Suture Fixation Versus Screw Fixation in Pediatric Tibial Eminence Fractures: A Systematic Review and Meta-Analysis of Clinical Outcomes and Reoperation Rates
Ahmed Elnewishy, Ziad El Menawy, Mohamed Zahed, Mahmoud Elmesalmi, Nour Elnaggar, Farouk Ahmed, Mahmoud Odeh, Mohamed Elgamal

TL;DR
Suture fixation is better than screw fixation for pediatric tibial eminence fractures, with fewer reoperations and hardware removals while maintaining similar stability and recovery.
Contribution
This study provides a meta-analysis comparing suture and screw fixation in pediatric tibial eminence fractures, highlighting suture fixation as a superior alternative.
Findings
Suture fixation significantly reduces reoperation frequency and hardware removal compared to screw fixation.
Return to sport rates are higher with suture fixation, with no significant differences in stability or functional recovery.
Publication bias was not detected, supporting the reliability of the findings.
Abstract
Suture fixation (SF) has gained prominence as a physeal-sparing alternative to screw fixation (SCF) in the operative management of pediatric tibial eminence fractures, aiming to reduce hardware-related complications while maintaining joint stability. This meta-analysis evaluated clinical and functional outcomes comparing SF with SCF in skeletally immature patients. A systematic review of comparative studies was conducted following the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines. Outcomes assessed included clinically relevant postoperative measures used to evaluate overall treatment success. Fixed-effect models were used to generate pooled effect estimates. Heterogeneity was quantified using the I² statistic, and publication bias was examined with funnel plots and Egger’s test. Four studies encompassing 224 pediatric patients were included. SF…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
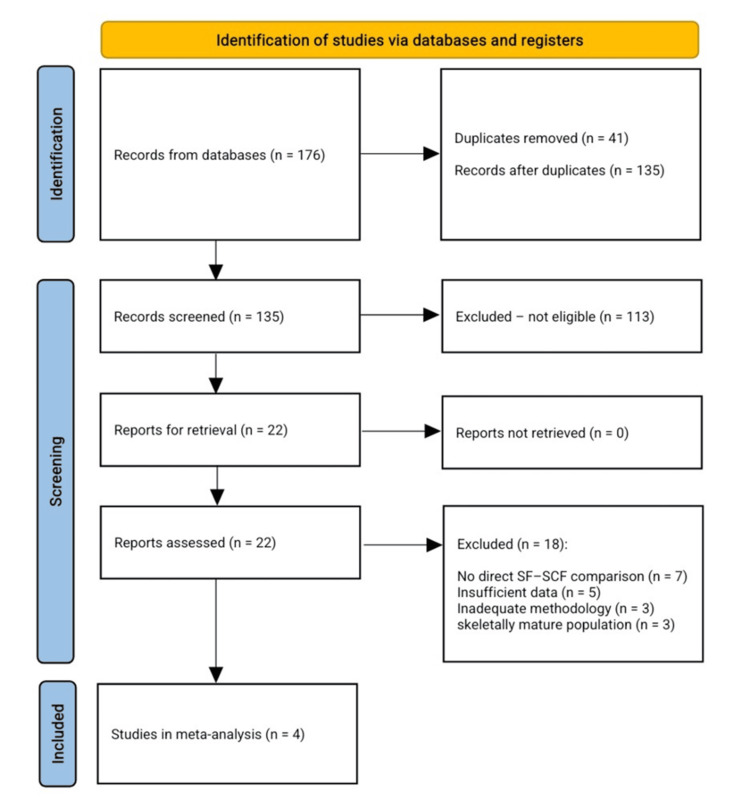 Figure 1
Figure 1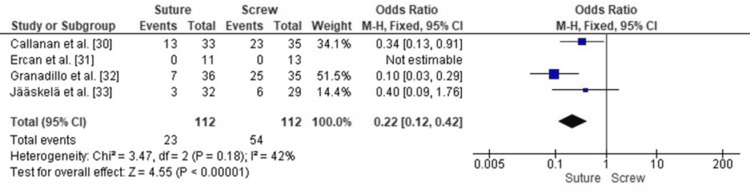 Figure 2
Figure 2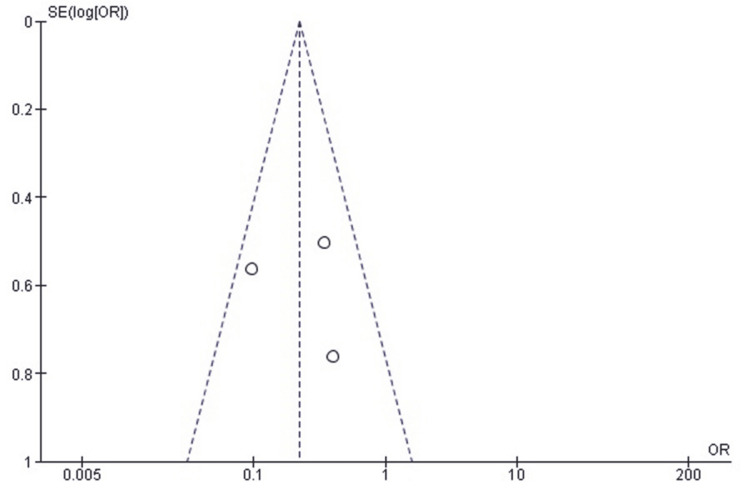 Figure 3
Figure 3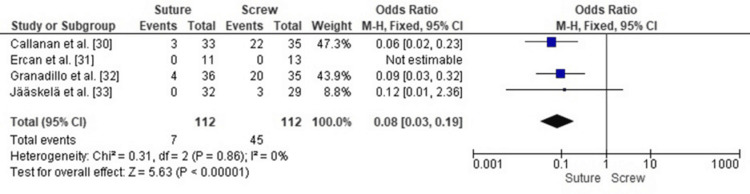 Figure 4
Figure 4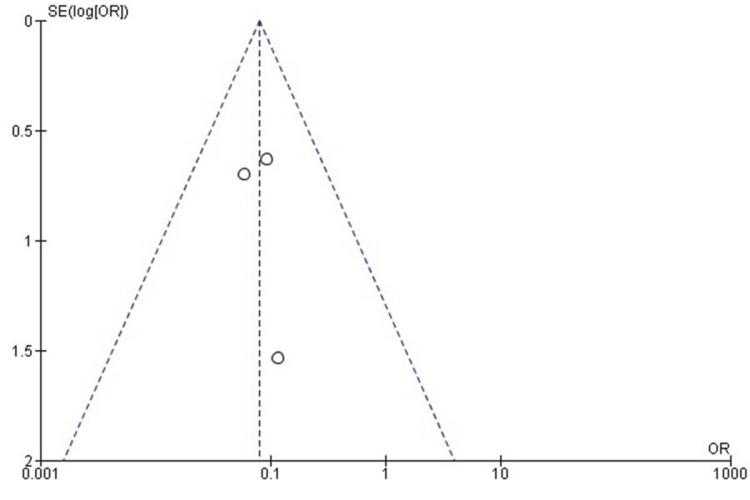 Figure 5
Figure 5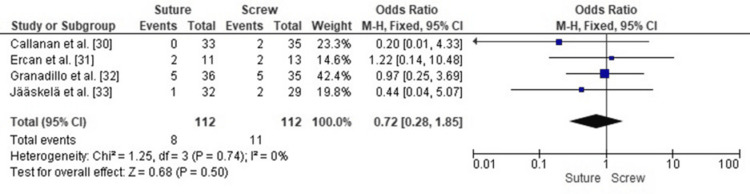 Figure 6
Figure 6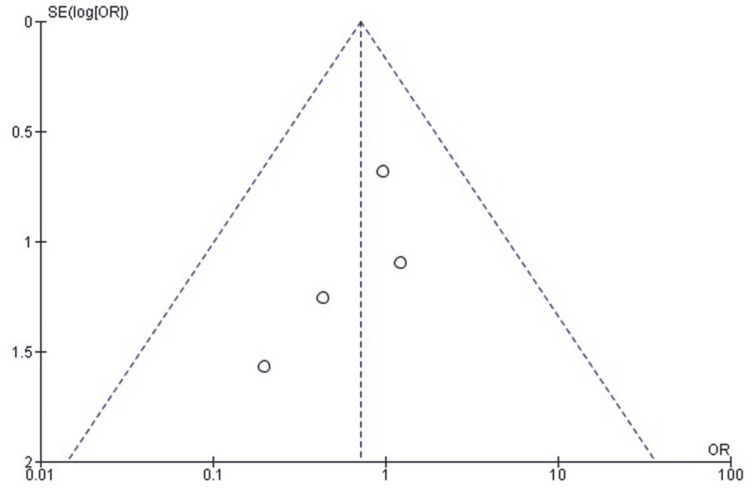 Figure 7
Figure 7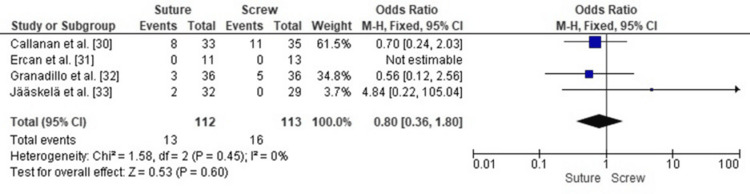 Figure 8
Figure 8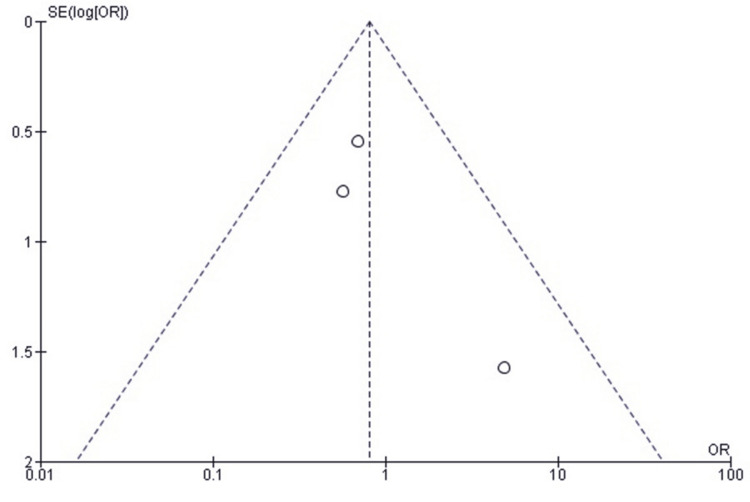 Figure 9
Figure 9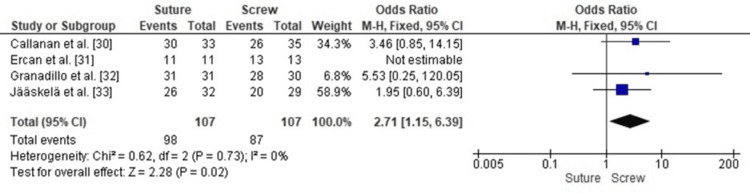 Figure 10
Figure 10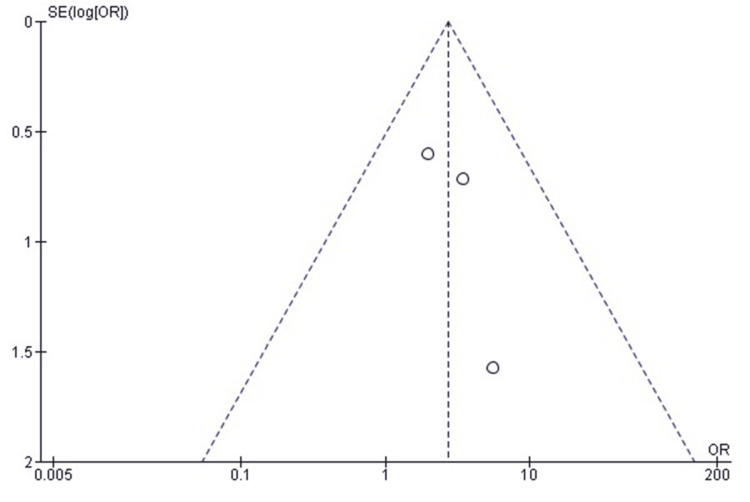 Figure 11
Figure 11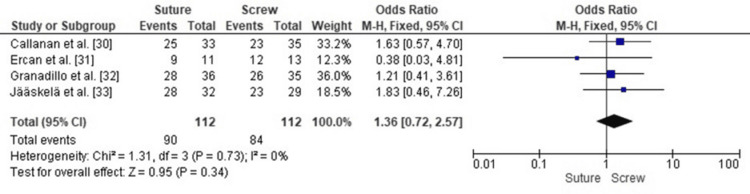 Figure 12
Figure 12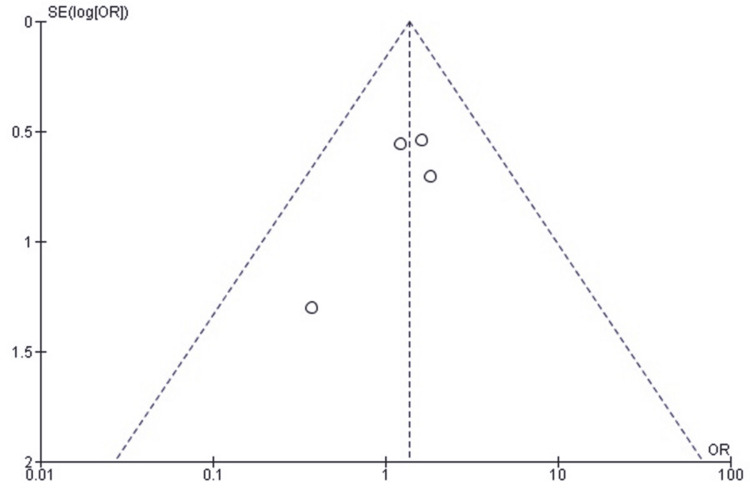 Figure 13
Figure 13| Category | Criteria |
| Inclusion criteria | Meyers-McKeever Type II or III TEFs in children with open physes |
| Comparative studies evaluating SFS and SCF | |
| Retrospective or prospective observational comparative studies | |
| Studies reporting extractable postoperative outcomes (reoperation, instability, arthrofibrosis, hardware removal, ROM, and RTS) | |
| Full-text articles published in English | |
| Exclusion criteria | Adult or skeletally mature participants |
| Mixed-age cohorts without separate pediatric analysis | |
| Single-arm case series or case reports | |
| Cadaveric or biomechanical studies | |
| Technical notes, reviews, or commentaries | |
| Conference abstracts without full data | |
| Studies lacking extractable numerical outcomes | |
| Overlapping datasets (less complete dataset excluded) |
| Category |
Callanan et al. [ |
Ercan et al. [ |
Granadillo [ |
Jääskelä et al. [ |
| Study design | Retrospective cohort, single pediatric institution (2000-2014) | Retrospective cohort (2015-2020) | Retrospective comparative case series (2000-2012) | Multicenter pediatric/young adolescent cohort |
| Sample size | 33 sutures/35 screws | 11 sutures/13 headless screws | 36 sutures/35 screws (+7 hybrid) | 32 open sutures/29 screws |
| Level of evidence | III | III | III | III |
| Patient demographics | Mean age 11.8; 72% male; type II 22%, type III 78%; meniscal entrapment 31%; meniscal tear 22% | Median age 11; similar sex distribution; minimal associated injuries; 3 meniscal tears repaired | Mean age 11.4; 68% male; 78% sports mechanism; meniscal injury predicted stiffness | Mean age 11.2; 57% male; type II-III; 14.8% concomitant injuries |
| Intervention details | Suture = tibial tunnels; screw = epiphyseal cannulated screw | Suture = Ultrabraid + tibial tunnels; screw = headless compression screw | Suture = transosseous tunnels; screw = cannulated screws/SmartNails | Suture = open osteosuture; screw = arthroscopic epiphyseal screws |
| Follow-up | Median 26 months | Minimum 2 years; median 34-42 months | Minimum 6 months; many long-term | Mean 87 months (24-189) |
| Outcome measures | ROM, instability, RTS, radiographic union, fragment elevation, reoperations | ROM, KT-1000 stability, IKDC, Lysholm, Tegner, strength, union time | ROM loss, residual pain, instability, union time, RTS, reoperations | RTP level, IKDC, QoL, displacement, regression predictors, reoperations |
| Results | Union: 3.2 mo vs 5.3 mo (P = 0.03). Fragment elevation: 5.4 vs 3.5 mm (P = 0.005). Full ROM: 76% vs 66%. Arthrofibrosis requiring surgery: 24% vs 31%. Instability: 0% vs 6%. RTS: 91% vs 74% (NS). Reoperations: 39% vs 66% (P = 0.03). Implant removal: 9% vs 62% (P < 0.001) | Operating time: 95 vs 65 min (P = 0.007). Union: 74 vs 72 days (NS). ROM: minimal deficits; no arthrofibrosis. Lysholm, Tegner, and IKDC scores similar. Stability: Lachman/pivot 0-1; KT-1000 <3 mm. Strength: symmetric. Daily activity resumed after 6 months | Whole cohort: flexion loss 22%, extension loss 42%; RTS 96%; healing ~19 weeks; mild pain 23%; instability 14%; complications 33%. Suture vs screw: tourniquet time ↑ in suture (P = 0.002). Healing 19 vs 19.7 weeks (NS). RTS 100% vs 93% (NS). Residual symptoms similar. Instability 14% both. Meniscal injury → stiffness (P = 0.002) | RTP: preinjury level 81.2% (suture) vs 69.0% (screw) (NS). Any level: 90.6% vs 89.7%. Time to RTP: 8 weeks vs 21 weeks (P < 0.05). KT-1000 >3 mm (OR 15.2) → failure to RTP; reoperation → poor IKDC (OR 19.0) |
| Complications | Arthrofibrosis requiring LOA/MUA: 24% vs 34%. ACLR 9% both. Meniscal repeat surgery 6-9%. High screw burden: removal 62%, multiple reoperations | No complications; no reoperations; no hardware removals | At least one complication: 39% vs 49% (NS). Arthrofibrosis requiring surgery: 8% vs 14%. Hardware removal: 11% vs 29%. Reinjury: 8% vs 14% | Reoperations: 9.4% vs 20.7%. Screw: pain → removal; instability → ACLR; displacement → repeat fixation. Minimal arthrofibrosis overall |
| Conclusion | Equivalent clinical outcomes, but screw = far higher reoperation and hardware removal → suture preferred | Suture and headless screw equally effective; headless screw shortens surgery and avoids a second procedure | No major differences; meniscal injury strongest predictor of stiffness; screw more likely to need removal | Both effective long-term; open suture = faster RTP and fewer failures; screw increases risk of poor RTP if reduction imperfect |
| Study | Selection | Comparability | Outcome | Total score (out of 9) |
|
Callanan et al. [ | ★★★★ | ★★ | ★★ | 8 |
|
Ercan et al. [ | ★★★ | ★★ | ★★★ | 8 |
|
Granadillo [ | ★★★★ | ★★ | ★★ | 8 |
|
Jääskelä et al. [ | ★★★★ | ★★ | ★★★ | 9 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsKnee injuries and reconstruction techniques · Bone fractures and treatments · Shoulder Injury and Treatment
Introduction and background
Tibial eminence fractures (TEFs), also known as tibial spine fractures or anterior cruciate ligament (ACL) avulsion fractures, account for nearly 14% of ACL-related injuries in children [1]. Although they constitute only 2-5% of traumatic knee effusions, TEFs are considered a significant clinical entity. The affected population predominantly comprises skeletally immature males aged 8-14 years, representing 66-70% of cases [2]. In the largest multicenter epidemiological study of 661 pediatric cases across eight institutions, the median age at injury was 12.2 years, confirming this concentration in early adolescence [2].
Biomechanically, the mechanism of TEFs is similar to ACL rupture in adults. In immature knees, incomplete ossification of the tibial spine renders the bone more susceptible to avulsion than the ligament itself [3]. TEFs account for 70.7% of proximal tibial injuries in children, as demonstrated by a recent systematic review of pediatric proximal tibial fractures [4].
Fractures of the tibial eminence occur during a period of unique structural and physiological characteristics of the growing knee [5]. The ACL inserts on the tibial eminence, located on the proximal tibial plateau, which is not fully ossified in children. This biomechanical weakness makes the bone fragment more likely to avulse under tensile or rotational stress than the ligament. The open physes (growth plates) also influence both the injury mechanism and surgical management. Implant penetration carries the risk of physeal injury and potential growth disturbance due to the close proximity of the tibial eminence to the proximal tibial physis [6]. Consequently, physeal-sparing fixation techniques, particularly all-suture or hybrid constructs, are more commonly employed [7].
Immature knees exhibit increased ligamentous elasticity and decreased subchondral bone stiffness, predisposing them to this type of avulsion pattern [8]. Fixation studies comparing suture and screw techniques suggest that skeletal maturity influences fixation strength: in immature bone, suture and screw techniques are comparable, whereas mature specimens may demonstrate greater resistance with sutures [9]. Arthroscopic, physeal-sparing techniques, such as suture pull-through or tri-pulley configurations, have demonstrated favorable outcomes [10].
ACL insertion avulsion is classically defined as a tibial spine fracture. The Meyers and McKeever classification system standardizes tibial spine avulsions based on the extent of fragment separation, guiding treatment decisions [11]. Type I fractures are nondisplaced with an intact posterior fragment. Type II fractures demonstrate beak-like anterior elevation [12]. Complete avulsion is classified as Type III, with further subclassification: Type IIIA indicates maintained anatomic position, whereas Type IIIB denotes rotation or inversion [13]. Type IV, added by Zaricznyj in 1977, includes comminuted or rotated fragments, usually following high-energy trauma [14]. MRI refinements have increased diagnostic accuracy by identifying meniscal entrapment or chondral injury not visible on plain radiographs [15]. Epidemiological studies indicate that Types II and III comprise over 80% of pediatric tibial spine injuries, most of which require operative management.
Insufficient reduction or fixation may leave the ACL elongated, causing persistent anterior laxity. Even after union, some patients experience functional instability and reduced athletic performance [16]. The most common postoperative complication is arthrofibrosis, a fibrotic contracture limiting motion, occurring in up to 30% of cases with prolonged immobilization. Early rehabilitation and range of motion (ROM) exercises greatly reduce this risk [17]. Other complications include mechanical impingement or an extension block from a prominent fragment, nonunion or malunion with angular deformity or limb-length discrepancy, and early osteoarthritic degeneration, with 18% of inadequately managed cases showing radiographic changes [18-20].
Arthroscopic suture fixation (SF) uses nonabsorbable sutures (e.g., FiberWire, ETHIBOND) passed through the ACL and secured via transtibial tunnels or anchors. This approach provides anatomic reduction and tensioning without intra-articular hardware, avoids physeal injury, and eliminates the need for implant removal. Biomechanical analyses demonstrate comparable or superior ultimate failure loads compared with screw fixation (SCF), permitting early mobilization and less postoperative stiffness [21]. Both techniques yield similar outcomes in immature knees, but sutures have fewer hardware-related complications [22].
SCF involves rigid cannulated or headless compression screws, which allow early rehabilitation. Advances such as smaller screw diameters (3-5 mm) and bioabsorbable materials have reduced hardware impingement and, in select cases, obviated the need for removal [23,24]. Comparative meta-analyses show that screws and SF provide similar stability and function, but screws carry a higher reoperation rate due to hardware-related complications [25,26]. More recent evidence indicates that SF is associated with superior Lysholm and IKDC scores and fewer postoperative issues, whereas screws are associated with shorter operative times but increased removal rates [27,28].
This systematic review and meta-analysis integrates current evidence comparing suture constructs and SCF, aiming to assess clinical and functional outcomes in children with TEFs.
Review
Methods
Search Strategy
A comprehensive literature search was conducted in November 2025 across PubMed, Scopus, Web of Science, Embase, and the Cochrane Library to identify studies comparing SF and SCF for the management of pediatric TEFs. The search strategy combined Medical Subject Headings (MeSH) and free-text terms, including “tibial eminence fracture”, “tibial spine avulsion”, “intercondylar eminence fracture”, “suture fixation”, “transosseous suture”, “screw fixation”, “arthroscopic fixation”, and “pediatric knee trauma”. Reference lists of all eligible full-text studies and relevant systematic reviews were manually screened to identify any additional suitable publications.
Inclusion Criteria
Studies were included if they involved pediatric patients with open physes and Type II or III TEFs according to the Meyers-McKeever classification. Only comparative observational studies, either prospective or retrospective, directly comparing SF with SCF were considered. Eligible studies needed to report sufficient outcome data to allow meta-analysis, including postoperative functional outcomes, reoperation rates for instability, arthrofibrosis, hardware removal, or other re-interventions. Only articles published in English and available in full text were included.
Exclusion Criteria
Studies were excluded if they lacked a direct comparison between suture and SCF or did not provide extractable numerical outcomes for relevant endpoints. Additional exclusion criteria included studies with skeletally mature participants or mixed-age cohorts without pediatric subgroup stratification, single-arm case series, case reports, cadaveric or biomechanical studies, surgical technique descriptions, reviews, commentaries, or conference abstracts. In instances of overlapping patient datasets, the study with the most complete and clearly reported cohort was selected.
A summary of the inclusion and exclusion criteria is provided in Table 1.
Outcome Measures
The primary outcomes of interest were reoperation rate, hardware removal rate, postoperative knee instability, and arthrofibrosis requiring surgical intervention, as these represent the most clinically significant complications following operative fixation. Secondary outcomes included return to sport (RTS) and full ROM recovery, which reflect functional recovery. Collected demographic variables, details of the fixation technique, and follow-up duration provided context for interpreting treatment effects across studies.
Data Extraction and Quality Assessment
Data were extracted using predesigned standardized forms to record study characteristics, patient demographics, fracture classification, fixation technique, follow-up duration, and all reported postoperative outcomes. Extraction was performed independently and cross-checked for accuracy, with disagreements resolved by consensus. The methodological quality of included studies was assessed using the Newcastle-Ottawa Scale (NOS), which evaluates study selection, comparability of intervention groups, and reliability of outcome assessment [29]. Each study received a total NOS score and was classified as low, moderate, or high quality according to established criteria.
Statistical Analysis
All statistical analyses were performed using Review Manager (RevMan v5.4, The Cochrane Collaboration) [26]. ORs with 95% CIs were used to pool results for dichotomous outcomes. Fixed-effect or random-effects models were chosen based on heterogeneity. When heterogeneity was low (I² < 50% on the chi-square test), a fixed-effect model was adopted. Egger’s regression method and visual inspection of funnel plots were used to assess publication bias, with a two-tailed p-value < 0.05 considered statistically significant.
Results
Search Result and Study Selection
A comprehensive systematic search was conducted to identify studies comparing SF and SCF for the management of pediatric TEFs. The initial search across all databases and reference lists yielded 176 records. After removing 41 duplicates, 135 unique studies remained for title and abstract screening. During this phase, 113 records were excluded for not meeting the predefined eligibility criteria. The most common reasons for exclusion were non-comparative study designs, lack of a direct SF-SCF comparison, adult or mixed-age populations without pediatric stratification, single-arm case series, biomechanical or cadaveric studies, technical notes, reviews, and studies without extractable clinical outcomes.
Following this stage, 22 full-text articles were assessed for eligibility. After detailed evaluation, 18 studies were excluded due to reasons such as absence of a direct SF-SCF comparison, insufficient or non-extractable data, inadequate methodology or follow-up, or inclusion of a skeletally mature population. Ultimately, four studies met all inclusion criteria and were incorporated into the final qualitative and quantitative synthesis.
The complete study selection process is presented in Figure 1.
PRISMA flowchart for the included studiesPRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses; SCF, screw fixation; SF, suture fixation
Study Characteristics
The four studies included in the final synthesis collectively evaluated 224 pediatric patients with TEFs managed operatively using either SF or SCF. Among these patients, 112 underwent suture-based fixation, and 112 received screw-based fixation. All studies focused exclusively on skeletally immature patients with Meyers-McKeever type II or III tibial spine avulsion injuries and provided comparable demographic and clinical details. The mean age across cohorts ranged from 10.9 to 11.8 years.
Despite variation in sample size and follow-up duration, all studies consistently reported extractable outcomes, including radiographic union, postoperative knee stability, ROM, RTS, complications such as arthrofibrosis or hardware-related symptoms, and the need for reoperation. These characteristics enabled a structured comparison of clinical and functional results between suture- and screw-based fixation techniques.
A detailed summary of the key characteristics of the included studies is presented in Table 2.
Quality Assessment of the Included Studies
Study quality was evaluated using the NOS, which assesses methodological rigor across three key domains: cohort selection, comparability of groups, and outcome assessment. Each study was assigned a rating based on the number of stars awarded in each domain. Studies were subsequently categorized as low, moderate, or high quality according to their total NOS scores. Table 3 presents the detailed quality assessment for each included study.
Results of the meta-analysis
Comparison of Reoperation Rates Between SF and SCF in Pediatric TEFs
A forest plot analysis of reoperation rates in pediatric TEFs treated with SF and SCF demonstrated a statistically significant lower reoperation rate for SF (pooled OR 0.22, 95% CI: 0.12-0.42, p < 0.00001), corresponding to a 79% lower risk of reoperation for children treated with SF compared with SCF.
Heterogeneity across the included studies was low (I² = 42%, p = 0.18), indicating minimal variability in study designs, populations, or fixation techniques. This enhances the validity of the pooled effect, demonstrating that the reduced risk of reoperation with SF is a robust and reproducible finding across the available evidence (Figure 2).
Forest plot comparing SF and SCF for reoperation ratesSCF, screw fixation; SF, suture fixationSources: [30-33]
Publication Bias Assessment for Reoperation Rate
A funnel plot of the effect estimates (Figure 3) showed that the distribution of effect estimates was roughly symmetrical. Minor asymmetry was likely attributable to differences in study size and standard error rather than selective reporting or systematic publication bias. Egger’s regression test was not statistically significant (p > 0.05), suggesting that the observed pattern is consistent with random variation and not due to small-study effects.
Funnel plot assessing publication bias for studies comparing SF and SCF regarding reoperation ratesSCF, screw fixation; SF, suture fixation
Comparison of Hardware Removal Rates Between SF and SCF in Pediatric TEFs
Forest plot analysis comparing hardware removal rates between suture and SCF demonstrated a statistically significant difference, with SCF associated with a markedly higher need for hardware removal. The pooled OR was 0.08 (95% CI: 0.03-0.19, p < 0.00001), indicating that children treated with SF were 92% less likely to require hardware removal compared with those treated with SCF.
Heterogeneity across the included studies was very low (I² = 0%, p = 0.86), indicating highly consistent effect estimates across study designs and populations. This confirms that the reduced hardware removal burden with SF is a robust finding across the available evidence (Figure 4).
Forest plot comparing SF and SCF for hardware removal ratesSCF, screw fixation; SF, suture fixationSources: [30-33]
Publication Bias Assessment for Hardware Removal Rate
A funnel plot was used to evaluate publication bias, showing approximately symmetrical study estimates. Minor asymmetry was likely due to variation in standard error and sample size rather than publication bias (Figure 5). Egger’s regression test was not statistically significant (p > 0.05), supporting the interpretation that any asymmetry is random rather than due to bias or small-study effects.
Funnel plot assessing publication bias for studies comparing SF and SCF regarding hardware removal ratesSCF, screw fixation; SF, suture fixation
Comparison of Postoperative Knee Instability Between SF and SCF in Pediatric TEFs
A forest plot analysis comparing postoperative knee instability in pediatric TEFs treated with SF versus SCF showed no statistically significant difference between the two fixation techniques (pooled OR 0.72, 95% CI: 0.28-1.85, p = 0.50). Heterogeneity across the included studies was negligible (I² = 0%, p = 0.74), indicating consistent effect estimates across study populations and methodologies, enhancing the reliability of the pooled analysis, and confirming that the similarity in instability rates between SF and SCF was not due to variability in the evidence (Figure 6).
Forest plot comparing SF and SCF for postoperative knee instabilitySCF, screw fixation; SF, suture fixationSources: [30-33]
Publication Bias Assessment for Postoperative Knee Instability
A funnel plot indicated an approximately symmetrical distribution of study estimates (Figure 7), suggesting any minor asymmetry was likely due to differences in standard error and small sample sizes rather than systematic publication bias. Egger’s regression test showed no statistically significant evidence of publication bias (p > 0.05).
Funnel plot assessing publication bias for studies comparing SF and SCF regarding postoperative knee instabilitySCF, screw fixation; SF, suture fixation
Comparison of Arthrofibrosis Requiring Surgery Between SF and SCF in Pediatric TEFs
Forest plot analysis comparing rates of arthrofibrosis requiring surgical intervention revealed no statistically significant difference between SF and SCF (pooled OR 0.80, 95% CI: 0.36-1.80, p = 0.60). Heterogeneity was extremely low (I² = 0%, p = 0.45), indicating stable effect estimates across populations and surgical techniques, supporting the conclusion that neither method offers a significant advantage in preventing postoperative arthrofibrosis requiring operative management (Figure 8).
Forest plot comparing SF and SCF for arthrofibrosis requiring surgerySCF, screw fixation; SF, suture fixationSource: [30-33]
Publication Bias Assessment for Arthrofibrosis Requiring Surgery
A funnel plot was used to assess publication bias and demonstrated an approximately symmetrical distribution of the study effect estimates (Figure 9). This symmetry is most likely attributable to differences in sample size and standard error among the included studies rather than selective outcome reporting. Egger’s regression test showed no statistically significant evidence of publication bias (p > 0.05), further supporting that the observed distribution reflects random variation rather than small-study effects or systematic bias.
Funnel plot assessing publication bias for studies comparing SF and SCF regarding arthrofibrosis requiring surgerySCF, screw fixation; SF, suture fixation
Comparison of RTS Between SF and SCF in Pediatric TEFs
Forest plot analysis comparing RTS in patients treated with SF versus SCF for pediatric TEFs demonstrated a statistically significant advantage for SF (OR 2.71; 95% CI: 1.15-6.39, p = 0.02). Heterogeneity across the included studies was very low (I² = 0%, p = 0.73), indicating a consistent effect estimate across different clinical settings, populations, and study designs. This consistency reinforces the reliability of the pooled findings and supports the conclusion that SF more consistently facilitates return to athletic activity following tibial spine avulsion repair (Figure 10).
Forest plot comparing SF and SCF for RTSRTS, return to sport; SCF, screw fixation; SF, suture fixationSources: [30-33]
Publication Bias Assessment for RTS
Publication bias was evaluated using a funnel plot, which showed an approximately symmetrical distribution of study estimates (Figure 11). Minor asymmetry was observed, likely due to variations in sample size and standard errors rather than true publication bias. Egger’s regression test showed no statistically significant evidence of publication bias (p > 0.05).
Funnel plot assessing publication bias for studies comparing SF and SCF regarding RTSRTS, return to sport; SCF, screw fixation; SF, suture fixation
Comparison of Full ROM Recovery Between SF and SCF in Pediatric TEFs
A forest plot analysis comparing ROM recovery for SF versus SCF in pediatric TEFs showed no statistically significant difference between the two fixation methods (pooled OR 1.36, 95% CI: 0.72-2.57, p = 0.34).
Heterogeneity across the included studies was low (I² = 0%, p = 0.73), indicating that the results were consistent across study designs, populations, and surgical approaches (Figure 12). Therefore, neither fixation method demonstrated a clear advantage in restoring full knee ROM following surgical repair.
Forest plot comparing SF and SCF for full ROM recoveryROM, range of motion; SCF, screw fixation; SF, suture fixationSources: [30-33]
Publication Bias Assessment for Full ROM Recovery
A funnel plot was used to evaluate publication bias, and the distribution of study effect estimates was approximately symmetrical, with minor asymmetry likely due to the differences in standard error and sample size rather than selective reporting or small-study effects (Figure 13); Egger’s regression test showed no statistically significant evidence of publication bias (p > 0.05).
Funnel plot assessing publication bias for studies comparing SF and SCF regarding full ROM recoveryROM, range of motion; SCF, screw fixation; SF, suture fixation
Discussion
A review comparing SF and SCF for pediatric TEFs found that although both fixation techniques resulted in satisfactory union and functional outcomes, SF was associated with fewer reoperations and hardware-related complications [30]. Pooled results showed that SF significantly reduced the rate of reoperation compared with SCF [30,32,33], with reoperation rates of 39% in patients treated with sutures versus 66% in the SCF group [30], 39% versus 49% [32], and 9.4% versus 20.7% for open osteosuture and arthroscopic SCF groups, respectively [33]. A recent meta-analysis by Manaf et al. [26] confirmed these findings, reporting a significantly higher risk of secondary surgery and complications with SCF. However, Ercan et al. [31] did not report any reoperations in either group when using headless compression screws, suggesting that modern screw designs may reduce hardware-related issues.
SF also showed a clear advantage in reducing hardware removal, with 62% of patients in the SCF group requiring implant removal compared with 9% in the SF group (Callanan et al. [30]), 29% versus 11% (Granadillo [32]), and 10% versus 0% (Jääskelä et al. [33]). Ercan et al. [31] found that headless screws minimized this issue, achieving results similar to SF. This reflects inherent design differences between the methods: screws, particularly metallic ones, can protrude into the joint, causing impingement or irritation, whereas sutures are intra-articularly smooth and rarely require removal. Across most studies, SF consistently avoided the need for secondary hardware removal procedures.
There was no significant difference in postoperative knee stability between the fixation techniques. Fourteen percent of patients in both groups reported subjective instability, with equivalent objective stability [32]. Callanan et al. [30] found no difference in laxity or reinjury rates, and Ercan et al. [31] reported symmetric stability with side-to-side KT-1000 differences below 3 mm for both groups. Jääskelä et al. [33] also found no differences in anterior tibial translation or pivot-shift test outcomes. Biomechanical studies by Thome et al. [9] demonstrated similar stiffness under cyclic loading for both techniques, and Ye et al. [22] reported equivalent displacement after mechanical testing.
The rate of arthrofibrosis requiring intervention was not significantly different between the fixation methods. Postoperative stiffness occurred in 24% of suture-treated patients and 31% of screw-treated patients [30], while Granadillo [32] reported arthrofibrosis in 8% of the suture group and 14% of the screw group. Ercan et al. [31] and Jääskelä et al. [33] found no differences between groups. These findings support Coyle et al.’s [14] hypothesis that arthrofibrosis is more closely associated with prolonged immobilization and delayed rehabilitation than with the type of fixation.
RTS rates were generally higher and faster with SF. Jääskelä et al. [33] reported a median return at eight weeks for osteoSF compared with 21 weeks for SCF. Callanan et al. [30] reported 91% versus 74%, and Granadillo [32] reported 100% versus 93% for suture versus SCF, respectively. Ercan et al. [31] found all patients in both groups returned to activity by six months, suggesting parity in long-term outcomes. The earlier return with SF may reflect reduced hardware irritation and earlier initiation of motion exercises. Wien Aryana [11] similarly noted that suture constructs do not impede early rehabilitation.
Excellent recovery of ROM was observed in both fixation methods. Callanan et al. [30] reported 76% full ROM in the suture group versus 66% in the screw group. Ercan et al. [31] found nearly identical outcomes, and Granadillo [32] and Jääskelä et al. [33] reported comparable flexion-extension arcs at final follow-up. These findings align with biomechanical studies by Ye et al. [22] and Thome et al. [9], showing similar fixation stiffness and displacement resistance. Callanan et al. [30] noted minor extension loss in a few screw-treated cases, likely due to notch impingement or fragment elevation.
Limitations
This systematic review has limitations due to heterogeneity in study design, sample size, and follow-up duration among included studies. Most studies were retrospective, which may introduce bias. Variations in surgical techniques and postoperative rehabilitation protocols may also influence outcomes. Nevertheless, the consistency of findings across studies supports their validity.
Conclusions
Our meta-analysis indicates that SF is superior to SCF regarding reoperation rates, hardware-related procedures, and RTS outcomes, while showing no significant differences in union rates, recurrent instability, or knee ROM. These findings suggest that SF may be the preferred technique for select pediatric patients, particularly when aiming to minimize implant burden and avoid secondary procedures. However, high-quality, prospective, and comparative studies with standardized surgical techniques and outcome measures are limited. Further research is needed to definitively establish the optimal role of SF in managing pediatric TEFs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tibial spine fracture type I in a 6 years old patient: complications and treatment J Orthop Sports Med Nicolini P 12313232021
- 2Poster 246: Epidemiology of tibial spine fractures in children: a national multicenter study Orthop J Sports Med Stevens A Patel N Cruz A 2325967123112023
- 3Tibial spine avulsion fractures: current concepts and technical note on arthroscopic techniques used in management of these injuries Regional Arthroscopy Sapre V Bagaria V London Intech Open 2013
- 4High incidence of soft tissue injury in pediatric proximal tibia fractures: a systematic review Arthrosc Sports Med Rehabil Sanders E Policicchio AL Phillips L 100771520233757690910.1016/j.asmr.2023.100771 PMC 10415616 · doi ↗ · pubmed ↗
- 5Avulsion fracture of the tibial eminence in an adult with a unique mechanism of injury Radiol Case Rep Patterson SP Christiansen GB Daffner RH 8438471320183000278510.1016/j.radcr.2018.05.015PMC 6040231 · doi ↗ · pubmed ↗
- 6Hybrid fixation of tibial eminence fractures in skeletally immature patients Arthrosc Tech Gans I Babatunde OM Ganley TJ 0422201310.1016/j.eats.2013.02.013PMC 383464724265991 · doi ↗ · pubmed ↗
- 7Physeal-sparing tibial eminence fracture fixation with a headless compression screw Orthopedics Johnson DL Durbin TC 6046083520122278488910.3928/01477447-20120621-08 · doi ↗ · pubmed ↗
- 8The tibial eminence fracture in skeletally immature patients Curr Opin Pediatr Shin YW Uppstrom TJ Haskel JD Green DW 50572720152550289610.1097/MOP.0000000000000176 · doi ↗ · pubmed ↗