45%)16 (55%)11 (42%)15 (58%)1.000
Secondary outcomes
SF-36 questionnaire score
The SF-36 questionnaire is used to assess the quality of life, consisting of 8 components (Physical Functioning (PF), Role Limitations due to Physical Health, Role Limitations (RL) due to Emotional Problems (RE), energy/fatigue, emotional well-being, social functioning, pain, and general health (GH), where a higher score indicates a better outcome. In this study, there were no significant differences in all these 8 components between the two groups. However, there is a trend showing that Group A (i.e. treatment group) subjects show better improvement in five out of the eight domains: namely PF, RL, RE, emotional and pain (Table 4).Table 4SF-36 results in visit 1, 2 and 3 for both group A and BDependent variablesGroupMean ± SDMean differences (V3-V1)P-value(p < 0.05) Partial ETA squared (n2)1. Physical functioning (PF)AVisit 01: 61.55 ± 4.627.240.3710.018Visit 02: 65.86 ± 5.30Visit 03: 68.79 ± 4.41BVisit 01: 67.11 ± 4.870.469Visit 02: 70.96 ± 5.32Visit 03: 67.58 ± 4.412. Role of Physical Limitation (RL)AVisit 01: 37.93 ± 6.3523.2760.090.044Visit 02: 61.21 ± 5.62Visit 03: 61.21 ± 5.07BVisit 01: 56.73 ± 5.862.885Visit 02: 56.73 ± 4.01Visit 03: 59.62 ± 3.793. Role of Emotional Limitation (RE)AVisit 01: 60.92 ± 5.7019.540.2730.024Visit 02: 68.97 ± 3.56Visit 03: 80.46 ± 4.80BVisit 01: 77.06 ± 4.101.141Visit 02: 75.64 ± 3.70Visit 03: 78.20 ± 5.554. EnergyAVisit 01: 67.24 ± 5.306.7240.8120.004Visit 02: 69.31 ± 6.41Visit 03: 73.97 ± 4.37BVisit 01: 65.58 ± 5.27.692Visit 02: 70.77 ± 6.35Visit 03: 73.27 ± 4.825. EmotionalAVisit 01: 77.59 ± 7.747.7520.4170.016Visit 02: 80.04 ± 8.58Visit 03: 84.58 ± 8.01BVisit 01: 77.23 ± 7.723.077Visit 02: 75.69 ± 7.12Visit 03: 80.31 ± 8.236. SocialAVisit 01: 77.59 ± 4.875.6040.6250.09Visit 02: 77.59 ± 7.76Visit 03: 83.19 ± 6.66BVisit 01: 72.60 ± 5.9910.577Visit 02: 77.40 ± 3.78Visit 03: 83.17 ± 3.787. PainAVisit 01: 53.62 ± 7.1912.5860.2520.026Visit 02: 62.41 ± 9.46Visit 03: 66.21 ± 9.82B Visit 01: 63.94 ± 6.922.404Visit 02: 67.12 ± 8.96Visit 03: 66.35 ± 7.648. General health (GH)AVisit 01: 61.72 ± 3.296.2070.1380.138Visit 02: 61.21 ± 7.33Visit 03: 67.91 ± 6.01BVisit 01: 54.23 ± 6.438.846Visit 02: 62.50 ± 3.10Visit 03: 63.07 ± 7.85
In the PF domain for instance, Group A achieved a 7.24 increment as compared to Group B which shows deterioration among the three visits, although it was not statistically significant. Similarly in the RL domain, Group A showed an increment of 23.27 while group B showed only 2.88, however it did not reach statistical significance. In the RE and emotional domain, again there was a trend showing increment in Group A versus Group B (19.54 vs. 1.14 and 7.75 vs. 3.07) but this increment was not statistically significant. Another component that showed improvement among the Group A is the pain component where there is a marked increment of 12.58 points from its baseline as compared to Group B which showed a modest increment of 2.40 from its baseline, however it was not statistically significant.
BCTQ questionnaire score
Overall, Group A has slightly better improvement as compared to Group B in both components of the BCTQ questionnaire, however they did not reach statistical significance. The mean SSS in Group A decrease by 0.68 points, while Group B showed a smaller reduction by 0.49 points. In terms of FSS component, the mean of FSS in group A had a decrement of 0.45 points from its baseline, while Group B only achieved a reduction of 0.19 points (Table 5).Table 5BCTQ and VAS score in in visit 1, 2 and 3 for group A and BDependent variablesGroupMean ± SDMean differences (V3-V1)P-value(p < 0.05)Partial ETA squared (n^2^)BCTQ1. Functional Status Scale(FSS)AVisit 01: 2.30 ± 0.24−0.4560.470.013Visit 02: 1.91 ± 0.39Visit 03: 1.82 ± 0.33BVisit 01: 1.80 ± 0.30−0.197Visit 02: 1.72 ± 0.19Visit 03: 1.60 ± 0.192. Symptom Specific Scale(SSS)AVisit 01: 2.60 ± 0.16−0.680.4510.015Visit 02: 2.05 ± 0.37Visit 03: 1.92 ± 0.30BVisit 01: 2.43 ± 0.33−0.49Visit 02: 1.94 + 0.16Visit 03: 1.94 ± 0.39Visual Analogue Scale(VAS)AVisit 01: 3.48 ± 0.36−1.4140.0030.103Visit 02: 2.79 ± 0.20Visit 03: 2.07 ± 0.20BVisit 01: 2.81 ± 0.200.5Visit 02: 2.31 ± 0.23Visit 03: 3.31 ± 0.28
VAS score
The mean VAS score in Group A decreased from 3.48 at baseline to 2.06, while in Group B, it increased from 2.80 to 3.30 (Table 5; Fig. 2). This change was statistically significant with a moderate effect size (p = 0.003, η² = 0.103).Fig. 2 Mean of VAS in Visit 1, 2 and 3 for Group** A** and B
Tolerability
A higher proportion of participants in Group B reported no side effects compared to Group A (82% vs. 68%) (Table 6). Tolerability in this study was assessed based on patient-reported side effects; however, a definitive causal relationship with the investigational treatment could not be established. Further analyses, such as blood investigations, would be required to determine any potential association.Table 6. Tolerability of treatment drugsSide effectsGroup A (n = 37)n (%)Group Bn (%)P-valueDiarrhoea5 (13.5)3 (9.1)0.866Abdominal pain2 (5.4)00.180Urticaria1 (2.7)00.393Weight gain1 (2.7)3 (9.1)0.908Smelly urine2 (5.4)00.180Bloated1 (2.7)00.936No side effects25 (67.6)27 (81.8)0.994
Discussion
The study findings indicate that patients receiving the oral combination of alpha-lipoic acid and vitamin B complex (Bionerv) experienced better pain control compared to the placebo group, as demonstrated by improvements in VAS scores. Although there was no statistically significant improvement in the pain component of the SF-36 or the BCTQ, the modest decrease in VAS scores from 3 to 2 may still be clinically relevant in the context of mild CTS. The baseline pain scores were relatively low likely due to the study’s focus on patients with mild to moderate CTS. While patients in the placebo group initially showed pain reduction in the first three months, this improvement was not sustained, with scores returning to 3 at six months, likely due to a placebo effect. These findings suggest that the combination may offer short-term pain relief, but the evidence for consistent and sustained analgesia is limited and requires further study.
The proposed benefits in quality of life (QoL) were not supported by statistically significant improvements in SF-36 or BCTQ scores. Therefore, any observed changes in these domains should be interpreted with caution. However, the improvement in VAS score is due to the analgesic effects of alpha-lipoic acid, that are likely mediated through multiple mechanisms, including attenuation of median nerve inflammation, reduction of oxidative stress and promotion of nerve regeneration [11]. Furthermore, its ability to inhibit neuronal T-type calcium channels may contribute to decreased neuronal excitability and pain perception [20]. As these mechanisms primarily influence pain modulation, the explanation above has been repositioned to align with pain-related outcomes rather than QoL improvements.
In addition to pain reduction, the oral combination of alpha-lipoic acid and vitamin B complex may contribute to improved quality of life and functional outcomes. Although the observed changes in SF-36 and BCTQ scores were not statistically significant, a trend toward improvement was noted in the treatment group at six months. This may be attributed to the analgesic effects of alpha-lipoic acid, which reduce pain intensity and enable greater engagement in daily activities, ultimately enhancing physical and emotional well-being. Beyond pain relief, alpha-lipoic acid may enhance nerve repair and reduce oxidative stress, potentially improving function and perceived quality of life despite the lack of statistical significance.
The findings of this study are consistent with Passiatore et al., which showed that Alpha Lipoic Acid-R (ALA-R) 600 mg significantly reduced daytime and nighttime pain in mild to moderate CTS patients within two months [9]. Similarly, Notarnicola et al., found that oral ALA supplementation effectively reduced pain over six months, with no added benefit from Extracorporeal Shockwave Therapy (ESWT) [21]. These findings further support the potential role of ALA in CTS management.
Although there was no statistical significance observed in the SSS and FSS components of the BCTQ, there was a larger mean reduction in in both of components in the treatment group, suggesting a possible trend towards symptom control and functional improvement. Our results resonated with several other studies that reported no significant BCTQ differences between treatment and placebo groups [9, 22]. The lack of significant changes in BCTQ scores among ALA-treated CTS patients may stem from mild disease severity where baseline functional impairment may not have been severe enough to detect substantial improvements in BCTQ scores.
- Hence, the use of NCS was necessary to look at objective improvement in CTS severity.
Despite no significant differences in DSL, SNAP, velocity, DML, or CMAP between the placebo and treatment groups, both groups showed mild improvements in electrophysiological parameters over time. Improvements were observed in mean CMAP over the left hand and SNAP in both hands within the treatment group at six months of treatment. However, since similar improvements were seen in the placebo group, the findings may reflect the natural course of recovery or placebo effect rather than a specific treatment effect. Overall, the NCS findings indicate a shift from moderate to mild CTS over time in both groups, where the proportion of mild cases continued to rise, with slightly greater reductions in moderate CTS in the treatment group. These findings suggest that while ALA may support nerve recovery, further studies are needed to confirm its specific contribution.
The tolerability in this study is based on patient reporting side-effects that developed after taking the medications. There are no blood or radiological investigation involved to confirm its association with the symptoms. In this study, most patients who received treatment and placebo group did not develop any side effects. The most common side- effects of the treatment that are observed in this study is diarrhoea, followed with abdominal pain and changed in urine odour. These symptoms are reported to be temporary, and it subsided after two weeks of discontinuation of the medications. Therefore, in this study, the treatment group are found to be tolerable, in agreement with most international studies ([23, 24]).
Conclusion
Overall, the oral combination of alpha-lipoic acid and vitamin B complex (Bionerv) demonstrated modest but consistent pain relief over six months, with trends suggesting potential functional and quality of life benefits. While the findings were not statistically significant, they align with previous studies supporting the role of ALA in CTS management. These effects may become more evident with a longer treatment duration. Given its tolerability and observed clinical improvements, this combination may serve as a supportive therapy in patients with mild to moderate CTS while awaiting definitive interventions. The limited sample size and study duration may have constrained the ability to detect stronger effects, highlighting the need for larger, longer-term trials.
The strength of this study lies in its RCT design, with computer-generated randomization, minimizing allocation bias. The double-blind approach ensures unbiased assessment. Additionally, the comparable baseline demographics between groups enhance comparability. The study also integrates objective NCS assessments alongside questionnaires, providing valuable insights into the effects of alpha-lipoic acid and vitamin B complex on median nerve electrophysiology.
This study had several limitations, including a small sample size, single-center design with limited ethnic diversity, and non-compliance influenced by pill burden, fasting, and festive seasons. Confounding factors, such as higher physiotherapy attendance in treatment group and unassessed diabetes control, may have affected outcomes. Despite these, findings suggest that alpha-lipoic acid (600 mg) with vitamin B complex (Bionerv) is a promising adjunct therapy for mild to moderate CTS, with prolonged use potentially enhancing nerve regeneration and quality of life.
Future research should involve a larger, multi-center sample for better statistical reliability and patient representation. A dedicated team should improve compliance through reminders, pill-counting methods, and small incentives to reduce dropout rates. Long-term studies should monitor ALA tolerability and safety, assessing liver, kidney, and potential systemic complications.
Supplementary Information
Supplementary Material 1.
Supplementary Material 2.
Supplementary Material 3.
Supplementary Material 4.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sevy JO, Sina RE, Varacallo M. Carpal Tunnel Syndrome. In: *Stat Pearls [Internet].* Treasure Island (FL): Stat Pearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK 448179/. Accessed 29 Oct 2023.28846321 · pubmed ↗