From Nerves to Nodules: A Case-Based Review of the Progression of Pure Neuritic Leprosy to Lepromatous Leprosy With Erythema Nodosum Leprosum
Shini Choubey, Hemanta K Kar, Debasmita Behera

TL;DR
This paper presents a rare case where pure neuritic leprosy progressed to lepromatous leprosy with a skin reaction, highlighting the importance of monitoring patients even after treatment.
Contribution
The paper reports a rare transformation of pure neuritic leprosy to lepromatous leprosy with ENL, only the second such case documented in the literature.
Findings
A patient with pure neuritic leprosy progressed to lepromatous leprosy with erythema nodosum leprosum after treatment completion.
The transformation may be linked to persistent bacilli and reduced cell-mediated immunity.
Treatment with rifampicin, minocycline, moxifloxacin, thalidomide, and corticosteroids led to significant improvement.
Abstract
Leprosy, caused by Mycobacterium leprae, affects the skin and peripheral nerves. Pure neuritic leprosy (PNL) is a rare subtype, characterized by nerve involvement without skin lesions. We report a rare case of PNL progressing to lepromatous leprosy (LL) with erythema nodosum leprosum (ENL), with only one such case previously reported in the literature and reviewed herein. A 35-year-old male diagnosed with PNL on sural nerve biopsy showing acid-fast bacilli (3+) completed multidrug therapy for 12 months. Nine months later, he developed painful erythematous nodules and sensory-motor deficits. Slit-skin smear (bacteriological index 4+) and biopsy confirmed LL with ENL. He was treated with monthly pulses of rifampicin, minocycline, and moxifloxacin, along with thalidomide and corticosteroids. Significant improvement occurred after six months. This case illustrates the intricate clinical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
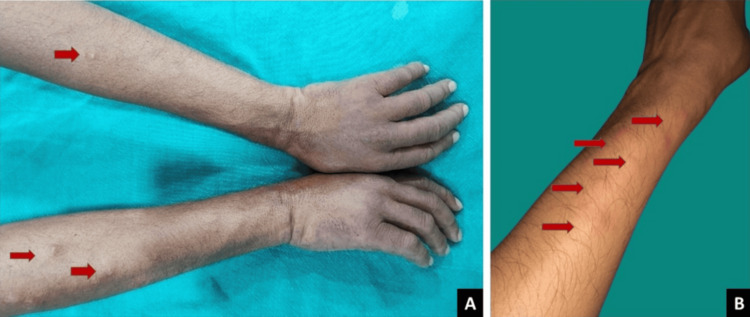 Figure 1
Figure 1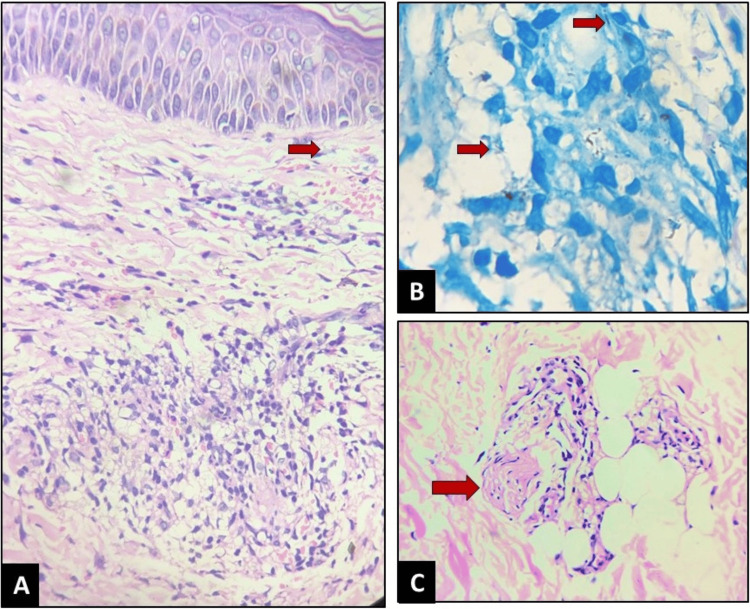 Figure 2
Figure 2 Figure 3
Figure 3| Case | Age | Gender | Duration after which the reaction occurred | Slit-skin smear | Lab investigations | Management | |
| PNL | T2R | ||||||
| Fernandes et al. (2020) [ | 30 | Male | Two months after diagnosis and initiation of MDT | Negative | Presence of | Skin biopsy sample for histopathology; BI: negative | PNL: MB-MDT with prednisolone; T2R: thalidomide and steroids; MDT continued |
| This case | 35 | Male | Nine months after diagnosis of PNL and initiation of MDT | Baseline: negative; T2R: 4+ | Presence of lepra bacilli in sural nerve biopsy: BI: 3+; nerve conduction study | Skin biopsy sample for histopathology: BI: 1+ | PNL: MB-MDT prednisolone; T2R: thalidomide and steroids; rifampicin 600 mg, minocycline 200 mg, and moxifloxacin 400 mg (RMM monthly once pulse for 12 months) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLeprosy Research and Treatment · Infectious Diseases and Tuberculosis · Phenothiazines and Benzothiazines Synthesis and Activities
Introduction
Leprosy, a chronic infectious disease caused by Mycobacterium leprae, manifests across a clinical spectrum, with nerve involvement being a hallmark. Pure neuritic leprosy (PNL) is a rare subtype, particularly seen in the Indian subcontinent (2.17-5.3%), characterized by isolated peripheral nerve damage without skin lesions, often delaying diagnosis and treatment [1]. PNL may gradually involve multiple nerves and affect the surrounding skin supplied by the involved nerves, a phenomenon known as secondary neuritic leprosy. This typically occurs in the borderline spectrum of the disease (BT to BB, rarely BL) when the body’s cell-mediated immunity (CMI) gradually deteriorates due to delayed initiation of anti-leprosy treatment. In PNL, neuritis more commonly manifests as Type 1 reactions (T1Rs) and only rarely as Type 2 reactions (T2Rs) [2]. In this report, we present a rare case of PNL that unexpectedly progressed to lepromatous leprosy (LL), the most severe and disseminated form of leprosy, complicated by erythema nodosum leprosum (ENL), or T2R [3].
ENL lesions are manifestations of T2R, a multisystem, immune-mediated complication of LL and, rarely, BL leprosy. T2R is characterized by the sudden development of tender skin lesions (ENL), neuritis, arthritis, dactylitis, orchitis, lymphadenitis, osteitis, ocular complications, and nephritis, with or without fever or malaise, and histological features consistent with ENL on tissue biopsy. ENL can be the initial manifestation of the disease or occur during the course of treatment. It is considered a neutrophilic, immune complex-mediated reaction, with evidence of complement, protein, and immunoglobulin deposition in the dermis and other tissues.
This article was previously presented as a poster and meeting abstract at the 105th British Association of Dermatologists’ Annual Meeting in Glasgow on June 1, 2025.
Case presentation
History and examination
A 35-year-old male from a leprosy-endemic region of India presented with progressive weakness and loss of sensation in both hands and feet over the past eight months. He was diagnosed with PNL in August 2022, confirmed by sural nerve biopsy, which showed acid-fast bacilli (AFB; 3+) and granulomatous inflammation, along with the presence of *M. leprae *within macrophages. Based on this diagnosis, he was started on WHO-recommended multidrug therapy (MDT) with rifampicin, dapsone, and clofazimine for 12 months.
During MDT, the patient experienced improvement in neurological symptoms, including sensory loss and motor deficits. The bacteriological index (BI) on skin smear examination also improved, correlating well with the clinical recovery. However, nine months after completing MDT, he developed numerous painful erythematous nodules on his face, trunk, and extremities, accompanied by systemic symptoms including fever, malaise, and joint pain (Figure 1A, 1B).
Baseline images(A) Multiple erythematous nodules (red arrows), 0.5-1.5 cm in diameter, present over the extensor aspects of both forearms, along with edema of the dorsum of the hands. (B) Zoomed-in view of erythematous nodules, clinically suggestive of ENL.ENL, erythema nodosum leprosum
These lesions were associated with progressive numbness, muscle weakness, and sensory deficits in both hands and feet. There was complete loss of sensation in the distribution of the ulnar, median, and lateral popliteal nerves. Examination revealed enlargement and tenderness of the left ulnar nerve with neuritis, partial ulnar claw hand, and atrophy of the small muscles of the left hand.
Investigations
Slit-skin smear examination was performed from the bilateral earlobes, bilateral eyebrows, left buttock, and nodule, following the standard WHO protocol using Ziehl-Neelsen staining for AFB. This revealed a positive BI of 4+ [1].
Histopathological examination of the skin revealed positive AFB and showed reticular dermal infiltration of lymphocytes, flattening of the rete ridges, and a prominent Grenz zone. The dermis demonstrated inflammatory cell infiltration with foamy macrophages, consistent with a diagnosis of LL with ENL (Figure 2A-2C).
Histopathology images(A) H&E stain, 10×: reticular dermal infiltration of lymphocytes, flattening of the rete ridges, and a prominent Grenz zone (red arrow). The dermis shows inflammatory cell infiltration with foamy macrophages. (B) Lepra stain, 40×: presence of AFB (red arrows) with a BI of 1+. (C) H&E stain, 40×: granular polymorphonuclear infiltration with perineural lymphocytic infiltration and lobar panniculitis (nerve fiber indicated by red arrow).AFB, acid-fast bacilli; BI, bacteriological index
Management
Three bactericidal drugs were administered in a monthly pulse regimen for 12 months due to the suspected presence of drug-resistant M. leprae: rifampicin 600 mg, minocycline 200 mg, and moxifloxacin 400 mg, each given as a once-monthly pulse. For management of ENL, thalidomide was initiated at 300 mg daily for seven days, followed by 200 mg daily for the next month, and then 100 mg daily for the subsequent three months to control the severe ENL reaction. Additionally, oral prednisolone (1 mg/kg body weight) was administered for the initial 12 weeks, with a tapering dose, to treat left ulnar neuritis.
At the six-month follow-up, the patient responded favorably to treatment, with no new ENL lesions or neuritis (Figure 3). Peripheral sensation and mobility of the partial claw hand improved with standard physiotherapy and the use of a claw-hand splint. The patient has been followed for 12 months with no recurrence.
Follow-up imageComplete improvement was observed at six months of follow-up, with no evidence of reaction, erythema, edema, or new lesions following monthly pulse therapy with rifampicin (600 mg), minocycline (200 mg), and moxifloxacin (400 mg).
Discussion
This case illustrates the clinical challenges associated with leprosy, particularly how PNL can progress to more severe forms, such as LL. The onset of ENL further complicates management, necessitating careful treatment strategies. While T1Rs are commonly documented in PNL, only a single instance of a T2R has been previously reported in PNL (Table 1) [4].
Differential diagnosis of PNL is essential due to overlapping symptoms with various neurological conditions. Clinicians must consider several potential alternatives, including Guillain-Barré syndrome, which presents with rapid-onset muscle weakness and sensory alterations. Diabetic neuropathy, characterized by sensory loss and pain primarily in the extremities, is another important consideration [5]. Multiple sclerosis may also mimic PNL, as it can cause diverse neurological symptoms, including motor deficits. Additionally, conditions such as chronic inflammatory demyelinating polyneuropathy, sarcoidosis, and HIV-associated neuropathy can exhibit similar presentations. Infectious causes like vitamin B12 deficiency and Lyme disease may also lead to peripheral neuropathy. Hereditary neuropathies, such as Charcot-Marie-Tooth disease, should be evaluated. Each of these conditions requires thorough clinical assessment and specific diagnostic tests to ensure accurate differentiation, highlighting the importance of an interdisciplinary approach in managing patients suspected of having PNL [6].
Recently, there has been a rise in atypical presentations of leprosy, including the development of skin lesions after peripheral nerve involvement, commonly observed in the borderline spectrum [7]. Drug resistance may contribute to changes in disease spectrum from PNL to LL; however, due to the patient’s economic constraints, a resistance study was not performed.
We hypothesize that drug-resistant M. leprae bacilli and/or persisters in the peripheral nerves, even after a complete course of MDT, play a significant role in reactivation or relapse of leprosy by spreading from the nerves to the skin, leading to downgrading toward LL following reduced CMI [8]. ENL usually develops due to rapid bacterial killing following MDT, either during or after treatment, and rarely before treatment. Persisters typically cause relapse after MDT completion due to their multiplication and may also trigger T2Rs. The exact mechanism remains unclear, though reduced CMI likely plays a key role [9]. All such cases require urgent drug-sensitivity testing and immunological evaluation. Lepromin testing could not be performed in this case due to its unavailability in India, preventing assessment of CMI status.
Conclusions
While T1Rs, with or without skin lesions, are known to occur in PNL, cases with a high bacillary load and low CMI may show downgrading toward the lepromatous spectrum and develop T2Rs, which is a rare phenomenon. This case emphasizes the importance of early diagnosis of all PNL cases, vigilant follow-up, and awareness of potential disease transformations, particularly in endemic areas.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Epidemiology of peripheral neuropathy: an Indian perspective Ann Indian Acad Neurol Trivedi S Pandit A Ganguly G Das SK 1731842020172890444510.4103/aian.AIAN_470_16PMC 5586108 · doi ↗ · pubmed ↗
- 2Leprosy reactions and neuropathic pain in pure neural leprosy in a reference center in Rio de Janeiro - Brazil Front Med (Lausanne) Pitta IJ Hacker MA Vital RT 865485920223540242810.3389/fmed.2022.865485 PMC 8992651 · doi ↗ · pubmed ↗
- 3P 030 from nerve to nodules: the unexpected progression of pure neuritic leprosy to lepromatous leprosy with erythema nodosum leprosum Br J Dermatol Choubey S Hemanta K 1932025
- 4Pure neuritic leprosy with type 2 reaction Indian J Lepr Fernandes E Pai VV Shukla P Gupta T Nandeesh BN 5761922020 http://www.ijl.org.in/published-articles/14092021175726/08_E_Fernandes_57-61_%281%29.pdf
- 5Pure neuritic leprosy: latest advancements and diagnostic modalities: diagnosis of pure neuritic leprosy Diagn Microbiol Infect Dis Razdan N VB Sadhu S 11652911020243927813610.1016/j.diagmicrobio.2024.116529 · doi ↗ · pubmed ↗
- 6Mandating nerve biopsy: a step towards personalizing therapy in pure neuritic leprosy J Peripher Nerv Syst Kulshreshtha D Malhotra KP Malhotra HS Thacker AK Garg RK Singh AK Maurya PK 1901962320183007000710.1111/jns.12283 · doi ↗ · pubmed ↗
- 7Pure neuritic leprosy: current status and relevance Indian J Dermatol Venereol Leprol Rao PN Suneetha S 2522618220162708892610.4103/0378-6323.179086 · doi ↗ · pubmed ↗
- 8Rare occurrence of lepra type 1 reaction in pure neuritic leprosy: a case report Clin Case Rep Pathak R Agrawal S Paudyal P 09202110.1002/ccr 3.4324 PMC 822389234194806 · doi ↗ · pubmed ↗