Double Trouble: Guillain-Barré Syndrome (GBS) Presenting as Overlapping Miller Fisher Syndrome (MFS) and Pharyngeal-Cervical-Brachial (PCB) Variant
Amit Kumar, Sandeep Garg, Praveen Bharti, Bhvika Zutshi

TL;DR
A rare case of Guillain-Barré Syndrome with overlapping features of two atypical variants is reported, emphasizing the need for early diagnosis and improved antibody testing.
Contribution
This case report highlights the coexistence of Miller Fisher Syndrome and Pharyngeal-Cervical-Brachial variant in Guillain-Barré Syndrome, reinforcing GBS as a spectrum disorder.
Findings
The patient showed progressive ophthalmoplegia, bulbar weakness, and upper limb weakness with areflexia.
Intravenous immunoglobulin treatment led to complete recovery at three months.
Anti-GQ1b and anti-GT1a IgG antibodies confirmed an immune-mediated process.
Abstract
Guillain-Barré Syndrome (GBS) is the leading cause of acute flaccid paralysis in India following the decline of poliomyelitis. Classical GBS typically presents with ascending symmetrical weakness and areflexia, while atypical variants, such as Miller Fisher Syndrome (MFS) and the Pharyngeal-Cervical-Brachial (PCB) variant, show distinct clinical patterns that are often under-recognized, particularly in resource-limited settings. This report describes a rare case of a 45-year-old previously healthy woman who developed progressive ophthalmoplegia, bulbar weakness, neck flexor weakness, and proximal upper limb weakness, along with areflexia, following a mild upper respiratory tract infection. Sensory function and lower limb motor strength remained intact. The differential diagnoses included brainstem stroke, myasthenia gravis, and diphtheritic polyneuropathy. Cerebrospinal fluid analysis…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1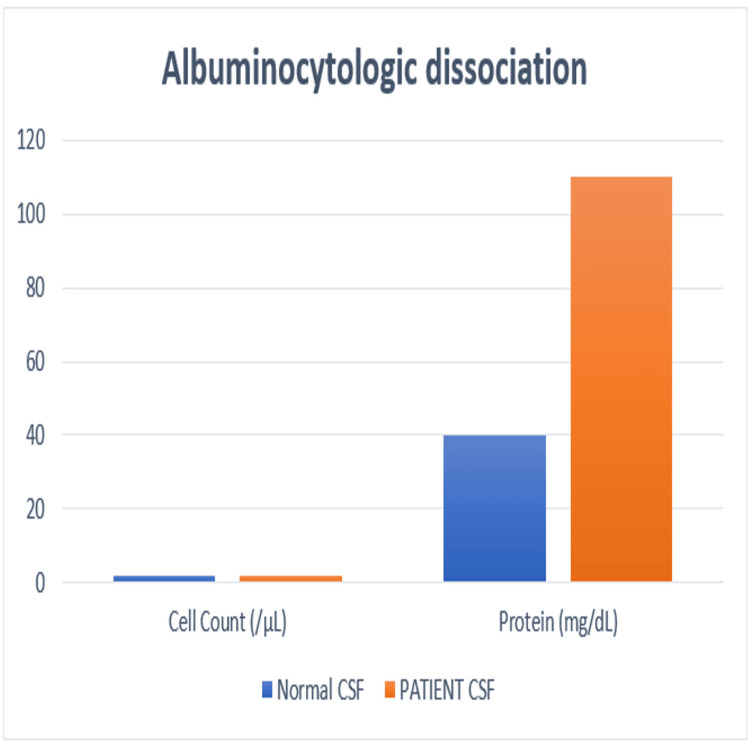 Figure 2
Figure 2| Test name | Result |
| Anti-ganglioside antibodies IgG | |
| GM1 | Negative |
| GM2 | Negative |
| GM3 | Negative |
| GD1a | Negative |
| GD1b | Negative |
| GT1a | Positive |
| GT1b | Negative |
| GQ1b | Positive |
| Antibodies against acetylcholine receptor | Negative |
| Antibodies against MuSK receptors | Negative |
| Day 0 | Fever episode |
| Day 1-11 | Progressive symptoms of diplopia, drooping of eye lids, dysarthria, and dysphagia, accompanied by neck weakness and upper limbs weakness |
| Day 12 | Presentation in emergency department |
| Day 13-19 | Progressive worsening |
| Day 15 | Starting of IVIG |
| Day 20 | Mild improvement |
| Week 4 | Near-complete recovery |
| 3 months | Full recovery with normal tests |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeripheral Neuropathies and Disorders · Facial Nerve Paralysis Treatment and Research · Long-Term Effects of COVID-19
Introduction
Guillain-Barré Syndrome (GBS) is an acute, immune-mediated polyradiculoneuropathy and is now the leading global cause of acute flaccid paralysis following the decline of poliomyelitis. In India, GBS has become a notable neurological emergency, with an estimated annual incidence of 1.5-2.7 per 100,000 population, though this is likely underestimated due to limited diagnostic access in rural regions [1,2]. Infectious triggers, such as Campylobacter jejuni, cytomegalovirus, Epstein-Barr virus, and *Mycoplasma pneumoniae, *commonly precede the illness and initiate an autoimmune response through molecular mimicry [3].
GBS usually presents with ascending symmetrical weakness, areflexia, and varying degrees of sensory or autonomic dysfunction. Typical variants include acute inflammatory demyelinating polyneuropathy (AIDP), acute motor axonal neuropathy (AMAN), and acute motor-sensory axonal neuropathy (AMSAN). Atypical variants, however, have been increasingly recognized, particularly in Asia. Among these, Miller Fisher Syndrome (MFS) and the Pharyngeal-Cervical-Brachial (PCB) variant are rare but clinically important subtypes [4].
MFS, first described in 1956, is defined by the triad of ophthalmoplegia, ataxia, and areflexia, and accounts for approximately 1%-5% of global GBS cases. It is more commonly observed in East Asia and is strongly associated with anti-GQ1b IgG antibodies, present in more than 85% of patients. This supports an autoimmune process targeting cranial nerves and neuromuscular junctions [5].
The PCB variant, described by Ropper in 1986, manifests with acute oropharyngeal, cervical, and upper limb weakness, with minimal or no lower limb involvement. Because of its presentation, it can mimic disorders such as myasthenia gravis or brainstem stroke, making diagnosis challenging. Anti-GT1a or anti-GQ1b antibodies are frequently detected in PCB cases, suggesting shared immunopathological mechanisms with other GBS variants [6].
Cases demonstrating overlapping features of MFS and PCB variants are uncommon but clinically significant. These presentations blur strict diagnostic categories and reinforce the concept of GBS as a spectrum rather than a collection of isolated syndromes. Such overlaps are especially vulnerable to misdiagnosis or delayed recognition in resource-limited settings where ganglioside antibody testing is unavailable or prohibitively expensive.
Case presentation
A 45-year-old previously healthy woman presented to the emergency department with a 12-day history of progressive diplopia, drooping of the eyelids, dysarthria, and dysphagia, accompanied by neck flexor weakness and an inability to raise both arms above shoulder level. She reported no fever, limb paresthesia, trauma, or bowel or bladder disturbances. One week earlier, she had experienced a mild upper respiratory tract infection, characterized by sore throat and rhinorrhea, which resolved spontaneously.
On examination, she was alert and oriented, with no signs of encephalopathy or meningeal irritation. Cranial nerve evaluation revealed bilateral external ophthalmoplegia with complete restriction of eye movements in all directions, along with partial bilateral ptosis (Figure 1). Assessment of the seventh cranial nerve showed bilateral lower motor neuron facial weakness. There was no gag reflex or palatal elevation, and her speech was dysarthric with a nasal quality.
Bilateral ptosis in the patient.
On motor examination, neck flexor strength was reduced to Medical Research Council (MRC) grade 3/5, and proximal upper limb weakness was noted, with deltoids and biceps graded at 2/5 bilaterally. Distal upper limb strength and all lower limb muscle power were normal. Deep tendon reflexes were absent throughout. Sensation, coordination, and gait were normal in all limbs; however, the patient was unable to sit or walk independently due to truncal instability and neck weakness. The differential diagnoses considered included brainstem stroke, myasthenia gravis, botulism, diphtheritic polyneuropathy, and GBS variants.
Routine laboratory tests, including hematological counts, renal and liver function tests, and electrolytes, were normal. The diphtheria throat swab was negative. Cerebrospinal fluid analysis showed a protein level of 110 mg/dL (normal 15-60 mg/dL) with 2 cells/mm³, consistent with albuminocytologic dissociation (Figure 2). Brain and cervical spine MRI findings were normal, with no evidence of infarction or demyelination. Nerve conduction studies (NCS) demonstrated prolonged distal latencies, reduced compound muscle action potential (CMAP) amplitudes, and absent F-waves in the upper limbs, indicating a demyelinating motor polyneuropathy predominantly affecting the upper limbs. Serology revealed positive anti-GQ1b IgG and anti-GT1a IgG antibodies. Antibodies to acetylcholine receptors and MuSK receptors were negative (Table 1).
Cerebrospinal fluid profile comparing normal values with findings in the patient, demonstrating albuminocytologic dissociation.
A diagnosis of GBS with overlapping MFS and PCB variants was established based on the clinical presentation, serological findings, and electrophysiological results. The patient was treated with intravenous immunoglobulin (IVIG) at 0.4 g/kg/day for five days, along with supportive care that included nasogastric feeding due to aspiration risk, close respiratory monitoring (no ventilatory support was required), and initiation of physiotherapy.
By day 7, the patient showed gradual improvement in ptosis and neck muscle strength. By week 3, there was near-complete recovery of ophthalmoplegia and upper limb function. At the three-month follow-up, the patient had fully recovered, with normal neurological examination findings, negative repeat anti-GQ1b antibody testing, and normalized nerve conduction study results (Table 2).
Discussion
GBS encompasses a broad group of acute immune-mediated polyradiculoneuropathies. The classic form is defined by ascending symmetrical weakness and areflexia, while atypical variants such as MFS and PCB present with more localized or distinct clinical features. This case, showing characteristics of both MFS and PCB variants, adds to the growing evidence that GBS subtypes fall along a continuum rather than functioning as isolated clinical entities [3].
The overlap of MFS and PCB is exceptionally rare but provides important insight into the clinical-immunological spectrum of GBS. One well-documented report described reversible nodo-paranodal conduction failure in an MFS/PCB overlap, supported by serial nerve conduction studies that showed rapid normalization of motor responses and delayed recovery of sensory potentials, findings consistent with reversible conduction failure rather than demyelination or axonal loss [6].
Another case described a 55-year-old man who was initially misdiagnosed with a possible posterior circulation stroke. He developed ophthalmoplegia, ataxia, mild dysarthria, and bilateral sensory loss in the hands, followed later by bulbar symptoms. Standard CT and MRI were normal, and once the overlap syndrome was recognized and IVIG was started, he showed rapid and sustained recovery [7]. Such cases highlight the need to maintain a broad differential diagnosis in patients presenting with cranial or bulbar deficits.
Our case aligns with this existing literature while contributing additional value by demonstrating dual antibody positivity (anti-GQ1b and anti-GT1a) along with an electrophysiological pattern of demyelinating motor neuropathy that predominantly affected the upper limbs. This antibody profile supports the diagnosis and helps distinguish these variants from mimics such as brainstem stroke or myasthenia gravis, where serology and conduction patterns differ. Together, the clinical picture, antibody findings, and neurophysiology provided a strong diagnostic foundation.
The GBS spectrum model proposed by Wakerley and Yuki conceptualizes these overlaps as part of a broader immunological and clinical continuum rather than discrete syndromes [4]. In one study of 60 patients with Fisher Syndrome, 50% demonstrated overlap features: 23% had PCB-type involvement, 15% progressed to classic GBS, and 12% showed characteristics of Bickerstaff brainstem encephalitis. These findings emphasize the dynamic and overlapping nature of these disorders [8].
From a prognostic standpoint, early initiation of IVIG is key. Previous reports associate timely IVIG therapy with marked improvement and full recovery over weeks to months. Our patient achieved complete recovery within three months, reinforcing the benefit of early immunotherapy in atypical or overlapping GBS presentations [7].
Conclusions
This example underscores the necessity for increased clinical vigilance about unusual and overlapping manifestations of GBS, especially in resource-limited environments where ganglioside antibody testing may be unavailable. Misdiagnosis or delayed intervention can result in considerable morbidity, including respiratory failure or progression of cranial nerve impairment. Consequently, doctors must uphold a heightened level of skepticism when faced with cranial nerve involvement accompanied by areflexia, even in the absence of typical ascending paralysis. By prioritizing accurate diagnosis and timely treatment, healthcare providers can mitigate the risks associated with GBS. This approach not only improves patient outcomes but also increases awareness about the disease's diverse presentations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Population incidence of Guillain-Barré syndrome: a systematic review and meta-analysis Neuroepidemiology Sejvar JJ Baughman AL Wise M Morgan OW 123133362011 http://dx.doi.org/10.1159/0003247102142276510.1159/000324710 PMC 5703046 · doi ↗ · pubmed ↗
- 2New chronic inflammatory demyelinating polyneuropathy/Guillain-Barré syndrome guidelines - impact on clinical practise Curr Opin Neurol Allen JA 455460372024 http://dx.doi.org/10.1097/WCO.00000000000012903887380110.1097/WCO.0000000000001290 · doi ↗ · pubmed ↗
- 3Guillain-Barré syndrome Lancet [Internet Willison HJ Jacobs BC van Doorn PA 717727201610.1016/S 0140-6736(16)00339-126948435 · doi ↗ · pubmed ↗
- 4Mimics and chameleons in Guillain-Barré and Miller Fisher syndromes Pract Neurol Wakerley BR Yuki N 90991520152523962810.1136/practneurol-2014-000937 · doi ↗ · pubmed ↗
- 5Guillain-Barré syndrome N Engl J Med Yuki N Hartung HP 2294230436620122269400010.1056/NEJ Mra 1114525 · doi ↗ · pubmed ↗
- 6Further regional variants of acute immune polyneuropathy. Bifacial weakness or sixth nerve paresis with paresthesias, lumbar polyradiculopathy, and ataxia with pharyngeal-cervical-brachial weakness Arch Neurol Ropper AH 671675511994 http://dx.doi.org/10.1001/archneur.1994.00540190051014801803910.1001/archneur.1994.00540190051014 · doi ↗ · pubmed ↗
- 7An Overlapping Case of Miller Fisher Syndrome and the Pharyngeal-Cervical-Brachial Variant of Guillain-Barré Syndrome Eur J Case Rep Intern Med Martins H Mendonça J Paiva D Fernandes C Cotter J 13877202010.12890/2020_001387 PMC 705097632133309 · doi ↗ · pubmed ↗
- 8How often and when Fisher syndrome is overlapped by Guillain-Barré syndrome or Bickerstaff brainstem encephalitis?Eur J Neurol Sekiguchi Y Mori M Misawa S Sawai S Yuki N Beppu M Kuwabara S 10581063232016 http://dx.doi.org/10.1111/ene.129832696988910.1111/ene.12983 · doi ↗ · pubmed ↗