Electronic Health Record Burnout in Surgery and Strategies to Improve Burnout: A Narrative Review
Allison Karwoski, Nicholas Hricz, Kevin Schlidt, Yvonne M Rasko

TL;DR
This review explores how electronic health records contribute to surgeon burnout in the U.S., focusing on documentation and time demands as key factors.
Contribution
The study identifies specific EHR-related burnout contributors among U.S. surgeons and suggests practical mitigation strategies.
Findings
Documentation burden and time demands are the most frequently reported EHR-related contributors to surgeon burnout.
Electronic messaging and usability also contribute to burnout, though less frequently reported.
Practical solutions include efficiency tactics like templates and system-level usability improvements.
Abstract
Physician burnout is a prevalent occupational syndrome characterized by emotional exhaustion, depersonalization, and diminished professional efficacy. Use of electronic health records (EHRs; also termed EMRs) has been associated with provider burnout in multiple settings. This review characterizes the most frequently reported EHR‑related contributors to burnout among U.S. surgeons across the following four domains: documentation burden, time demands (including after‑hours work), electronic messaging/in‑basket load, and usability. We searched PubMed for English-language, U.S. articles published from January 2004 to April 2024. Two reviewers independently screened and domain‑coded with consensus resolution. We report domain frequencies as n (%) with 95% confidence intervals (CIs) (Wilson) and summarize study‑level magnitudes where available (e.g., hours/day in EHR, after‑hours share,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
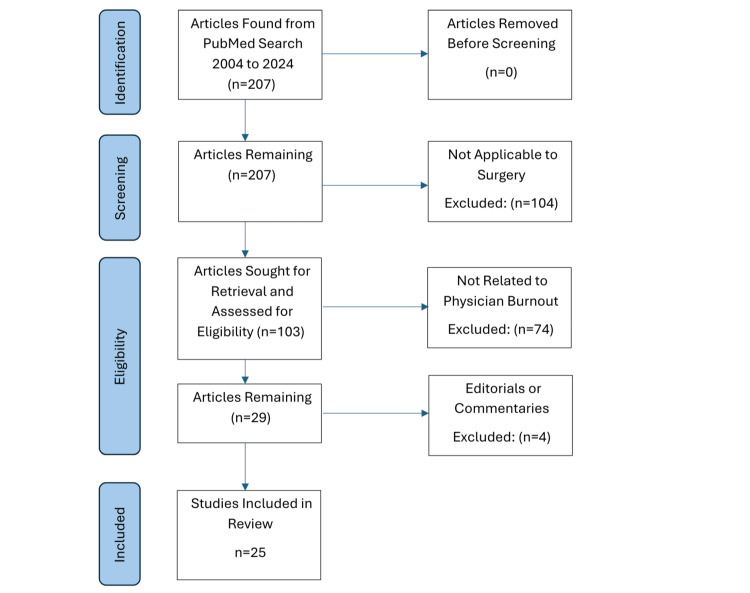 Figure 1
Figure 1| Source (authors, year; ref) | Potential source of burnout | |||
| Documentation burden | Usability | Time demands (including after-hours/remote use) | Electronic messaging | |
|
Malay, 2020 [ | X | NA | X | NA |
|
Cox et al., 2021 [ | NA | X | X | NA |
|
Ebbers et al., 2022 [ | X | X | X | NA |
|
Dymek et al., 2021 [ | X | NA | NA | X |
|
Yan et al., 2021 [ | X | NA | X | X |
|
Lilly et al., 2019 [ | NA | NA | X | NA |
|
Kesler et al., 2022 [ | NA | NA | X | X |
|
Somerson et al., 2020 [ | X | NA | X | NA |
|
Victores et al., 2014 [ | NA | NA | X | NA |
|
Coleman et al., 2021 [ | X | NA | X | NA |
|
McPeek-Hinz et al., 2021 [ | X | NA | X | NA |
|
Lin et al., 2021 [ | NA | X | NA | NA |
|
Bahr et al., 2023 [ | NA | X | NA | NA |
|
Ho et al., 2023 [ | X | NA | X | NA |
|
Drudi et al., 2022 [ | X | NA | NA | NA |
|
Carayon et al., 2015 [ | X | NA | X | NA |
|
Aziz et al., 2019 [ | X | NA | X | X |
|
Wormer et al., 2015 [ | X | NA | X | NA |
|
Ham et al., 2016 [ | X | NA | X | NA |
|
Shenson et al., 2016 [ | NA | NA | NA | X |
|
Sun et al., 2018 [ | NA | NA | NA | X |
|
Cronin et al., 2015 [ | NA | NA | NA | X |
|
Congelosi et al., 2023 [ | NA | NA | X | X |
|
Crowson et al., 2016 [ | X | NA | X | NA |
|
Freiburg et al., 2011 [ | X | NA | NA | NA |
| Domain | Studies reporting as contributor (n/N) | % of studies | 95% CI (Wilson) |
| Documentation burden | 15/25 | 60.0% | 40.7–76.6% |
| Time demands | 17/25 | 68.0% | 48.4–82.8% |
| Electronic messaging | 8/25 | 32.0% | 17.2–51.6% |
| Usability | 4/25 | 16.0% | 6.4–34.7% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealthcare professionals’ stress and burnout · Hospital Admissions and Outcomes · Electronic Health Records Systems
Introduction and background
Electronic health record (EHR) systems, also termed electronic medical records (EMRs), were introduced to improve clinical efficiency, accessibility, and reliability of patient information [1]. First introduced in the 1970s, EHR use has increased steadily, with broad adoption across U.S. hospitals and office-based practices [2]. EHRs have been linked to increased adherence to evidence-based care and safety improvements, including fewer medication errors, fewer unnecessary tests, improved anticoagulation prophylaxis adherence, increased vaccination rates, and lower mortality [3-7]. Recent narrative reviews of physician and medical student burnout further underscore the need for multilevel strategies to address this syndrome [8]. However, integration into clinical workflow can be associated with burnout among surgical professionals. The magnitude of this association varies by specialty, role, and study design [9-11].
Physician burnout is a prevalent syndrome with components of depersonalization, exhaustion, and a diminished sense of accomplishment [11]. In repeated surveys of U.S. physicians, burnout prevalence increased from ~35% to ~56% in some samples between 2013 and 2020 [12-15]. Surgeons have elevated risk and consequences, including substance misuse, attrition, interpersonal strain, suicidal ideation, depression, and potential impacts on patient outcomes [16-19]. Consistent with observational evidence, we use association language throughout and pre-specify four domains to align the Introduction and Results: documentation burden, time demands (including after-hours use), electronic messaging/in basket load, and usability [9-11]. We also note that well‑implemented EHR features (e.g., standardized order sets, dashboards, team-based messaging rules, voice dictation) can reduce friction in some workflows. Because EHR configurations, documentation requirements, and policy incentives differ across countries, we focused on U.S.-based studies to provide a coherent and policy-relevant synthesis. Our objective was to characterize the most frequently reported EHR-related contributors to burnout among U.S. surgeons across these four domains and outline practical, evidence-aligned strategies.
Review
Methodology
Search Criteria
We searched PubMed on April 30, 2024, for studies from January 1, 2004, through April 30, 2024. A Preferred Reporting Items for Systematic reviews and Meta-Analyses literature search extension (PRISMA‑S) compliant strategy with Boolean terms, MeSH, date limits, and filters appears in Appendix 1. In brief, we combined EHR/EMR terms (“Electronic Health Records”[Mesh] OR EHR* OR EMR* OR “electronic medical record*” OR “health information technolog*”), burnout/stress terms (“Burnout, Professional”[Mesh] OR burnout OR stress OR workload OR “time demand*” OR inbox OR messag* OR usabilit*), and surgical terms (“Surgery”[Mesh] OR surg* OR otolaryngology OR orthopedic* OR vascular surgery OR surgical oncology OR intensive care OR ICU). Limits: English; Humans; 2004-2024. We hand‑searched reference lists of included articles. No protocol was registered (e.g., Open Science Framework); this is stated as a limitation.
Inclusion and Exclusion Criteria
We included U.S.‑based English-language studies published from 2004 to 2024, addressing surgeons/surgical trainees/surgical services and reporting EHR‑related burnout or stress/workload linked to burnout (qualitative or quantitative). We excluded non-surgical, non-burnout-related editorials/commentaries. Mixed populations (e.g., intensive care unit (ICU) including non‑surgeons) were included if informative to surgical workflows and flagged in text. A total of 207 records were screened, of which 25 met the inclusion criteria (Figure 1).
Reporting Items for Systematic reviews and Meta-Analyses flowchart of study selection.
Data Extraction, Coding, and Inter‑rater Reliability
Eligibility was assessed by the first and second authors. Two authors independently coded whether each of the four domains (documentation, time demands, electronic messaging, usability) was reported as a contributor to burnout. A codebook (Appendix 2) defined each domain and decision rules for “contributor” (1), “assessed but not contributor” (0), and “not assessed” (NA) with verbatim criteria/examples. We computed percent agreement (P₀) and Cohen’s kappa (κ) for each domain, excluding NA codes. Agreement was moderate across domains (κ = 0.38-0.61).
Summary Methods and Statistics
Given heterogeneity, we conducted a structured narrative synthesis. To provide statistical context beyond counts, we report domain frequencies as n (%) with 95% Wilson score confidence intervals (CIs). Where available, we also summarized key design features, burnout measures, and EHR exposure definitions for each included study in Appendix 3 as a brief methodological appraisal; we did not apply a formal risk-of-bias scoring tool. Sensitivity tallies limited to validated burnout measures (e.g., Maslach Burnout Inventory (MBI)) and comparable exposure metrics (e.g., after‑hours %) were pre‑specified but constrained by reporting heterogeneity; we describe these plans in Appendix 2 and temper conclusions accordingly.
Results
We screened 207 records, of which 25 studies met the inclusion criteria for this narrative synthesis (Figure 1). Studies spanned general surgery, vascular surgery, orthopedics, otolaryngology, surgical oncology, and surgical intensive care (SICU). Sample compositions included attending surgeons, surgical residents, and mixed surgical services.
Coding Approach and Table Conventions
Each included article was domain‑coded for whether it reported an EHR‑related contributor to burnout in four a priori domains, namely, documentation burden, time demands (including after‑hours/remote use), electronic messaging/in‑basket load, and usability. In Table 1, an “X” denotes that the domain was reported as a contributor in that study; empty cells indicate the domain was assessed but not identified as a contributor. A brief verbatim‑trigger codebook (criteria/examples) is shown in Appendix 2.
Domain Frequencies With Confidence Intervals
Across the 25 studies, the most frequently reported EHR‑related contributors were time demands and documentation, followed by electronic messaging and usability (Table 2). We present Wilson 95% CIs to add statistical context to simple tallies.
Stratified Descriptive Summaries
Given heterogeneous designs and reporting, we provide descriptive stratifications (see Appendix 3 for study-level details by specialty, role, setting, and era).
By specialty (general/vascular/orthopedics/ENT/oncology/SICU): In each specialty cluster, time demands and documentation remained the top two reported domains. Messaging burden appeared most often in services with high outpatient follow‑up and portal use; usability issues surfaced around transitions and downtime.
By role (attending vs. resident): Residents more often reported after‑hours EHR time and duty‑hour implications; attendings more often reported remote/nighttime EHR use and in‑basket load.
By setting (outpatient vs. inpatient/ICU): Outpatient settings emphasized documentation and messaging, whereas ICU/inpatient settings emphasized task volume, task switching, and workflow complexity within the EHR.
By era (2004-2012, 2013-2019, 2020-2024): Studies from 2020-2024 more frequently mentioned portal messaging growth and remote access patterns; the overall rank order of domains (time, documentation > messaging > usability) did not change directionally.
Sensitivity Notes
Where studies used validated burnout instruments (e.g., MBI) or comparable exposure metrics (e.g., hours/day in EHR, after‑hours %), the directional pattern (time/documentation most frequently reported) was unchanged. Because of small strata and reporting heterogeneity, we did not perform inferential comparisons or meta‑analysis of effect sizes. Selected study‑level magnitudes (e.g., EHR hours/day, remote use share, odds ratios linking inbox volume or documentation time to burnout) are summarized in Appendix 3 for context.
Other Observations
None of the included studies explicitly assessed medicolegal contributors to burnout; this likely reflects the scope of the search and study aims rather than proof of no effect.
Discussion
We identified 25 U.S. studies relevant to EHR‑related burnout in surgical settings spanning general surgery, vascular surgery, orthopedics, otolaryngology, surgical oncology, and ICU care. Across these studies, the most frequently reported contributors were time demands and documentation burden, with additional contributions from electronic messaging and usability (Tables 1, 2). To avoid over‑interpretation of heterogeneous observational evidence, our statements reflect associations rather than causation. Where available, we summarize study‑level magnitudes (e.g., hours/day in the EHR, after‑hours share, message volume, odds ratios) without aggregating across unlike populations or settings. None of the included studies explicitly assessed medicolegal contributors; this likely reflects scope/search limits rather than the absence of an effect. Finally, we direct readers to Table 2 (domain frequencies with 95% CIs) and Appendix 3 (select effect estimates) for a statistical context that goes beyond simple tallies.
Documentation
In U.S. surgical practice, documentation burden is consistently associated with burnout signals. Studies describe long, billing‑oriented notes, copy‑forward content, and extensive data entry that enlarge cognitive load and divert attention from patient‑facing work [45-47]. For context, ambulatory time‑motion data show substantial portions of the workday devoted to EHR/desk tasks; specialty and oncology clinics similarly report intensive documentation effort during visits. We emphasize that these estimates come from different roles and settings (e.g., ambulatory attendings vs. disease‑specific clinics) and therefore are not additive. Together, they support the qualitative pattern that documentation processes, i.e., note composition, order entry, and chart review, are frequently cited alongside burnout measures in surgical environments [48-54].
Time Demands
Surgeons have the highest mean annual hours worked of all specialties (+303 hours over average); additional time spent navigating EHRs detracts from other patient care, self-care, or other important life events [55]. One study found that surgeons, when they fail to balance administrative and clinical demands with their personal lives, gave their personal lives a lower priority [56]. Across several included studies, approximately 17% of EMR encounters occurred outside of scheduled working hours, underscoring the extent of after-hours work [22,32,57]. EMR usage at home was associated with increased odds of burnout [53]. In a time‑use analysis of academic surgeons, roughly 35% of EMR time occurred remotely, with a greater proportion of this time occurring during nighttime hours and on Sundays [21]. Because these estimates come from distinct systems, roles, and measurement approaches, they should not be interpreted as additive; rather, they converge on the pattern that EHR‑related tasks frequently extend into personal time.
Electronic Messaging
Every surgical specialty has experienced growth in outpatient interactions, commonly through electronic messaging [39,41]. While there are positive benefits to electronic messaging, such as the ability to mitigate patient frustrations, concerns, and questions while decreasing costs, over-utilization can also impact burnout. High patient call message volumes are associated with higher rates of provider burnout [24]. Electronic messaging between healthcare providers has also increased. While messaging allows for effective relaying of information, inappropriate messaging unnecessarily burdens providers. In one tertiary academic hospital, roughly 28% of nighttime communication was classified as non-urgent, highlighting the importance of timing and content [40].
Usability
Transitioning to use EHRs or transitioning from a different EHR system can cause struggles for providers [2]. While certain basic principles exist between them, there can also be variability within the same EHR based on the hospital. Despite this, little literature exists to guide EHR transitions, instead relying on the internal training teams when applicable [58]. Additionally, for providers who are required to learn how to operate EHRs for the first time, their efficiency drastically drops. While it does eventually improve, it often does not return to the pre-EHR baseline [37]. One limitation of EHRs also relates to downtime, the period when the system is partially or fully unavailable. These time periods can pose significant risks to patients and hospital operations. While protocols often exist to mitigate this risk, one study showed that the protocols were only executed 27.6% of the time [59]. Providers who are dissatisfied with their EHR are at a higher risk of burnout; however, satisfaction with one’s EHR was found to be protective of burnout, demonstrating the difference that a functional, usable EHR makes [34]. In a large nurse survey linked to hospital outcomes, poor EHR usability was associated with higher intention to leave among nurses and with significantly higher odds of inpatient mortality and 30-day readmission [60].
Burnout Strategies
Surgeons’ workloads are already high between balancing scheduled surgery, clinic patients, consultations, administrative tasks, hospitalized patient visits, and emergent surgeries. Given the already high risk of burnout in the field, combating the issue from every avenue is important [15]. While global changes to EHRs would likely have the most significant contribution to EHR-related burnout rates in surgeons, the changes will take time and likely require years of refinement to ultimately achieve the desired outcome. The design of EMRs would ideally be optimized on a user-centered design with direct input from physicians. By creating a system that enhances usability and patient care, physicians would be more likely to adopt and optimize an EHR [61]. While EHRs do have limitations, they also provide an economic advantage, increased quality of care, and can be a protective factor against burnout when utilized well [31,34,62].
The quality of EHR training can impact usability, which can then be extrapolated to improved burnout rates [63]. Most surgeons likely remember their onboarding training at a new hospital included hospital tours, meeting staff, company policies, going through multiple handbooks, and, at some point, going through the EHR. Surgeons frequently receive suboptimal introductions to their new practice settings; robust onboarding can help mitigate the transition [64]. This extends beyond index training, as one study evaluated 1,010 providers participating in a personalized re-training program designed to improve efficiency and knowledge using EHRs. The results showed a reduction in burnout rates from 32% to 23% [65]. Studies have also shown that daily EHR usage decreases over a period of years, highlighting that physicians also improve their efficiency over time [33].
Speech recognition software allows physicians to create text from voice commands, decreasing documentation time [66]. This technology has continued to become more complex and useful in documentation [23,67]. Artificial intelligence (AI) has the potential to drastically impact documentation by leveraging natural language processing technology to automate documentation of patient visits in EHRs [68]. The benefits of AI, particularly regarding machine learning, are not limited to documentation only. While still in its infancy, rapid processing and analysis of past medical experiences can be an excellent therapeutic aid. Although it is unlikely to fully replace a surgeon’s own onus to perform a chart review, it may develop into an adjunct that decreases EHR-related time.
Medical scribes have been proposed to alleviate stress through decreased provider-EHR time, increased patient and provider satisfaction, improved workflow efficiency, and billing and reimbursement coding optimization [47,69,70]. Systematic reviews and meta-analyses support scribe usage with an improved impact on relative value unit per patient hour as well as satisfaction [71]. While the impact on burnout has some varied data, some studies show reduced burnout and significantly less time charting [72]. One retrospective study examined 148,410 scribed encounters at 55 different clinics and found that surgery had the lowest median completion time, further showing the potential for scribes to improve documentation-related burnout [47]. These findings had a financial impact, as one pediatric plastic surgery clinic at a tertiary care facility found that scribes reduced their cost per office visit [73]. With an improvement in documentation burden, coding, and inter-office communication, scribes may be a useful addition to help mitigate burnout [74]. At the individual level, surgeons can also adopt practical tactics to use the EHR more efficiently and reduce burden. Examples include customizing templates and order sets for common scenarios, using speech recognition or macros for repetitive documentation, batching inbox and portal message review into scheduled blocks, delegating appropriate tasks through team-based messaging protocols, and requesting optimization or retraining sessions when workflows change. These strategies cannot fully offset structural and policy constraints but provide pragmatic steps within current systems.
While some strategies above can help mitigate burnout related to EHRs in the surgical field, the largest and most lasting change would have to be at a policy level. While vendors can mitigate difficulties with current issues, until it is required that EMRs are produced in a user-friendly design, with input from healthcare professionals, have interoperability standards to easily facilitate the exchange of information between systems, and there is a reform to payment policy to include care coordination and accuracy of information provided, there is little incentive for EHRs to adapt to the needs of patients [46]. The requirement of significant changes to the usability of EHR, including reform of certification standards, interoperability, and increasing physician engagement in the design, implementation, and customization, would be an important first step in addressing EHR-related issues.
While EHRs have made a substantial positive contribution to healthcare, they have also been frequently associated with physician burnout in surgical specialties. This review of the literature identified documentation and time demands as the two most frequently reported EHR‑related domains associated with burnout signals. Surgeons are inherently placed under an immense amount of stress at baseline in their careers, and the inherent risk of burnout associated with providing complex surgical care needs to be better addressed. Ultimately, for there to be a substantive impact on burnout rates, changes to EMRs need to happen at a policy level. However, steps can be taken in the interim to attempt to better mitigate burnout. Addressing EHR-related burden is essential to sustaining the surgical workforce and ensuring safe, efficient patient care.
Limitations
This review is limited by a single database (PubMed) search, restriction to U.S.‑based, English‑language studies, and lack of a formal risk‑of‑bias assessment, which may exclude relevant international or non‑English literature and limit comparability across heterogeneous designs and measures. As a narrative (rather than systematic) review, heterogeneity in study designs, burnout measures, and EHR exposure definitions precludes meta‑analysis and formal pooling. Selection and publication bias are possible. Specialty‑specific workflows and local EHR configurations may restrict generalizability across surgical settings. To enhance reproducibility, we provide PRISMA‑S search details and a brief domain codebook; discrepancies in domain coding were resolved by consensus.
Conclusions
This narrative review of 25 studies highlights that EHR-related burnout among surgeons is most frequently reported in association with excessive documentation demands and time burdens, with additional contributions from electronic messaging and usability issues. Although EHRs have improved safety, coordination, and transparency in patient care, they have also introduced significant administrative strain that detracts from efficiency and work-life balance. Addressing this issue will likely require a multifaceted approach, enhancing system usability, optimizing workflow integration, expanding effective onboarding and retraining programs, and supporting the adoption of tools such as speech recognition, AI, and medical scribes. Lasting improvement will probably depend on policy-level reforms that promote user-centered EHR design and interoperability standards. Given the observational and heterogeneous nature of the available evidence, these findings should be interpreted as associations rather than causal effects; future comparative, prospective, and interventional studies will be important to test whether targeting these domains reduces burnout and improves outcomes. Mitigating EHR-related burnout is critical to preserving surgeon well-being, sustaining workforce longevity, and ensuring the delivery of safe, high-quality surgical care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Clinically excellent use of the electronic health record: review JMIR Hum Factors Wolfe L Chisolm MS Bohsali F 05201810.2196/10426 PMC 623188730291099 · doi ↗ · pubmed ↗
- 2Benefits and drawbacks of electronic health record systems Risk Manag Healthc Policy Menachemi N Collum TH 4755420112231222710.2147/RMHP.S 12985 PMC 3270933 · doi ↗ · pubmed ↗
- 3Clinical information technologies and inpatient outcomes: a multiple hospital study Arch Intern Med Amarasingham R Plantinga L Diener-West M Gaskin DJ Powe NR 10811416920091917180510.1001/archinternmed.2008.520 · doi ↗ · pubmed ↗
- 4Effect of computerized physician order entry and a team intervention on prevention of serious medication errors JAMA Bates DW Leape LL Cullen DJ 131113162801998979430810.1001/jama.280.15.1311 · doi ↗ · pubmed ↗
- 5The effect on test ordering of informing physicians of the charges for outpatient diagnostic tests N Engl J Med Tierney WM Miller ME Mc Donald CJ 149915043221990218627410.1056/NEJM 199005243222105 · doi ↗ · pubmed ↗
- 6Electronic alerts to prevent venous thromboembolism among hospitalized patients N Engl J Med Kucher N Koo S Quiroz R Cooper JM Paterno MD Soukonnikov B Goldhaber SZ 96997735220051575800710.1056/NEJ Moa 041533 · doi ↗ · pubmed ↗
- 7Improved influenza and pneumococcal vaccination in rheumatology patients taking immunosuppressants using an electronic health record best practice alert Arthritis Rheum Ledwich LJ Harrington TM Ayoub WT Sartorius JA Newman ED 150515106120091987708810.1002/art.24873 · doi ↗ · pubmed ↗
- 8Physician and medical student burnout, a narrative literature review: challenges, strategies, and a call to action J Clin Med Cotobal Rodeles S Martín Sánchez FJ Martínez-Sellés M 22631420254021771310.3390/jcm 14072263 PMC 11989521 · doi ↗ · pubmed ↗