Salivary Gland Secretory Carcinoma in the Facial Region: A Pediatric Case Presentation
Alexandra Perales, Miguel Flores, Carlos Manresa, Mariana Villarroel-Dorrego

TL;DR
This paper presents a rare case of salivary gland secretory carcinoma in a 12-year-old child, highlighting its unusual occurrence in pediatric patients.
Contribution
The novelty lies in documenting a pediatric case of a tumor typically found in adults, emphasizing the need for awareness in younger populations.
Findings
Salivary gland secretory carcinoma can occur in children, despite being predominantly an adult-onset tumor.
The case presented a slow-growing, painless facial mass that was confirmed as secretory carcinoma via histopathology.
Abstract
Salivary gland secretory carcinoma (SC) represents a rare, slow-growing, low-grade malignant neoplasm that occurs mainly in the parotid gland. It has a slight predilection for the male gender and usually appears in adulthood. The morphologic and immunohistochemical features are like those observed in secretory breast carcinoma; however, it has been described as a distinct salivary gland tumor. Its clinical characteristics remain nonspecific and therefore can be misdiagnosed. This report describes a 12-year-old patient who presented with a slow, progressive, painless, and deforming mass at the level of the left lower third of the face, of eight months' evolution. After clinical and imaging evaluation, an excisional biopsy was performed. The sample was sent for histopathological study, which reported salivary gland SC. Although this condition typically presents in adults, it can occur in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1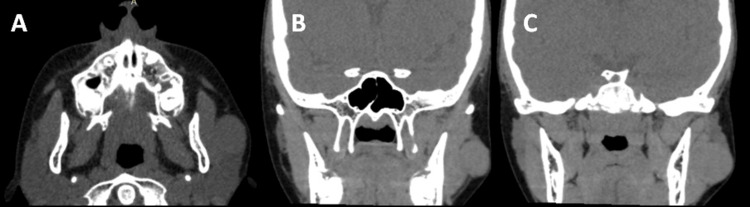 Figure 2
Figure 2 Figure 3
Figure 3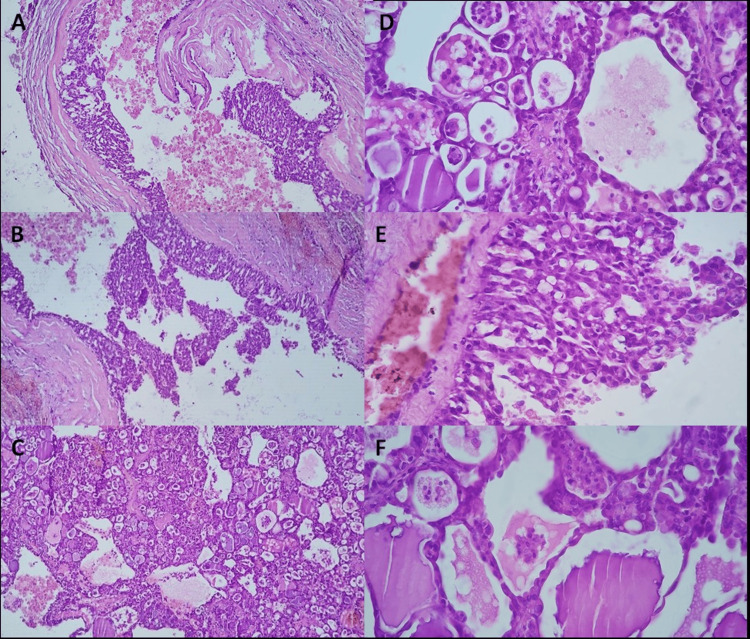 Figure 4
Figure 4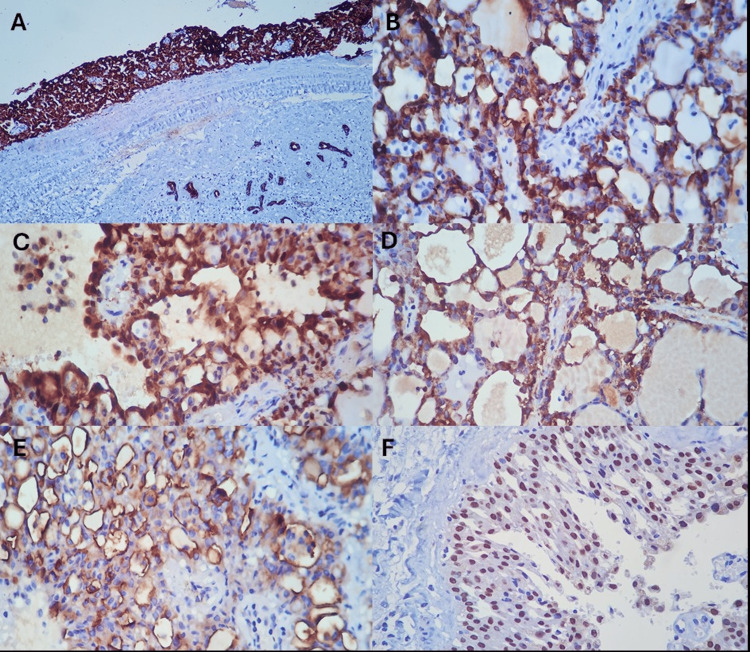 Figure 5
Figure 5| Author, year | Gender/Age (in years) | Location | Histopathology | IHC | Treatment |
| Meng et al., 2023 [ | M, 4 y | Parotid gland | Solid, tubular and papillary growth patterns, eosinophilic secretions within microcystic structures | CK7, S100, and pan-TRK protein. Protein p63 was positive with a peripheral pattern | Excision with free margins |
| Ngouajio et al., 2017 [ | M, 14 y | Parotid gland | Cystic, tubular, and/or papillary architecture | S100, mammaglobin, cytokeratin 19, and vimentin | Left superficial parotidectomy with selective neck dissection |
| Ash et al., 2023 [ | M, 13 y | Parotid gland | Solid, microcystic, macrocystic, papillary-cystic, and tubular patterns | CK7 and S-100 | Excision |
| Rastatter et al. 2012 [ | F, 14 y | Parotid gland | Prominent papillary formations and several microscopic cystic spaces | S100 | Parotidectomy |
| Hwang et al., 2014 [ | F, 13 y | Parotid gland | Microcysts, tubular structures, and solid nests, with focal papillary formation | S100, CK 19, and vimentin | Excisional biopsy with free margins |
| Keisling et al., 2014 [ | F, 5 y | Buccal mucosa | Microcystic spaces, foamy cells, and vacuolated cells | Vimentin, AE1/AE3, CK7. EMA, S100, and mammaglobin | Excisional biopsy |
| Joshi et al., 2015 [ | M, 15 y | Parotid gland | Microcystic with containing vacuoles | S100, CK7, CK19, vimentin, EMA | Parotidectomy |
| Oza et al., 2016 [ | F, 9 y; F, 16 y | Parotid gland | Papillary and microcystic pattern | Mammoglobin and S100 | Parotidectomy |
| Chen et al., 2018 [ | F, 12 y | Parotid gland | Microcystic pattern | CK7, S100, GATA3 | Superficial parotidectomy |
| Shigeta et al., 2018 [ | F, 7 y | Parotid gland | Microcystic structure | S100, mammaglobin, GCDFP15, vimentin, CAM5.2 | Superficial parotidectomy |
| Shukla et al., 2018 [ | M, 17 y | Parotid gland | Solid, cystic, tubular, and papillary architecture with individual cells having abundant eosinophilic granular to vacuolated cytoplasm | CK, EMA, S100 and mammaglobin | Excision of injury with free edges |
| de Melo et al., 2025 [ | F, 9 y | Upper lip | Microcystic nests filled with eosinophilic secretions | CK7, mammaglobin, and S100. PAS positive | Excisional biopsy |
| de Souza Tolentino et al., 2025 [ | F, 14 y | Palate | Tumor cells arranged in a microcyst architecture | - | Excisional biopsy, bilateral tonsillectomy, and adjuvant radiotherapy |
| Serrano-Meneses et al., 2024 [ | M, 11 y | Left cheek | Cystic tumor, well-circumscribed and encapsulated. Intracystic cellular proliferation of monotonous cells with eosinophilic cytoplasm, round nuclei | CK (AE1-3), CK 7, GATA3, and S100. PAS positive | Resection |
| Moreddu et al., 2023 [ | M, 8 y; F, 12 y | Parotid gland | Encapsulated, micro-cystic proliferation of monomorphic tumor cells with abundant eosinophilic cytoplasm | S100 and SOX10 | Complete parotid excision surgery with neck node level II dissection |
| Woo et al., 2014 [ | M, 14 y | Parotid gland | Microcystic, tubular, and solid growth patterns, as well as granular and vacuolated amphophilic cytoplasm | Vimentin, S100 and EGFR | Parotidectomy |
| Inaba et al., 2015 [ | F, 15 y | Parotid gland | Microcystic pattern | S100 and mammaglobin | Parotidectomy |
| Quattlebaum et al., 2015 [ | F, 15 y | Parotid gland | Dominant cyst with intracystic fragments of solid and papillary tan tissue with surrounding atrophic salivary gland tissue | S100 and CK19 | Superficial parotidectomy with facial nerve dissection |
| Salgado et al., 2021 [ | Four cases total: M, 7 y; M, 9 y; F, 14 y (n=2) | 3 cases, parotid gland. 1 case, submandibular gland. | Well-circumscribed lesions composed of mid-size, monotonous cells with eosinophilic and sometimes vacuolated cytoplasm. Duct-like structures and microcysts with colloid-like material | S100, CK7, mammaglobin and GATA3 | Excision of injury with free edges |
| Cardoni et al., 2023 [ | F, 12 y | Maxillary sinus | Low-grade component: Papillary/tubular architecture, with cells with dense chromatin and inconspicuous nucleoli. High-grade component: solid pattern | CK (AE1/AE3), vimentin, CK7, EMA, S100 and SOX10, GATA3 and MUC4 | Four courses of 5-fluorouracil and cisplatin plus oral TRK-inhibitor drug. Surgery for a suspected neoplastic residue in the ethmoid area. Adjuvant proton therapy on surgical bed (61.4 Gy) and on an area including the ipsilateral laterocervical lymph nodes (54.05 Gy). |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSalivary Gland Tumors Diagnosis and Treatment · Cancer and Skin Lesions · Soft tissue tumor case studies
Introduction
Salivary gland secretory carcinoma (SC), previously known as mammary analogue secretory carcinoma, is a rare, low-grade malignant neoplasm of the salivary glands that occurs primarily in the parotid gland, followed by the submandibular gland, minor salivary gland, and accessory parotid gland. Its morphological and immunohistochemical similarities are similar to those observed in secretory breast carcinoma. Its characteristic clinical manifestation is the presence of a slow-growing, painless tumor lesion; however, these features remain nonspecific, and therefore it can be misdiagnosed [1-3]. Before being first described by Skálová et al. in 2010 [4], SC was histologically misdiagnosed as an acinar cell carcinoma. Both entities have similarities, but with different histological characteristics and outcomes. Furthermore, SC is characterized by the ETV6-NTRK3 fusion resulting from a chromosomal translocation [3-5].
SC has a low overall incidence, representing less than 0.3% of all salivary gland tumors. Commonly, they may be present in adulthood with slight male predominance, and there have been few cases reported in pediatric patients [6-10]. SC is an indolent malignant salivary gland neoplasm that rarely metastasizes and therefore has a good prognosis. However, its rarity in childhood makes it a diagnostic challenge. The use of immunohistochemical markers, such as S100, SOX10, and mammaglobin, is very helpful. While the demonstration of ETV6 rearrangement by FISH, RNA sequencing, or PCR would be ideal, it is not possible in all cases [3-5]. We describe an unusual case of SC in the facial region of a pediatric patient to highlight pediatric diagnostic pitfalls and management considerations.
Case presentation
A 12-year-old male patient was referred to the Department of Oral and Maxillofacial Surgery of the Hospital General del Oeste "Dr. José Gregorio Hernández," Caracas, Venezuela, with an extraoral normochromic and normothermic painless mass with slow growth on the left parotid-masseteric region evolving over eight months. It was mobile and soft to palpation (Figure 1). The patient had not received prior treatment for the lesion, and his mother did not provide any relevant medical history.
Extraoral photographs. Nodular, mobile lesion is observed in the left parotid-masseteric region.
Clinically, a nodular, mobile lesion was observed, separated from the muscular planes, soft to palpation, and completely asymptomatic. No adenopathy was found. A facial computed tomography revealed a 2.6 cm well-defined, encapsulated, isodense image, located in the left parotid-masseteric region, underlying subcutaneous tissue and superficial to the masseter muscle (Figure 2).
CT scan showing an isodense image corresponding to the lesion.Isodense image overlying the left parotid gland and masseter muscle and underlying cutaneous tissue, of 2.56 cm in larger diameter, with well-defined margins throughout its extent, corresponding to a tumor lesion. Axial (a) and coronal view (b and c).
The clinical diagnoses proposed were dermoid cyst and pleomorphic adenoma, given the benign clinical characteristics of the lesion. Under intravenous conscious sedation, an excisional biopsy of the lesion was performed, preserving the facial nerve (Figure 3). After antiseptic and asepsis measures, markings were made for the preauricular approach. Local anesthetic (lidocaine 2% and epinephrine 1:100,000) was infiltrated, then an incision was made with a number 15 scalpel in the cutaneous and subcutaneous plane, and a blunt dissection was made until the lesion was located and excised. Hemostasis was controlled, and tissue synthesis was carried out layer by layer, completing the surgical act without complications.
Excisional biopsy of the lesion.Preauricular surgical approach preserving nerve. Note the dark color of the tumor.
A violet-colored, well-defined specimen was studied. Microscopic evaluation showed a well-circumscribed but not encapsulated glandular neoplasm. The tumor was composed of microcystic structures with distinctive luminal material (Figure 4). Completed excision with free margins was observed.
Histopathology sections with H&E stainingNeoplasm showed a well-circumscribed, non-encapsulated, glandular neoplasm, with a macro and microcystic structures (4X H&E) (a-c). The lumen is outlined by rounded cells with round vesicular nuclei, fine granular chromatin, and prominent nucleoli. No perineural or vascular invasion was observed (10X H&E) (d-f).H&E: hematoxylin and eosin
An immunohistochemistry study was performed, showing positivity for CK-7, S-100, mammaglobin, MUC 4, and SOX10 (Figure 5), confirming the diagnosis of SC. Molecular conformation of ETV6 or RET rearrangement was not carried out.
Immunohistochemistry staining. Expression of CK-7 (a,b), S-100 (c), mammaglobin (d), MUC4 (e), and SOX10 (f).
The patient was referred to the pediatric oncology department, and after a clinical and paraclinical evaluation, the absence of disease was found. Additional therapy was not indicated; however, strict outpatient check-ups were established. Around 20 months of clinical follow-up have shown no evidence of neoplasia, and the sensory and motor function of the area remains intact.
Discussion
SC represents a rare tumor of salivary glands in children. It was initially described by Skálová et al. in a case series of 16 salivary gland tumors that exhibited histomorphological and immunohistochemical characteristics remarkably similar to mammary secretory carcinoma [5].
SC usually presents as a low-grade, malignant lesion with a low rate of regional lymph node metastases and a low mortality rate. It has often been misdiagnosed as acinic cell carcinoma; therefore, it represents one of the main differential diagnoses, along with mucoepidermoid carcinoma and adenocarcinoma. However, the immunohistochemical and molecular profile of SC makes it possible to differentiate it from other salivary gland tumors [11-13].
The most notable characteristic in the present case is the patient's age, which does not coincide with the average age reported for this neoplasm, which is typically the fourth and fifth decades of life [9-14]. Though SC can occur in children, it is relatively rare. Cases reported in children and adolescents are summarized in Table 1.
Regarding the clinical presentation, studies agree that this is a painless, slow-growing, deforming tumor that can cause facial asymmetry. Occasional bleeding and ulceration of the adjacent mucosa have also been reported [11-12]. In terms of location, this entity has a predilection for major salivary glands, particularly the parotid gland [1], coinciding with the present case, where the lesion was encapsulated lateral to the superficial lobe of the left parotid gland and masseteric muscle.
Concerning the histopathological characteristics, almost all SC cases had typical microcystic architecture, bland tumor cells with eosinophilic to vacuolated cytoplasm, and abundant hypereosinophilic luminal secretion [13-14]. Other patterns include tubular, follicular, and papillary-cystic structures, and a few cases may show a macrocystic morphology. The tumour cells have low-grade vesicular round to oval nuclei with finely granular chromatin and distinctive, centrally located nucleoli. The pale pink cytoplasm is granular to vacuolated. Cellular atypia is usually mild, and mitoses are rare. High-grade transformation is uncommon. Very rare cases of high-grade show solid growth, tumor necrosis, and multiple mitotic figures. Immunohistochemical panel of S-100, mammaglobin, and DOG1 distinguishes SC from acinic cell carcinoma [13]. SC shows a diffuse and strong expression of pancytokeratins (AE1-AE3 and CAM 5.2), CK7, CK8, CK18, CK19, epithelial membrane antigen, S-100 protein, MUC4, SOX10 and mammaglobin [13-14].
Management of SC is based on oncological surgical resection. Lymphadenectomies, radiation, and chemotherapy its reserved for cases with regional involvement, histological risk factors (positive margins, perineural invasion), or metastatic disease. Yet, there is still no clear management established for the treatment of SC, due to the low numbers of cases and lack of evidence. Most SC cases involve low-grade malignant neoplasms with effective surgical management, which agrees with the patient reported in this work. Still, there are reports of high-grade, more aggressive cases with higher rates of recurrence [32]. Boon et al. [5] reported 31 patients with SC who underwent tumor resection. Only one patient developed a local recurrence, but no regional recurrences or distant metastases were observed. Furthermore, they found that overall survival at 5 and 10 years was 95% and disease-free survival was 89%.
Conclusions
SC is an infrequent malignant neoplasm of the salivary glands that does not commonly affect children. Although rare, it can occur and mimic benign lesions due to its behavior and clinical characteristics. There are few reports of SC in the pediatric age, but many agree that the clinical course is indolent, which can lead to misdiagnosis. Clinicians should be aware of this possibility and include this diagnosis when encountering a pediatric patient. It should be noted that this is a case report of one patient, and it was not possible to perform genetic fusion testing, which is ideal for the diagnosis of SC.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Histopathology of the Salivary Glands Berlin: Springer Hellquist H Skalova A Berlin Springer 2014
- 2Salivary gland secretory carcinoma: clinicopathologic and genetic characteristics of 215 cases and proposal for a grading system Am J Surg Pathol BaněčkováM Thompson LD Hyrcza MD 6616774720233707073910.1097/PAS.0000000000002043 · doi ↗ · pubmed ↗
- 3Parotid mammary analogue secretory carcinoma: A case report and review of literature World J Clin Cases Min FH Li J Tao BQ 40524062920213414176610.12998/wjcc.v 9.i 16.4052 PMC 8180236 · doi ↗ · pubmed ↗
- 4Mammary analogue secretory carcinoma of salivary glands, containing the ETV 6-NTRK 3 fusion gene: a hitherto undescribed salivary gland tumor entity Am J Surg Pathol SkálováA Vanecek T Sima R 5996083420102041081010.1097/PAS.0b 013e 3181 d 9efcc · doi ↗ · pubmed ↗
- 5Clinicopathological characteristics and outcome of 31 patients with ETV 6-NTRK 3 fusion gene confirmed (mammary analogue) secretory carcinoma of salivary glands Oral Oncol Boon E Valstar MH van der Graaf WT 29338220182990989810.1016/j.oraloncology.2018.04.022 · doi ↗ · pubmed ↗
- 6Secretory carcinoma of the salivary gland (mammary analogue secretory carcinoma) in children [article in Russian]Arkh Patol Sidorov IV Kletskaya IS Konovalov DM 43518220203230743810.17116/patol 20208202143 · doi ↗ · pubmed ↗
- 7Secretory carcinoma of the salivary gland: a rarity in children J Pediatr Hematol Oncol Kelly GA Venkatramani R Quintanilla NM Chelius DC Roy A Mahajan P 1671724420223448654310.1097/MPH.0000000000002304 · doi ↗ · pubmed ↗
- 8A parotid gland mammary analogue secretory carcinoma in a 4-year-old boy: case report and literature review Fetal Pediatr Pathol Meng Z Si W Xiuli Z Liu Y 3423504220233605308210.1080/15513815.2022.2116621 · doi ↗ · pubmed ↗