Incidence of Cytomegalovirus (CMV) Infection in After Kidney Transplant Patients: A Systematic Review and Meta‐Analysis
Gleice K. Jesus, Róger Costa, Gabriel O. Franco, Cleyde C. S. Marconi, Maria B. Arriaga, Eduardo M. Netto

TL;DR
This study finds that nearly half of kidney transplant patients develop CMV infection, highlighting key risk factors and the need for targeted monitoring.
Contribution
A systematic review and meta-analysis quantifies CMV incidence and identifies risk factors in kidney transplant recipients.
Findings
The pooled incidence of CMV infection in kidney transplant recipients is 42%.
Key risk factors include donor-recipient serodiscordance, advanced age, and post-transplant lymphopenia.
High heterogeneity among studies suggests variability in CMV incidence across populations.
Abstract
Kidney transplantation is recognised by the World Health Organisation as the most effective therapy for end‐stage renal disease, offering substantial improvements in survival and quality of life. However, the immunosuppression required to prevent graft rejection predisposes recipients to opportunistic infections, among which cytomegalovirus (CMV) remains a leading cause of morbidity and mortality. To determine the incidence of CMV infection in kidney transplant recipients and identify clinical and laboratory predictors and associated risk factors. A systematic review and meta‐analysis, registered in PROSPERO (CRD42024524165), was conducted in accordance with PRISMA guidelines. PubMed, Web of Science, and LILACS databases were searched up to 6 March 2024 for cohort studies reporting CMV incidence post‐kidney transplantation. Methodological quality was assessed using the Newcastle–Ottawa…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
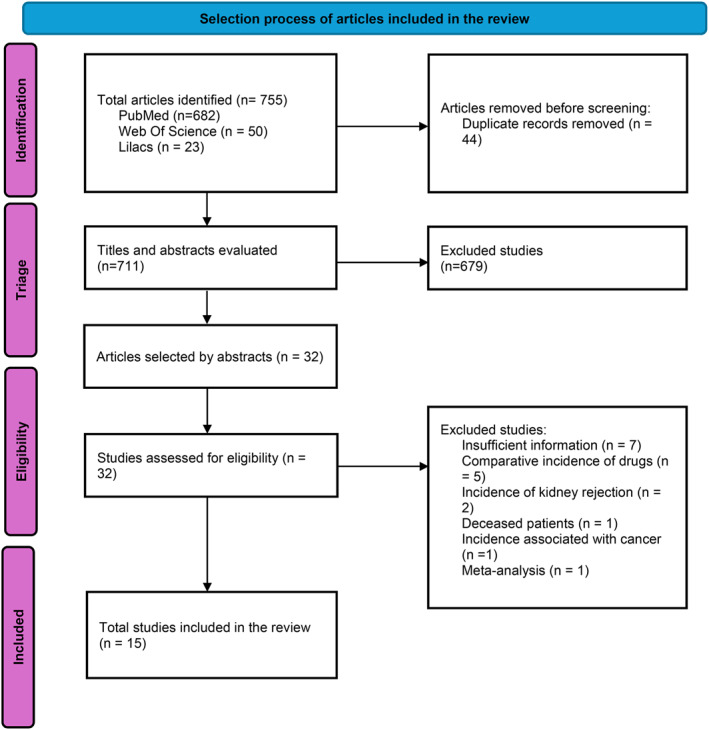 FIGURE 1
FIGURE 1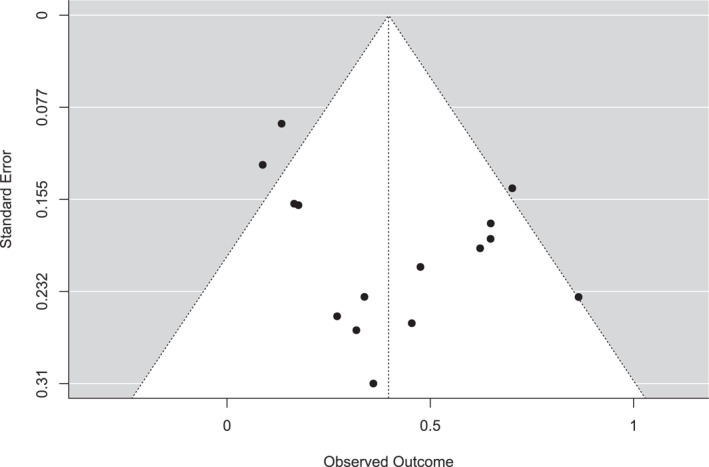 FIGURE 2
FIGURE 2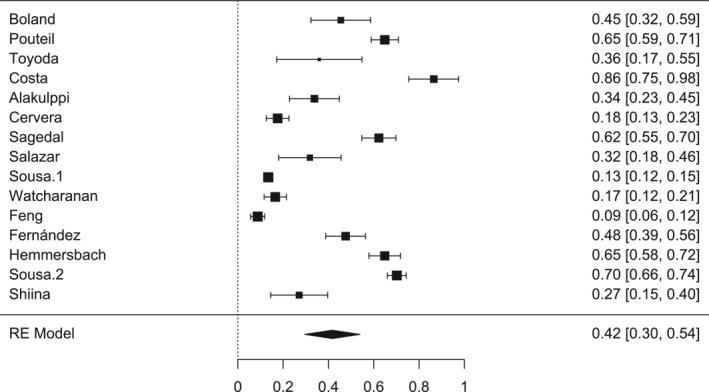 FIGURE 3
FIGURE 3| Author | Selection (max. 4) | Comparability (max. 2) | Exposure (max. 3) | Total | |||||
|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 1 | 1 | 2 | 3 | ||
| Boland (1990) [ | * | * | * | * | ** | * | * | — | 8/9 |
| Pouteil (1992) [ | * | * | * | * | ** | * | — | * | 8/9 |
| Toyoda (1997) [ | * | * | * | ** | * | * | 7/9 | ||
| Costa (1999) [ | * | * | * | * | * | * | * | * | 8/9 |
| Alakulppi (2006) [ | * | * | * | ** | * | * | 7/9 | ||
| Cervera (2007) [ | * | * | * | * | ** | * | * | 8/9 | |
| Sagedal (2008) [ | * | * | * | * | ** | * | * | * | 9/9 |
| Salazar (2009) [ | * | * | * | ** | * | * | 7/9 | ||
| Sousa (2010) [ | * | * | * | ** | * | * | 7/9 | ||
| Watcharanan (2012) [ | * | * | * | ** | * | * | * | 8/9 | |
| Feng (2016) [ | * | * | * | ** | * | * | 7/9 | ||
| Fernández (2019) [ | * | * | * | ** | * | * | 7/9 | ||
| Hemmersbach (2019) [ | * | * | * | ** | * | * | 7/9 | ||
| Sousa (2021) [ | * | * | * | * | ** | * | * | * | 9/9 |
| Shiina (2023) [ | * | * | ** | * | * | 6/9 | |||
| Author | Country | Type of study | Population |
|
| Middle ages | Follow‐up time (months) | Incidence | Diagnosis | Risk factors |
|---|---|---|---|---|---|---|---|---|---|---|
| Boland [ | Netherlands | Cohort | Adults | 55 | 25 | NR | 1–6 | 0.45 | Antigenemia. | Positive IgM |
| Thumb [ | France | Cohort | Adults | 242 | 157 | NR | 1–3 | 0.65 | Antigenemia, culture and serology | Viraemia associated with severe infection |
| Toyoda [ | United States | Cohort | Adults | 25 | 9 | NR | 1–12 | 0.36 | Serology, elisa | High levels of AECA and IL‐2 |
| Coast [ | Brazil | Cohort | 37 | 32 | NR | 1–4 | 0.86 | PCR, elisa | NR | |
| Alakulppi [ | Finland | Cohort | Adults | 71 | 24 | 47 | 1–12 | 0.34 | Genotyping, PCR | IL10 genotype |
| Cervera [ | Spain | Cohort | Adults | 222 | 39 | 50 | NO | 0.18 | Genotyping, PCR | Low MBL production genotypes and TLR4 mutation |
| Sagedal [ | Norway | Cohort | Adults | 159 | 99 | 47 | 1–3 | 0.62 | PCR, MBL and MASP‐2 immunological assays | Low MASP‐2 levels |
| Salazar [ | Chile | Cohort | Children | 44 | 14 | 5.5 | 1–6 | 0.32 | Indirect immunofluorescence | Previous seronegativity, younger age |
| Sousa [ | Brazil | Cohort | Adults | 1676 | 225 | 41.4 | 1–12 | 0.13 | PCR and antigenemia | Ischaemia time |
| Watcharananan [ | Thailand | Cohort | Adults | 218 | 36 | 43.3 | 3–6 | 0.17 | PCR | Higher viral load, acute rejection |
| Feng [ | China | Cohort | Adults | 319 | 28 | 45 | 1–4 | 0.09 | CMV‐QNAT, elisa, antigenemia | History of rejection, negative expression of anti‐CMV IgG |
| Fernández‐Ruiz [ | Spain | Cohort | Adults | 124 | 59 | 59.8 | 12 | 0.48 | Cellular immunity monitoring | Low CD8+ count |
| Hemmersbach‐Miller [ | United States | Cohort | Elderly | 182 | 118 | 57.5 | 12 | 0.65 | Antigenemia | Advancing age and genitourinary conditions |
| Sousa [ | Brazil | Cohort | Adults | 466 | 327 | 52 | 24 | 0.70 | PCR | Previous seronegativity, absence of prophylaxis |
| Shiina [ | Japan | Cohort | Adults | 48 | 13 | 47 | 12 | 0.27 | Absolute lymphocyte count | Low lymphocytes count on day 28 post‐day |
| Study | Preditor | Incidence | Observations |
|---|---|---|---|
| Boland [ | pp65 antigenemia | HIV‐positive with active infection: 74% | Antigenemia precedes IgG/culture; useful for pre‐emptive intervention |
| Serodiscordance D+/R− | Primary infection: 36% | Highest risk group for primary CMV | |
| Pouteil‐Noble [ | Positive IgM/viruria | 65% | Association with moderate/severe forms (OR ≈ 3.28) |
| Toyoda [ | Elevated post‐CMC‐DNA AEC | NR | Elevated AECA 1–4 weeks after CMV‐DNA; they are maintained for months; possible vascular rejection |
| Coast [ | qPCR (blood/urine) | Active infection (any method): 86.4%; urine CRP: 64.9% | PCR detects before serology; some PCR‐positive cases only |
| Alakulppi [ | Donor IL‐10 genotype (−1082 AA vs. AG/GG) | 15% (AA) and 41% (AG/GG) | Associated polymorphism; scenario D+/R−; prophylaxis varied among patients |
| Cervera [ | TLR4 polymorphism | 58.4% | Presence of the mutation increases the risk of primary CMV |
| Sagedal [ | MASP‐2 low (≤ 148 μg/L) | CMV disease at 12 weeks: 22%; overall infection: 59.8% | No prophylaxis; biweekly PP65 tracking |
| Salazar [ | Paediatric (< 5 years) | Up to 6 months: 45%; condition: 11% | Greater precocity of events in paediatrics |
| Watcharananan [ | Prior acute rejection/high viral load (qPCR) | 4.6% | Approximate cut‐off point: 1.7 × 10^4 copies/mL versus. < 7.2 × 10^3 |
| Feng [ | Leucopenia and high viral load | 8.8% | Leucopenia favours viral infections |
| Anti‐CMV IgG positive | 9%–12% | Combined with other factors | |
| Advanced age (≥ 65 years) | 60.7% | Increased vulnerability | |
| Post‐transplant lymphopenia | 44% | Patient with lymphopenia on the 28th day developed CMV within 1 year | |
| Pre‐transplanted MIC deficiency | 71% | 39% when CD8+ ≥ 1 cél/mL | |
| Fernández‐Ruiz [ | Absent/weak CMI (specific T‐response) | At 12m: 47.6% (viraemia 39.5%) | Reduced cellular response in the pre/post‐immediate predicts events |
| Sousa—2 [ | Diabetes mellitus | 73.7% | Associated with other infections, mainly by multidrug‐resistant microorganisms. |
| Shiina [ | ALC‐D28 < 1.100/μL | 27% (stratified by LAC: NR) | HR 3.32 for low LAC; VPN 83% to the cutoff point |
| Study | Risk factors | Prevention or monitoring strategy |
|---|---|---|
| Boland [ | Serodiscordance D+/R−: Primary infection 36%; active 74% (seropositive) | Early surveillance with antigenemia; preemptive intervention when positive |
| Pouteil‐Noble [ | Positive IgM: High severity (OR ≈ 3.28) | Combine IgM + viruria/viraemia to stratify severity and anticipate therapy |
| Toyoda [ | Elevated AECA: Suggests associated vascular risk/rejection | Monitor signs of endothelial injury; consider impact on surveillance and rejection |
| Coast [ | Early detection by qPCR: Identifies initial subclinical infection | Implement serial qPCR as the basis of pre‐emptive protocol |
| Alakulppi [ | Donor IL‐10 genotype (−1082 AA vs. AG/GG) | Consider genotyping as risk refinement |
| Cervera [ |
Induction with ATG; D+/R− risk: Increased risk with lymphodepletion | Prophylaxis with ganciclovir; PP65‐guided preemptive; |
| Sagedal [ | Low MASP‐2/MBL | Intensified surveillance without prophylaxis |
| Salazar [ | Paediatric range | Intensive monitoring in the first months; lower thresholds for intervention |
| Sousa—1 [ |
Early infectious complications: CMV as one of the main infections | Apply systematic laboratory screening protocols |
| Watcharanan [ | Previous acute rejection; high viral load by qPCR: Association with symptomatic CMV | Use viral load cut‐off points to initiate pre‐emptive therapy; heightened post‐rejection surveillance |
| Feng [ | D+/R−; IgG negative pre‐transplant; leucopenia/high viral load: high risk in subgroups | Stratify by serology; reinforce prophylaxis and serial qPCR at high risk |
| Fernández‐Ruiz [ | Reduced IMR: Higher incidence of events at 12 months | Monitor CMI in the pre‐ and post‐immediate; modular qPCR frequency/prophylaxis |
| Hemmersbach‐Miller [ |
Elderly (≥ 65 years old) Elevated risk of infections in year 1 | Enhanced surveillance protocols; integration with qPCR and clinical assessment |
| Sousa—2 [ | DECD: CMV as the most common infection; independent association with MDR | Intensified surveillance and antimicrobial stewardship; attention to MDR |
| Shiina [ |
ALC‐D28 < 1.100/μL HR 3.32; VPN 83% for cutoff point | Use ALC‐D28 as screening for monitoring density in the 1st year |
- —Brazilian National Research Council
- —Coordination for the Improvement of Higher Education Personnel scholarship
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCytomegalovirus and herpesvirus research · Renal Transplantation Outcomes and Treatments · Transplantation: Methods and Outcomes
Introduction
1
Kidney transplantation is recognised by the World Health Organisation (WHO) as the most effective therapeutic option for patients with end‐stage renal disease, significantly improving quality of life and increasing survival rates to 83% compared with dialysis [1]. Despite these benefits, the immunosuppression required to prevent graft rejection markedly increases susceptibility to opportunistic infections, affecting up to 57.1% of recipients within 6 months post‐transplant. Among these, cytomegalovirus (CMV) infection is a leading cause of morbidity and mortality, with an overall incidence of 8.8% between the third and sixth months after transplantation [2] and a ninefold higher risk of graft rejection (odds ratio [OR] = 8.9; 95% CI: 2.8–28.1; p = 0.001) [3]. Incidence rates vary between populations: 52% in children [4], 60.7% in older adults [5], and up to 75% in donor–recipient serodiscordance (D+/R−) cases [6], the latter representing one of the main risk factors for primary infection and symptomatic disease.
Over 3 decades, the incorporation of sensitive laboratory methods has changed the way CMV is detected after kidney transplantation. The diagnosis of infection can be carried out by serological methods (IgG, IgM), pp65 antigenemia assays, viral culture, or molecular techniques [7]. Quantitative polymerase chain reaction (qPCR) is particularly valuable for early detection of viral replication [4], enabling timely therapeutic interventions and reducing progression to symptomatic disease [8]. It offers superior sensitivity and specificity compared with pp65 antigenemia [1, 2, 5], particularly in leukopenic patients [4, 7].
Cytomegalovirus (CMV) infection is one of the most significant infectious complications in the post‐kidney transplant period, associated with high morbidity and mortality rates and an increased risk of graft rejection. Previous studies indicate incidences ranging from 8.8% to over 70%, with significant variations according to sociological, clinical, and laboratory factors. This variability makes it difficult to define accurate and universal estimates, in addition to limiting the implementation of prevention and monitoring protocols that are appropriate for all clinical contexts.
Unlike syntheses focused on immunosuppressive regimens, this review anchors the incidence of CMV in laboratory markers, emphasising comparable early detection and risk stratification across centres.
This, the present systematic review and meta‐analysis aims to estimate the incidence of CMV infection in kidney transplant recipients, synthesise evidence based on laboratory markers that allow detection, in addition to showing the evolution of diagnostic methods and the usefulness of infection predictors to anticipate events, and finally, identify associated risk factors. An integrated understanding of these metrics can guide more effective preventive and preemptive surveillance strategies, with the potential to reduce clinical complications, preserve graft function, and optimise the prognosis of transplant patients.
Methodology
2
Protocol Registration
2.1
This systematic review was registered in the International Prospective Register of Systematic Reviews (PROSPERO) [9] under registration number CRD42024524165 (https://www.crd.york.ac.uk/PROSPERO/view/CRD42024524165). The review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA) guidelines [10].
Search Strategy
2.2
Searches were performed in PubMed, Web of Science, and LILACS up to March 2024, with filters for English, Spanish, and Portuguese languages and full‐text availability. The following descriptors were used: ‘Cytomegalovirus Infections’ [Mesh] OR ‘cytomegalovirus’ [Mesh] AND ‘Kidney Transplantation’ [Mesh] AND ‘Incidence.’ Equivalent strategies were applied across all databases. See supplement.
Eligibility Criteria
2.3
After screening the articles found through the search strategy, those that adequately met the inclusion and exclusion criteria were selected. For inclusion, cohort and case‐control studies published up to March 2024 that evaluated CMV infection in living patients after kidney transplantation, presenting data on the incidence of infection, were selected. Systematic reviews, meta‐analyses, letters to the editor, monographs, studies on infection by other viruses, transplantation of other organs, comparative incidence of medications, and studies without full text available were excluded.
Study Selection
2.4
Articles were imported into Rayyan [11] for screening. After duplicate removal, three reviewers (G.J., R.C., C.M.) independently assessed titles and abstracts. Discrepancies were resolved through consensus meetings. In cases where an agreement could not be reached, a fourth reviewer acted as a tie‐breaking mediator. Studies that met the criteria were read in full to confirm eligibility.
Data Extraction
2.5
Four authors (G.J., R.C., C.M., G.F.) extracted data into an Excel spreadsheet, including: author, publication year, title, country, study design, sample size, mean age, population, positive cases, follow‐up duration, incidence, time to infection onset, risk factors, diagnostic methods, laboratory variables and conclusions. The data were then included in a Excel worksheet.
Risk of Bias Assessment
2.6
The methodological quality of the included observational studies was assessed using the Newcastle‐Ottawa Scale (NOS) [12] tool, as recommended for cohort and case‐control studies. The instrument evaluates three parameters: selection, comparability and outcome/exposure, as can be seen in Table 1. The evaluation was made by one author (G.J.) and verified by two others (G.F. e M.A.). Risk of bias was then categorised as high, moderate, or low. The researchers resolved any discrepancies by jointly re‐evaluating a paper.
Statistical Analysis
2.7
For the data analysis of this meta‐analysis, the Jamovi Project programme (Jamovi version 2.4.8) was used. The incidence of CMV infection and their respective 95% confidence intervals (CI) were used as the ratio between the number of positive patients and the total number of patients included in the study. The incidence was expressed as a percentage. Heterogeneity between studies was assessed using the I^2^ statistic. Publication bias was assessed using the funnel plot, Egger's test, and Fail‐Safe N.
Results
3
Search Strategy
3.1
A total of 755 potentially eligible articles were identified for inclusion in this review. After removing duplicates (n = 44), 711 articles were screened by title and abstract using Rayyan [10]. Of these, 679 articles were excluded, and the remaining 32 were selected for full‐text reading. Subsequently, 17 studies were excluded: 7 for not providing sufficient incidence data, 5 for presenting comparative medication incidence, 2 for addressing kidney graft rejection incidence, 1 for reporting incidence in deceased patients, 1 for associating incidence with cancer, and 1 for being a meta‐analysis. After completing the eligibility assessment, 15 articles were included in the systematic review and meta‐analysis, as shown in Figure 1.
PRISMA flowchart.
Table 2 of the general characteristics of the studies shows the sample size (N) of each study, the total of them was 3888 (median of 159), the mean age was 45.1 and the mean follow‐up time was 7.14 months.
Risk Bias
3.2
To assess the methodological quality and risk of bias of the observational studies included in this systematic review, the Newcastle‐Ottawa Scale (NOS) [12] was used, and all 15 articles included were cohort articles and were endorsed by the NOS cohort model. The scale assigned up to 9 points distributed among the parameters.
In the Table 1, the studies evaluated obtained scores ranging from 6 to 9 points.
The presence of publication bias was also assessed using the funnel plot, as shown in Figure 2, in addition to the Fail‐Safe N = 11.326 (p < 0.001), Kendalls Tau = 0.067 (p = 0.770) and Egger's Regression = 0.633 (p = 0.527) tests. These results confirm that there is no evidence of publication bias, demonstrating the stability and reliability of this meta‐analysis.
Funnel plot for publication bias assessment. Funnel plot showing publication bias evaluation among the meta‐analysis included studies.
The funnel plot analysis was complemented by Kendall's Tau (value 0.124), Egger's regression (value 1.394), and Fail‐Safe N (363.000) tests. And despite the slight asymmetry in the funnel plot, none of the complementary tests showed significant evidence of publication bias, and the high Fail‐Safe N suggests that the results of the meta‐analysis are robust.
Statistical Analysis
3.3
The present meta‐analysis, consisting of 15 studies, identified a pooled incidence of CMV infection of 0.42 (95CI: 0.30%–0.54%), considering follow‐up periods ranging from 1 to 24 months. These results demonstrate a robust and clinically relevant finding. The I^2^ value was 98.75% (p < 0.001), showing high heterogeneity among the studies. Therefore, the meta‐analysis was carried out under a random‐effects model.
Figure 3 presents the individual results of the studies included in the meta‐analysis, as well as the estimated pooled effect. It is observed that, although some studies present wider confidence intervals or results that are not statistically significant in isolation, such as Toyoda et al. [15], Salazar et al. [4] and Shiina et al. [21], most of them demonstrate a consistent association with the occurrence of CMV infection in different clinical and population contexts.
Forest plot. Forest plot of the studies included in the meta‐analysis. Each line represents the point estimate and 95% confidence interval of each study. The black diamond represents the combined effect according to the random effects model, with an estimated value of 0.42 [0.30, 0.54].
The estimate evidenced reflects the aggregate prevalence of infection among the studies, considering methodological and sample variations. The studies with the greatest weight in the analysis, such as Sousa et al. [1], Pouteil‐Noble et al. [14], Hemmersbach‐Miller et al. [5] corroborate this finding, reinforcing the consistency of the data and the reliability of the results.
Despite the heterogeneity between the studies, possibly due to differences in diagnostic methods, populations evaluated and follow‐up periods, as demonstrated by Salazar et al. [4], Sousa et al. [1, 2] and Feng et al. [20], the findings support the clinical relevance of CMV infection in the context of kidney transplantation. The body of evidence supports the importance of virological monitoring and the implementation of appropriate preventive strategies, especially in higher‐risk groups, such as patients with D+/R serology–, children, and the elderly.
Also in Figure 3, it is observed that two works by the same author, Sousa et al. [1] and Sousa et al. [2], carried out in different years, presented very different incidences of CMV. The 2010 study recorded an incidence of 0.13 (95 CI: 11%–15%), while the 2021 study had a significantly higher incidence of 0.70 (95 CI: 66%–74%). A possible explanation for this discrepancy is the age profile of the populations analysed: in 2021, the authors included older patients (mean of 52 years), while in 2010 they evaluated younger patients (mean of 41 years). Considering that advanced age is a recognized risk factor for CMV infection, this demographic difference may have had a direct influence on the higher incidence observed in Sousa's study in 2021 [2].
Laboratory Predictors and Diagnostic Performance
3.4
In classic and contemporary series, qPCR detected CMV before serology, including as the only positive method in some cases, supporting its use as an early detection tool [16]. The pp65 antigenemia appeared, on average, on day 45. Cellular specific anti‐CMV immunity measured early predicted subsequent events, with a higher incidence of infection in patients with no or weak response [3]. ALC‐D28 (absolute lymphocyte count 28th day) < 1100/μL showed useful operational PPV (83% NPV) and a 3.3‐fold higher risk of CMV in the 1st year [21].
Positive IgM and viruria were associated with moderate/severe forms (ratio of 3.3 for severity with positive IgM) [14]. Low levels of MASP‐2 in the pre‐transplant period were associated with the development of CMV disease in the first 12 weeks (p = 0.028) [6]. In parallel, AECA (Anti‐endothelial antibodies) rose 1–4 weeks after detection of CMV DNA and remained high for months, suggesting endothelial injury and possible impact on rejection [15].
Some studies presented risk factors or reduction factors for infection among the patients studied, as shown in Table 1. Alakulppi et al. [17] observed a lower incidence when the donor has the IL‐10 genotype (−1082 AA), with a p‐value = 0.036. Feng et al. [20], showed more variations in risk factors.
The synthesis of clinical and laboratory predictors (Table 1) highlights important characteristics of early detection. qPCR identified subclinical infection before antigenemia, including as the only positive method in some cases [16]. Shiina et al. [21] It was observed that the absolute lymphocyte count on the 28th post‐transplant day (ALC‐D28 < 1100/μL) was associated with a higher incidence of CMV (HR = 3.32; VPN = 83%). In the study by Fernandéz‐Ruiz et al. [3] it was seen that reduced anti‐CMV specific cellular responses, assessed in the pre‐ and post‐immediate, predicted subsequent CMV events. And components of the complement lectin pathway, especially MASP‐2, have been associated with early CMV disease [6]. Together, these markers allow for reproducible risk stratification and guide surveillance and preemptive intervention (Table 3).
Discussion
4
Our findings reinforce that surveillance strategies anchored in laboratory predictors allow us to estimate the incidence and anticipate the risk of CMV infection in a comparable manner. Older studies, based on serology or antigenemia, probably underestimated the incidence and detected the events later [13, 14]. On the other hand, the progressive incorporation of molecular methods such as qPCR, since the end of the 90s [16] and monitoring of specific cellular immunity has shifted the identification of cases to earlier stages of the post‐transplant period and revealed subclinical infection. This methodological evolution explains part of the heterogeneity observed and, at the same time, justifies the inclusion of historical series to understand the trajectory of the disease over almost 3 decades [3, 21] (Table 4).
Based on the studies analysed, CMV infection continues to be a frequent event after kidney transplantation with a wide variation in incidence, according to diagnostic method, population profile, and follow‐up window. The study by Sousa et al. [2], reported an incidence of 8.8% between the third‐ and sixth‐months post‐transplant, while Feng et al. [20], found rates of 47% among recipients with unfavourable immunological and serological risk factors. Despite its high frequency, studies suggest that when identified and treated early and treated appropriately, CMV infection does not compromise the survival of the actual graft. When the infection is not controlled, it can cause acute rejection, viral nephropathy, and graft failure [1]. Shiina et al. [21] showed that patients with low cellular immunity had CMV infection of more worrisome clinical condition (HR = 3.32; 95% CI = 1.08–10.2).
Stratification by subgroups reinforced the clinical applicability of the findings. Children and the elderly had a higher incidence and severity of events [4, 5]. D+/R− serodiscordance remained the main risk factor for primary infection and disease [14]. In recipients of donors with expanded criteria, CMV was the most common complication, independently associated with infection by multidrug‐resistant microorganisms [1]. Such patterns not only reduce heterogeneity through more homogeneous comparisons, but also enrich the clinical relevance of the review by guiding who to monitor more closely, when, and with which tools.
The absence of direct analysis by immunosuppressive regimens can be understood as a limitation, but it was a conscious methodological option to avoid confusion due to the great variation of regimens in studies. Instead, we emphasise laboratory markers that are comparable over time and useful for preemptive treatments: serial qPCR as the screening axis [16], pp65 [13] and ALC‐D28 [21] to qualify initial risk, specific cellular immunity to modulate intensity [3] or duration of surveillance, and IgM/viruria as severity alarms [20].
In summary, by centring incidence on laboratory predictors and arranging markers in post‐transplant timelines, this review explains historical heterogeneity, standardises comparison between studies, and delivers actionable parameters for pre‐emptive surveillance and risk stratification in post‐kidney transplant care.
Conclusion
5
This review confirms that CMV infection remains one of the most frequent and clinically relevant infectious complications in kidney transplant recipients, presenting mainly in the first few months after the procedure. The estimated pooled incidence was 42% (95% CI: 30%–54%), with high heterogeneity (I^2^ = 98.75%), reflecting substantial differences between studies in terms of population profiles, immunosuppressive regimens employed, diagnostic methods, and prophylaxis strategies adopted.
By refocusing the analysis on laboratory markers, this work offers a practical and standardisable path for surveillance: serial qPCR as the basis of early detection, pp65 antigenemia as the typical operational window. ALC‐D28 < 1100/μL as a simple screening point to intensify follow‐up, MIC to modulate the frequency and duration of monitoring, and, as complementary signs, low MASP‐2 pre‐transplant and elevated AECA after viraemia, suggesting greater susceptibility and possible vascular impact.
This approach is independent of the variability of immunosuppressive regimens between centres and eras and speaks directly to the care routine: it allows for earlier action, personalisation of risk, and protection of the graft. Sensitivity analysis in modern scenarios where qPCR is the gold standard reinforces the robustness of these conclusions.
Author Contributions
The conceptualisation of the study was carried out by Gleice K. Jesus and Eduardo M. Netto. Data curation was conducted by Gleice K. Jesus, Róger J. Costa, Gabriel O. Franco and Cleyde C. S. Marconi. The formal analysis had the participation of Gleice K. Jesus, Gabriel O. Franco and Eduardo M. Netto, while the methodology was developed by Gleice K. Jesus, Róger J. Costa, Cleyde C. S. Marconi and Eduardo M. Netto. The project was managed by Gleice K. Jesus and Eduardo M. Netto. Statistical analysis was performed by Gleice K. Jesus, Gabriel O. Franco, Maria B. Arriaga and Eduardo M. Netto. The orientation was the responsibility of Eduardo M. Netto, and the validation was carried out by Gleice K. Jesus and Eduardo M. Netto. The original draft was written by Gleice K. Jesus, and all authors participated in the writing, revision, and editing, having access to all the data, contributing, revising, and approving the final version of this manuscript, as well as assuming final responsibility for the decision to submit it for publication.
Funding
GJ (166623/2023‐7) and CM (140187/2021‐9) are recipients of a Brazilian National Research Council (CNPq) scholarship; GF (88887.960010/2024‐00) and RC (8887.91553/2023‐00) are recipient of a Coordination for the Improvement of Higher Education Personnel scholarship (CAPES); the project received funding from CNPq (404193/2019.6). The funders were not involved in the conceptualisation, data extraction, analysis, preparation of the manuscript and the decision to publish.
Ethics Statement
The authors have nothing to report.
Consent
The authors have nothing to report.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Supporting Information S1
Supporting Information S2
Supporting Information S3
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1S. R. de Sousa , C. D. da Fonseca , M. Taminato , et al., “Infectious Events in Kidney Transplant Recipients From Deceased Expanded Criteria Donors: A Prospective Cohort,” Revista da Escola de Enfermagem 55 (2021): 1–8, 10.1590/1980-220x-reeusp-2021-0255.34545911 · doi ↗ · pubmed ↗
- 2S. R. Sousa , N. Z. Galante , D. A. Barbosa , and J. O. Pestana , “Incidence and Risk Factors for Infectious Complications in the First Year After Transplantation,” Jornal Brasileiro de Nefrologia 32, no. 1 (2010): 75–82, 10.1590/S 0101-28002010000100013.21448523 · doi ↗ · pubmed ↗
- 3M. Fernández‐Ruiz , E. Giménez , V. Vinuesa , et al., “Regular Monitoring of Cytomegalovirus‐Specific Cell‐Mediated Immunity in Intermediate‐Risk Kidney Transplant Recipients: Predictive Value of the Immediate Post‐Transplant Assessment,” Clinical Microbiology and Infection 25, no. 3 (March 2019): 381.e 1–381.e 10, 10.1016/j.cmi.2018.05.010.29803844 · doi ↗ · pubmed ↗
- 4M. Paulina Salazar E , A. Alba G , A. Deluchi B , et al., “Cytomegalovirus Infection and Disease in Children Undergoing Solid Organ Transplantation,” [Internet] (April 2008), www.sochinf.cl.
- 5M. Hemmersbach‐Miller , B. D. Alexander , D. L. Sudan , C. Pieper , and K. E. Schmader , “Infections After Kidney Transplantation: Does Age Matter?,” Clinical Transplantation 33, no. 4 (April 2019): e 13516, 10.1111/ctr.13516.30849194 PMC 6465112 · doi ↗ · pubmed ↗
- 6S. Sagedal , S. Thiel , T. K. Hansen , T. E. Mollnes , H. Rollag , and A. Hartmann , “Impact of the Complement Lectin Pathway on Cytomegalovirus Disease Early After Kidney Transplantation,” Nephrology Dialysis Transplantation 23, no. 12 (2008): 4054–4060, 10.1093/ndt/gfn 355.18577532 · doi ↗ · pubmed ↗
- 7C. zao Wu , C. X. qian , W. Z. yang , et al., “Simultaneous Monitoring of CMV and BKV by Quantitative PCR in Renal Transplant Recipients,” Journal of Virological Methods 210 (December 2014): 40–44, 10.1016/j.jviromet.2014.09.018.25261811 · doi ↗ · pubmed ↗
- 8F. Watzinger , K. Ebner , and T. Lion , “Detection and Monitoring of Virus Infections by Real‐Time PCR,” Molecular Aspects of Medicine 27, no. 2–3 (2006): 254–298, 10.1016/j.mam.2005.12.001.16481036 PMC 7112306 · doi ↗ · pubmed ↗