Procalcitonin as a Potential Prognostic Marker in Advanced Hodgkin Lymphoma: A Case-Based Perspective
Mohamad Mosi, Refat Jayyusi, Shaila Saaki, Moin Makrani, Mazin Saadaldin

TL;DR
This case report explores procalcitonin (PCT) as a possible indicator of disease severity in advanced Hodgkin lymphoma, highlighting its potential role beyond infection detection.
Contribution
The paper presents a case where elevated PCT levels in Hodgkin lymphoma may reflect tumor-driven inflammation rather than infection, suggesting a novel prognostic application.
Findings
PCT levels rose in a patient with advanced Hodgkin lymphoma despite no evidence of infection.
The case suggests PCT elevation may be linked to HL-associated systemic inflammation.
The report advocates for cautious interpretation of PCT in oncology and further study of its prognostic value.
Abstract
This case report examines the potential role of procalcitonin (PCT) as a prognostic biomarker in classic Hodgkin lymphoma (cHL), focusing on a 61-year-old male with advanced disease and systemic inflammation. The patient presented with progressive dyspnea, bilateral pleural effusions, and mediastinal lymphadenopathy. Imaging revealed hepatic, splenic, and adrenal involvement, consistent with stage IV HL. Axillary lymph node biopsy confirmed lymphocyte-rich cHL, with immunohistochemical markers including CD30, CD15, PAX5, Ki-67, MUM1, and BCL6. Despite broad-spectrum antimicrobial therapy and a comprehensive infectious workup, the patient exhibited rising PCT levels (peak 4.5 ng/mL) and declining albumin levels, with no microbiological evidence of infection. This persistent elevation of PCT in the absence of confirmed infection suggests a possible link between HL-associated inflammation…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
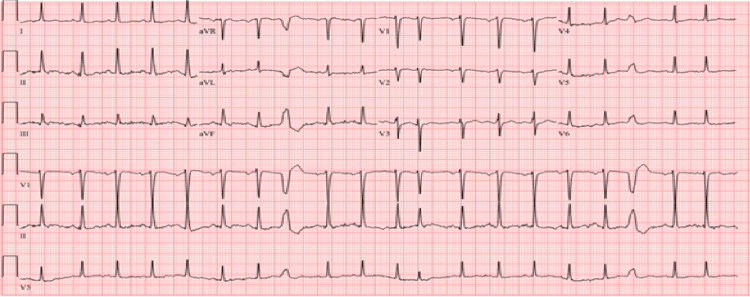 Figure 1
Figure 1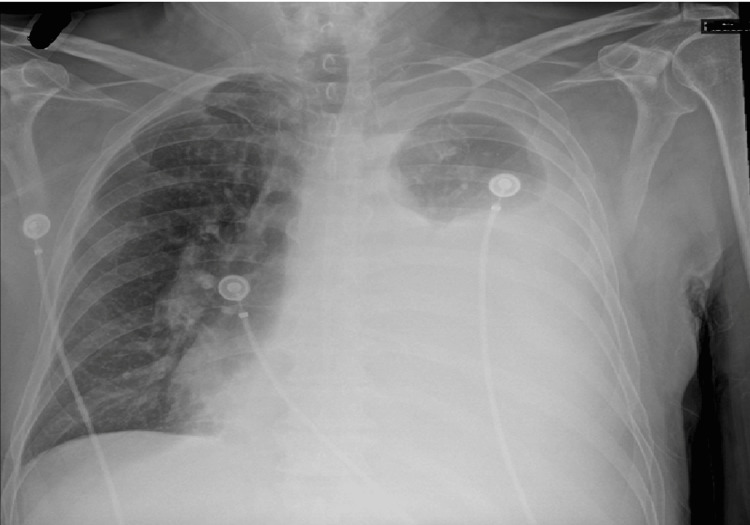 Figure 2
Figure 2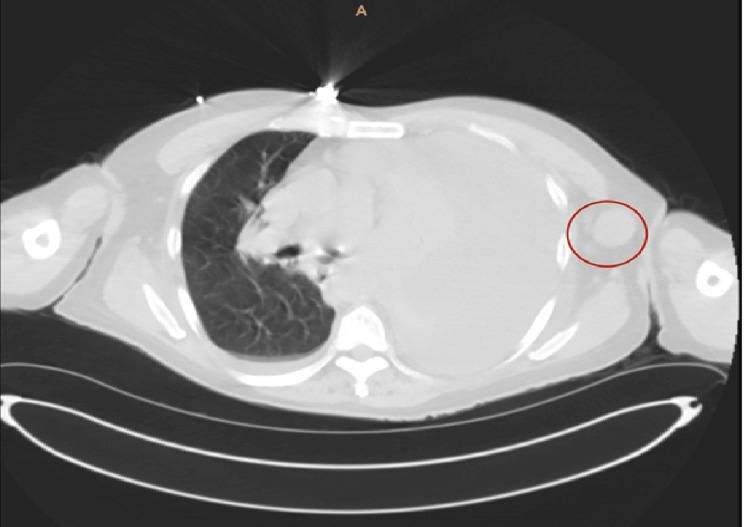 Figure 3
Figure 3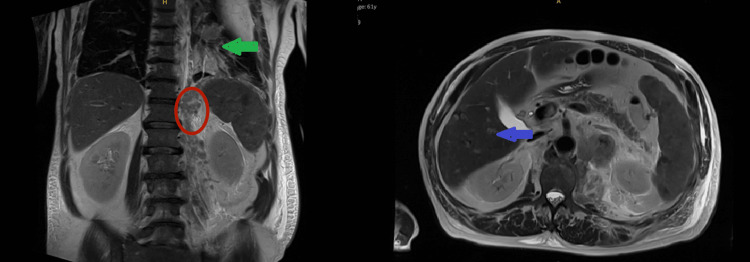 Figure 4
Figure 4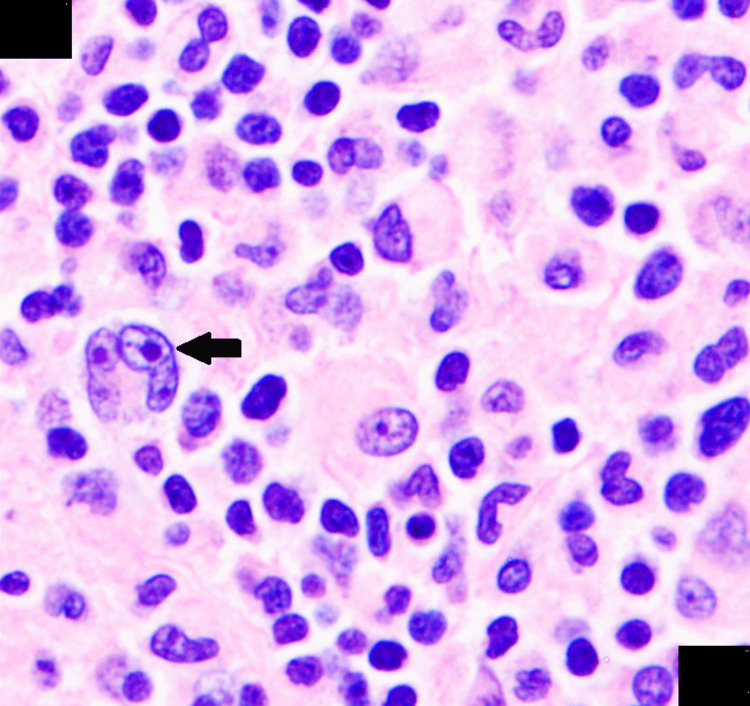 Figure 5
Figure 5| Parameter | Patient value | Reference range |
| WBC | 10.2 ×10⁹/L | 4.0-11.0 ×10⁹/L |
| Hg | 11 g/dL | 13.5-17.5 g/dL (male) |
| Hct | 37% | 41-53% (male) |
| PLT | 258 ×10⁹/L | 150-400 ×10⁹/L |
| TP | 6.3 g/dL | 6.0-8.3 g/dL |
| LDH | 240 U/L | 140-280 U/L |
| ALP | 200 U/L | 44-147 U/L |
| ALT | 10 U/L | 7-56 U/L |
| AST | 9 U/L | 10-40 U/L |
| TB | 0.5 mg/dL | 0.1-1.2 mg/dL |
| BUN | 20 mg/dL | 7-20 mg/dL |
| Cr | 1.2 mg/dL | 0.7-1.3 mg/dL (male) |
| Na | 136 mmol/L | 135-145 mmol/L |
| K | 4.5 mmol/L | 3.5-5.0 mmol/L |
| Ca | 8.5 mg/dL | 8.6-10.2 mg/dL |
| Mg | 1.5 mg/dL | 1.7-2.2 mg/dL |
| Albumin | 3 g/dL | 3.5-5.0 g/dL |
| Cholesterol | 250 mg/dL | <200 mg/dL |
| HDL | 35 mg/dL | >40 mg/dL (male) |
| TG | 170 mg/dL | <150 mg/dL |
| Glucose (blood) | 110 mg/dL | 70-99 mg/dL (fasting) |
| CRP | >190 mg/L | <10 mg/L |
| PCT | 0.3 ng/mL | <0.05 ng/mL |
| Lactic acid | 0.1 mmol/L | 0.5-2.2 mmol/L |
| ABG pH | 7.47 | 7.35-7.45 |
| ABG PCO₂ | 35 mmHg | 35-45 mmHg |
| ABG PO₂ | 45 mmHg | 75-100 mmHg |
| ABG HCO₃ | 20 mmol/L | 22-26 mmol/L |
| Pleural fluid WBC | 500 /µL | <500 /µL (non-infectious) |
| Pleural fluid LDH | 190 U/L | <200 U/L (transudate) |
| Pleural fluid TP | 4 g/dL | <3 g/dL (transudate) |
| Pleural fluid glucose | 50 mg/dL | >60 mg/dL |
| Parameter | Patient value | Reference range |
| WBC | 11 ×10⁹/L | 4.0-11.0 ×10⁹/L |
| Hg | 10.5 g/dL | 13.5-17.5 g/dL (male) |
| Hct | 36% | 41-53% (male) |
| PLT | 233 ×10⁹/L | 150-400 ×10⁹/L |
| TP | 7 g/dL | 6.0-8.3 g/dL |
| LDH | 270 U/L | 140-280 U/L |
| ALP | 210 U/L | 44-147 U/L |
| ALT | 25 U/L | 7-56 U/L |
| AST | 35 U/L | 10-40 U/L |
| TB | 1 mg/dL | 0.1-1.2 mg/dL |
| BUN | 29 mg/dL | 7-20 mg/dL |
| Cr | 1.4 mg/dL | 0.7-1.3 mg/dL (male) |
| Na | 140 mmol/L | 135-145 mmol/L |
| K | 4 mmol/L | 3.5-5.0 mmol/L |
| Ca | 8 mg/dL | 8.6-10.2 mg/dL |
| Mg | 1.2 mg/dL | 1.7-2.2 mg/dL |
| Albumin | 2.9 g/dL | 3.5-5.0 g/dL |
| Glucose | 100 mg/dL | 70-99 mg/dL (fasting) |
| CRP | >190 mg/L | <10 mg/L |
| PCT | 4.5 ng/mL | <0.05 ng/mL |
| Lactic acid | 2.1 mmol/L | 0.5-2.2 mmol/L |
| IL-6 | 39 pg/mL | 0-5 pg/mL |
| Pleural fluid WBC | 750 /µL | <500 /µL (non-infectious) |
| Pleural fluid LDH | 200 U/L | <200 U/L (transudate) |
| Pleural fluid TP | 3.5 g/dL | <3 g/dL (transudate) |
| Pleural fluid glucose | 60 mg/dL | >60 mg/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSepsis Diagnosis and Treatment · Lymphoma Diagnosis and Treatment · Inflammatory Biomarkers in Disease Prognosis
Introduction
Hodgkin lymphomas (HLs) are malignant lymphoid neoplasms originating from B lymphocytes, most commonly involving the cervical lymph nodes. A hallmark of HL is the presence of large, atypical B cells known as Hodgkin and Reed-Sternberg cells, which play a central role in disease pathogenesis [1].
Lymphoma constitutes about 4% of all newly diagnosed cancer cases and 3.3% of cancer-related deaths in 2024 in the United States [2]. Classic HL (cHL) makes up about 10-15% of all lymphomas. The overall incidence of HL is rare, with roughly 2.6 cases per 100,000 people in the United States [3]. Numerous prognostic factors and their relationship with HL have been studied, such as age, gender, albumin, B symptoms, anemia, etc. [4].
While extensive research has examined the prognostic implications of these clinical and laboratory parameters, few studies have investigated the role of procalcitonin (PCT) in HL. PCT, a protein of 116 amino acids produced by C cells of the thyroid. PCT increases not only with bacterial infection but also with other inflammatory states, such as HL. During systemic inflammation, particularly bacterial infections, PCT levels rise significantly. This elevation is mediated by inflammatory cytokines such as interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α), which stimulate PCT production from neuroendocrine cells located in the lungs and intestine [5].
This case explores the potential relationship between PCT levels and HL, with a particular focus on evaluating PCT as a prognostic inflammatory biomarker. Understanding this association may offer insights into disease activity, treatment response, and overall prognosis in patients with HL.
Case presentation
A 61-year-old male with a significant smoking history, chronic obstructive pulmonary disease, and heart failure with reduced ejection fraction presented to the emergency department with progressive dyspnea that began two months prior and acutely worsened over the preceding three days. The patient reported a productive cough with scant white sputum. On initial evaluation, vital signs revealed hypotension (BP 100/60 mmHg), tachycardia (HR 100 bpm), hypoxemia (SpO₂ 85% on room air), and normothermia (36.9°C). Physical examination demonstrated decreased bilateral breath sounds, more pronounced on the left, with diffuse wheezing. The patient’s admission laboratory results are summarized in the table below.
The electrocardiogram showed sinus tachycardia (Figure 1).
Electrocardiogram showing sinus tachycardia
Chest radiography revealed bilateral pleural effusions, more prominent on the left, with associated left lung atelectasis (Figure 2).
Chest X-rayLarge left pleural effusion with minimal aeration of the left upper lobe.
A CT of the chest, performed with and without contrast, demonstrated a large left‑sided pleural effusion, narrowing of the left mainstem bronchus, and mediastinal as well as axillary lymphadenopathy concerning for malignancy. The neck slices revealed no evidence of metastasis involving the cervical region or thyroid gland (Figure 3).
CT chest without contrastProminent bilateral axillary lymph nodes, more pronounced on the left. A representative left axillary lymph node measures 2.3 cm in diameter (red circle). A left pleural effusion is also noted.CT: computed tomography
Further staging with abdominal MRI demonstrated splenomegaly with innumerable foci of restricted diffusion and hypoenhancement suggestive of malignant infiltration, a left adrenal mass consistent with metastasis, and an infiltrative lesion involving the left pleural space with transpleural extension. Multiple hepatic lesions were noted, the largest measuring 15 mm in the right hepatic lobe (Figure 4).
MRI of the abdomen without contrastTiny scattered foci throughout the liver, with the largest measuring 15 mm in the right hepatic lobe (blue arrow). Adrenal nodules are present (red circle). A lung lesion is also noted (green arrow).MRI: magnetic resonance imaging
Initial management included supplemental oxygen via nasal cannula (2 L/min), bronchodilator therapy (albuterol/ipratropium), oral prednisone, azithromycin, and guideline-directed medical therapy for heart failure. A left-sided chest tube was placed, draining 1.5 liters of pleural fluid over two days. Pleural fluid analysis revealed an exudative effusion with negative cultures and cytology on two separate samples.
A lymph node biopsy from the left axilla confirmed cHL, lymphocyte-rich subtype. Immunohistochemistry demonstrated positivity for CD30, CD15, PAX5, Ki-67, MOM1, and BCL6, with negative staining for CD20, CD3, LCA, and CD23. EBER-ISH highlighted abundant large atypical lymphocytes consistent with Hodgkin cells (Figure 5). Due to rapid reaccumulation of pleural fluid, a PleurX catheter was placed for ongoing drainage.
Lymph node biopsyHistopathological examination of lymph node tissue demonstrates classic features of HL. Large binucleated Reed-Sternberg cells with prominent eosinophilic nucleoli are observed (black arrow) within a mixed inflammatory background composed predominantly of small lymphocytes. Hematoxylin and eosin stain; magnification 100×, oil immersion objective.HL: Hodgkin lymphoma
A nuclear medicine bone scan showed no evidence of osseous metastasis. During the initial days of hospitalization, the patient developed intermittent fever spikes with rising PCT levels (up to 3.5 ng/mL) and declining serum albumin. Despite an extensive infectious workup, including blood, sputum, and urine cultures; CT imaging of the chest, abdomen, and pelvis; pulmonary viral and bacterial PCR panels; and a nuclear medicine white blood cell tag scan, all results were negative. Empiric broad-spectrum antimicrobial therapy was initiated (vancomycin, piperacillin-tazobactam, metronidazole, and fluconazole), yet PCT continued to rise (peak 4.5 ng/mL).
On hospital day ten, the patient developed hypotension requiring transfer to the intensive care unit, where he subsequently died. The new onset of shock was likely multifactorial, attributable to the advanced stage of HL, underlying heart failure with reduced ejection fraction, severe pleural effusion necessitating drainage every three days via a PleurX catheter, and a possible infectious process. Despite extensive evaluation, including urinalysis, blood cultures, chest radiography, and repeated tagged white blood cell scans, no infectious source was identified. A comprehensive summary of the laboratory and diagnostic workup at the time of shock is provided in Table 2.
Discussion
cHL accounts for approximately 85-95% of all HL cases [6,7]. Most patients with cHL present with lymphadenopathy. The commonly involved nodal sites include cervical, mediastinal, supraclavicular, and axillary, with some variation in site preference among different subtypes. Extranodal involvement usually arises from hematogenous dissemination, while primary extranodal disease is rare. The most commonly involved extranodal sites include the lungs, liver, and bone. cHL exhibits a bimodal age distribution with one peak in the pediatric age group and a second peak over 60 years [7].
Staging of HL is primarily determined through imaging modalities such as PET and CT, which provide critical anatomical and metabolic information. According to the Ann Arbor classification, stage I disease involves a single lymph node region or lymphoid organ (I) or a solitary extranodal site (IE). Stage II is defined by involvement of two or more lymph node regions on the same side of the diaphragm (II) or localized extranodal extension with adjacent nodal involvement (IIE). Stage III indicates lymph node involvement on both sides of the diaphragm, potentially including the spleen. Stage IV reflects disseminated disease with one or more extranodal organs affected, such as the bone marrow, liver, or lungs, with or without concurrent lymph node involvement [8]. For stage 4 HL, the chance of surviving at least five years is about 82% [9].
The patient, a 61-year-old individual, presented with clinical symptoms suggestive of lymphoproliferative disease. A diagnosis of cHL was established through axillary lymph node biopsy and flow cytometric analysis, which demonstrated B lymphocytes expressing CD30, CD15, PAX5, Ki-67, MUM1, and BCL markers. Staging CT revealed hepatic and splenic involvement, consistent with stage IV disease according to the Ann Arbor classification.
Multiple prognostic factors have been investigated in HL, with age representing a key determinant due to its association with comorbidities and decreased tolerance to chemotherapy in older patients compared to younger cohorts. Gender also influences outcomes, as males typically exhibit a poorer prognosis than females [4]. Hypoalbuminemia has been consistently associated with unfavorable clinical outcomes, a relationship that may be mechanistically explained by the suppression of hepatic albumin synthesis during inflammatory states. Specifically, the upregulation of acute-phase protein production mediated by IL-6 and the reduced availability of amino acids secondary to compromised nutritional status contribute to diminished albumin synthesis. Moreover, circulating albumin concentrations are inversely correlated with key inflammatory mediators, including IL-6, TNF-α, and IL-1RA [4,10]. In the present case, the male patient’s advanced age, concomitant heart failure with reduced ejection fraction, low serum albumin levels, and stage IV cHL likely contribute collectively to a less favorable prognosis.
Markers of systemic inflammation are frequently elevated in patients with HL, reflecting disease activity and offering potential utility as diagnostic and prognostic indicators. At the time of diagnosis, approximately 70% of HL cases exhibit elevated CRP, neutrophilic leukocytosis, and increased serum ferritin levels, while PCT typically remains within normal limits [11,12].
However, emerging evidence suggests that PCT may be elevated in more advanced stages of HL. In a study by Piperidou et al. [12], 137 newly diagnosed HL patients were evaluated, including 79 with advanced-stage disease. The authors reported that PCT levels exceeded 0.1 ng/mL in patients with advanced disease, with two cases exceeding 0.5 ng/mL (p<0.001). These findings suggest that PCT elevation may be linked to the severity of the inflammatory response in HL, potentially driven by elevated pro-inflammatory cytokines such as TNF-α and IL-6.
Although PCT is classically elevated in bacterial infections, patients in the study had negative infectious workups (blood, sputum, and urine cultures; CT imaging of the chest, abdomen, and pelvis; pulmonary viral and bacterial PCR panels; and nuclear medicine white blood cell tag scan) and were treated empirically with broad-spectrum antibiotics and antifungals without subsequent decline in PCT levels (patient’s PCT trended up to 5 ng/ml despite antibiotic and antifungal coverage). This observation supports the hypothesis that PCT elevation in HL may be independent of infection and instead reflects disease-related inflammation and prognosis.
Conclusions
These findings suggest that PCT may serve as a supplementary biomarker in HL, particularly in advanced stages of disease. Its elevation could aid prognostication and risk stratification, warranting further investigation in larger prospective cohorts. However, further research is warranted to validate this potential correlation and strengthen its role in clinical decision-making.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1An update on the pathology and molecular features of Hodgkin lymphoma Cancers (Basel) Satou A Takahara T Nakamura S 26471420223568162710.3390/cancers 14112647 PMC 9179292 · doi ↗ · pubmed ↗
- 2Global incidence, mortality and risk factors of Hodgkins and non-Hodgkins lymphoma 1990-2021: a global health data study Blood Kundu R Kal N Singh A Jagadeesh D 63601442024
- 3Hodgkin lymphoma: 2025 update on diagnosis, risk-stratification, and management Am J Hematol Ansell SM 236723789920243923979410.1002/ajh.27470 · doi ↗ · pubmed ↗
- 4Prognostic factors in hodgkin lymphoma Mediterr J Hematol Infect Dis Cuccaro A Bartolomei F Cupelli E Galli E Giachelia M Hohaus S 20140536201410.4084/MJHID.2014.053PMC 410350225045461 · doi ↗ · pubmed ↗
- 5Physiology and genetics of procalcitonin Physiol Res Maruna P NedelníkováK Gürlich R 5761492000 https://pubmed.ncbi.nlm.nih.gov/10984072/10984072 · pubmed ↗
- 6Classical Hodgkin lymphoma; real-world observations from physicians, patients, and caregivers on the disease and its treatment (CONNECT): observations of Physicians on treatment and interim PET-adapted regimens Blood Flora DR Parsons SK Liu N 13901382021
- 7Diagnosis of Hodgkin lymphoma in the modern era Br J Haematol Wang HW Balakrishna JP Pittaluga S Jaffe ES 455918420193040761010.1111/bjh.15614 PMC 6310079 · doi ↗ · pubmed ↗
- 8Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification J Clin Oncol Cheson BD Fisher RI Barrington SF Cavalli F Schwartz LH Zucca E Lister TA 305930683220142511375310.1200/JCO.2013.54.8800 PMC 4979083 · doi ↗ · pubmed ↗