The impact of neighborhood-level racial and economic segregation on low-risk cesarean delivery among Black, White, and Biracial (Black/White) individuals
Ella Batterson, Shira Goldenberg, Rebecca J. Baer, Gretchen Bandoli

TL;DR
This study examines how neighborhood segregation affects cesarean delivery rates among Black, White, and Biracial individuals, finding persistent disparities even after adjusting for factors like age and socioeconomic conditions.
Contribution
The study introduces a novel analysis of how neighborhood-level racial and economic segregation influences low-risk cesarean delivery disparities among Black, White, and Biracial individuals.
Findings
Black individuals had the highest low-risk cesarean delivery rates across all segregation levels compared to White individuals.
Biracial individuals had higher cesarean delivery rates than White individuals but not Black individuals, indicating complex health disparities.
Socioeconomic factors and maternal characteristics partially mediated the disparities in cesarean delivery rates.
Abstract
Research has established Black-White low-risk cesarean delivery (CD) disparities; however, it is unknown how select structural factors are involved in this disparity and whether Biracial (Black/White) individuals face similar disparities. Our objective was to estimate the association of low-risk CD among Black, White and Biracial individuals, and determine whether these associations vary by neighborhood level racial and economic segregation. Three hundred eighty-five thousand, eight hundred twenty-five nulliparous, term, singleton, vertex births among Black, White, and Biracial individuals in California (2011–2019) were included from a statewide administrative birth cohort of birth certificates linked to hospital records. We used a generalized estimating equation, Poisson regression stratified by Index of the Concentration of the Extremes (ICE) tertile to estimate risk ratios (RR) for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
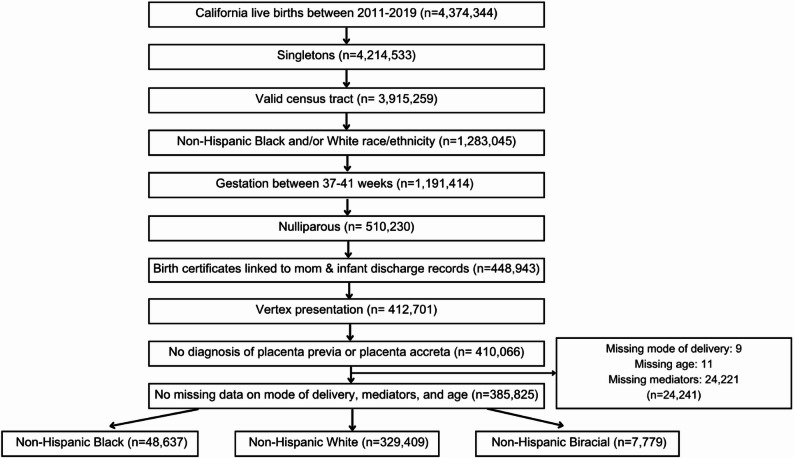 Figure 1
Figure 1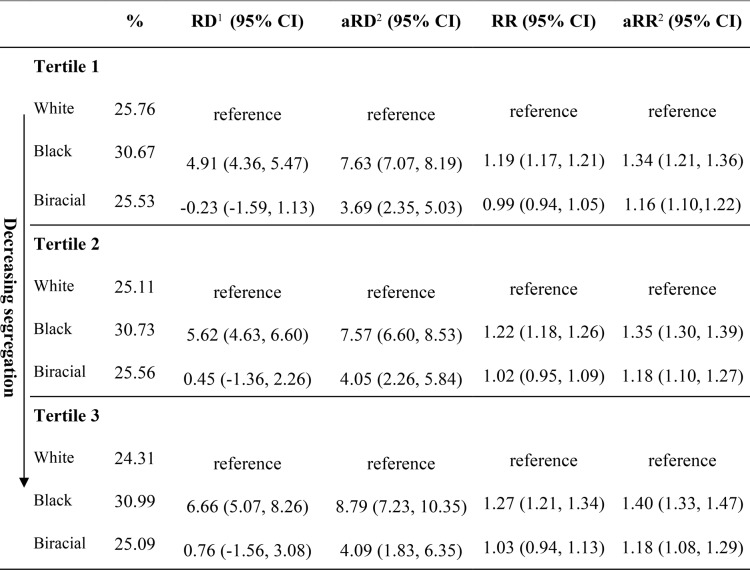 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMaternal and Perinatal Health Interventions · Migration, Health and Trauma · Maternal Mental Health During Pregnancy and Postpartum
Background
Low-risk cesarean delivery (CD) refers to nulliparous, term, singleton, and vertex (NTSV) births through cesarean sections. Cesarean deliveries can be lifesaving procedures when necessary, but they are major surgical interventions that can lead to adverse outcomes [1], including future subfertility and subsequent pregnancy risks such as placenta previa, uterine rupture, and stillbirth [2]. Given the risks associated with CD, Healthy People 2030 aims to decrease the low-risk CD rate to 23.6%. In 2019, California was able to achieve a low-risk CD rate of 22.8%; however, progress has been unequal and racial and ethnic disparities remain [3]. Among low-risk individuals in California, Black individuals have 1.3 times the risk of a CD compared to White individuals after adjusting for maternal age, maternal body mass index, hypertension, diabetes, gestational age, birthweight, and induction of labor [4]. Between 2011 and 2017, White individuals saw an 11% decrease in their low-risk CD rate, compared to a 1% decrease among Black individuals [4]. The unchanged CD disparity suggests that new interventions and policy changes are still needed to reach maternal health equity.
Maternal and infant disparities likely reflect broader underlying social and economic inequities perpetuated through racism and discrimination [5]. Structural racism refers to the large-scale systems, social forces, institutions, ideologies, and processes that interact to create and perpetuate inequalities among racial and ethnic groups [6]. Segregation measures are a common indicator of structural racism due to historical redlining policies that led to disinvestment in predominantly Black communities [7, 8]. Research has shown that aspects of structural racism measured through racial, economic, and residential segregation are associated with chronic health conditions and psychosocial factors that increase their risk for pregnancy-related complications [9–13]. In particular, Black individuals are more likely to have risk factors for CD, such as high body mass index (BMI) and diabetes, which are hypothesized to be due to lifelong exposure to intersecting systems of racism, sexism, and socioeconomic inequality that shape access to healthcare, nutrition, neighborhood conditions, and chronic stress physiology [10, 14]. A 2024 study in California using a neighborhood deprivation index reported that Black individuals had a higher risk of CD at all levels of socioeconomic disadvantage compared to White individuals [15]. The Index of the Concentration at the Extremes (ICE) score is a popular measure that accounts for spatial and economic polarization simultaneously using census-level race and income data, which helps decrease multicollinearity issues [8]. The ICE measure has demonstrated that social and economic segregation, as a proxy for structural racism, is associated with severe maternal morbidity (SMM) and preterm birth among Black individuals, but this measure has not been used to investigate the CD disparity [7, 15, 16].
While most maternal health research has examined Black-White disparities, there is a growing multiracial population in the United States, with the White and Black-identifying population growing by 67.4% from 2010 to 2020 [17]. Most health research has excluded the Biracial population due to the lasting impacts of the “one drop rule” used to categorize anyone with “Black blood” as Black [18]. Yet, a growing body of research supports disaggregation of the multiracial group, as differences in health outcomes have been revealed when specific subgroups of Biracial identities are compared [19]. Furthermore, a study comparing the risk of preterm birth among those who identified as Black and White revealed that they had a lower risk of preterm birth than their Black counterparts, but a higher risk than their White counterparts [20]. Since CD disparities are most pronounced when comparing Black to White individuals, examining the Biracial-White disparity will provide actionable evidence in this understudied population.
While we are aware of low-risk CD disparities among Black individuals, to our knowledge, there has been no published research examining the CD rates among Biracial groups, nor how racial and economic segregation could play a role in the low-risk CD disparity. Using a statewide birth cohort from California between 2011 and 2019, we examined whether racial disparities in low-risk CD are modified by a measure of racial and economic segregation in a population of Black, White, and Biracial individuals. We hypothesized that Black individuals would have the highest risk of CD compared to Biracial and White individuals, and that the racial disparity would be largest in areas that experience the most segregation. We further hypothesized that Biracial individuals would have a higher risk of CD than White individuals within areas that experience the most segregation.
Methods
Study design and population
The sample was drawn from the Study of Mothers and Infants (SOMI), an administrative birth cohort consisting of individuals who delivered liveborn infants in California between 2005 and 2021. To create the cohort, birth certificates were probabilistically linked to hospital, emergency department, and ambulatory surgery records from the Department of Health Care Access and Information (HCAI) for both mothers and infants, covering the period from one year before birth through one year after birth [20]. These linked records included diagnostic and procedure codes based on the International Classification of Diseases, 9th Revision (ICD-9), and 10th Revision, Clinical Modification (ICD-10) reported to HCAI by the hospitals. The SOMI was approved by the University of California, San Diego (UCSD) and the Committee for the Protection of Human Subjects within the Health and Human Services Agency of the State of California [21].
The sample was restricted to nulliparous, term (37- 41 weeks gestation) singleton vertex births delivered between 2011 and 2019 to women who identified as non-Hispanic Black, White, or Biracial. Additional inclusion criteria included a valid residence census tract and successful linkage of birth certificates and hospital discharge records for mother and infant. Individuals that had a fetus in nonvertex presentation and those with placenta previa or placenta accreta were excluded. Finally, we excluded those with missing data on BMI, education, adequacy of prenatal care, mode of delivery, age, primary attendant at birth, rurality, and payer source for delivery, resulting in a final sample of 385,825 (Fig. 1).
Fig. 1. Sample selection figure: California 2011–2019
Maternal characteristics
Maternal characteristics were selected to describe the study sample based on a review of the literature indicating their influence on cesarean delivery, as well as the availability of these data from birth certificates [1, 4, 7, 11, 13, 17, 22–27]. The characteristics included maternal age at delivery (years), maternal education (less than high school, high school degree or equivalent, some college, and college degree), insurance type (private, public, other), Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) enrollment (yes, no, missing), rurality (urban, rural), gestational age at delivery (37–41 weeks), induction of labor (yes, no), body mass index (BMI, kg/m2, calculated from pre-pregnancy weight and height), primary attendant at birth (midwife, M.D/D.O, other), and birthweight for gestational age (SGA, AGA, LGA). We assessed adequacy of prenatal care (adequate, intermediate, and inadequate), using the Adequacy of Prenatal Care Utilization (APNCU) index [28]. Hypertension and diabetes (pregestational or gestational) were obtained from maternal HCAI records and birth records. The data sources for outcomes, variables, and relevant ICD codes are provided in Supplemental Table 1.
Measurement of exposure & outcome
The sample was restricted to non-Hispanic Black, White, and Biracial populations to align with our study objective. We measured maternal race and ethnicity as reported on birth certificate records. The outcome of cesarean delivery was also abstracted from birth records from diagnoses and procedure codes based on the ICD-9 and ICD-10 as reported to the California Office of Statewide Health Planning and Development by the hospitals. The low-risk CD criteria was consistent with prior research and included nulliparous, term (37–41 week gestation), singleton, and vertex births without placenta previa or placenta accreta [4, 29].
Measurement of ICE tertiles
We linked the data with census tract annual 5-year estimate data available from the American Community Survey (ACS), 2011–2019 to generate ICE scores by census tract for each individual. The ICE_Race−Income_ score is a multidimensional measure used to examine racial and economic segregation [30]. The formula is defined as ICEi = (Ai-Pi)/Ti where i can be race, income, or race and income. The ICE_Race−Income_ measure combines data on income and race. Ai represents the privileged extreme consisting of White residents in the 80th income percentile (>25,000) in a given area [30]. The score assigns subjects a score from − 1 (most disadvantaged) to 1 (most advantaged) based on the area they live to calculate the directions of racial economic segregation [14]. The ICE_Race−Income_ score was calculated for each census tract using ACS annual 5-year estimates. A score was assigned to everyone in this analysis to represent the degree of racial and economic segregation based on where they live. ICE_Race−Income_ scores were categorized into three tertiles based on the study sample distribution with tertile one consisting of individuals living in census tracts with the highest concentration of low-income Black residents and tertile 3 consisting of the highest concentration of high-income White residents.
Mediator variables
Based on candidate Directed Acyclic Graphs (Supplemental Fig. 1), covariates were conceptualized as potential mediators given the lack of causal pathways between any measured variables and our primary exposures of race and ethnicity. The mediators included socioeconomic factors measured through education, rurality, insurance type, and WIC enrollment. Quality of care was measured through adequacy of prenatal care, primary attendant for birth, and induction of labor. Maternal characteristics included hypertension, diabetes, and pre-pregnancy BMI (underweight [< 18.5 kg/m2], normal [18.5–24.9 kg/m2], overweight [25.0–29.9 kg/m2], and obese [30.0 kg/m2]).
Statistical analysis
To test the relationship between race and ethnicity and CD we used Generalized Estimation Equation (GEE) Poisson regression to account for clustering by census tract. Models were stratified by ICE_Race−Income_ tertile to examine whether associations between race and ethnicity and CD differ by racial and economic segregation. Within each tertile, non-Hispanic White individuals served as the reference. We produced models to calculate both risk ratios and risk differences to estimate the relative and absolute measures of race and ethnicity on CD stratified by ICE_Race−Income_. To formally test for heterogeneity, a product term was included in the additive (risk difference) and multiplicative (risk ratio) models. The first set of models were unadjusted and the second were age-adjusted. While by definition age is not a confounder, we adjusted for it due to its well-documented association with CD and its imbalance across racial groups [24, 25]. Estimates included 95% confidence intervals, and no adjustment was made for multiple comparisons.
Mediation analysis
Finally, we conducted a decomposition analysis to assess the role of mediating factors between race and ethnicity and CD within the same ICE tertile. We used the SAS macro% mediation to obtain the natural direct effect, natural indirect effect, and proportion mediated by each mediator variable [31], and interaction was allowed for in models when present. Selected mediators included education, insurance type, primary attendant at birth, rurality, WIC enrollment, BMI, induction of labor, adequacy of prenatal care, hypertension, and diabetes.
Results
Descriptive results
The sample consisted of 385,825 low-risk births, among which 329,409 (85.4%) were Non-Hispanic White, 48,637 (12.6%) were Non-Hispanic Black, and 7,779 (2.0%) were Non-Hispanic Biracial birthing people (Table 1). Most of the Black population lived in the areas experiencing the highest racial and economic segregation that consist of predominantly Black and low-income residents (tertile 1). Although less than the Black population, most of the Biracial population (53.5%) also lived in these highly disadvantaged areas whereas the White population predominantly lived in tertiles 2 and 3 (73.9%).Table 1. Characteristics of low-risk births, overall and by race and ethnicity, California 2011–2019 (n = 385,825) Race and EthnicityTotal n = 385,**825 (%)**Non-Hispanic White n = 329,**409 (%)**Non-Hispanic Black n = 48,**637 (%)**Non-Hispanic Biracial^1^n = 7,**779 (%)**Mode of delivery Cesarean99,212 (25.71)82,297 (24.98)14,934 (30.71)1,981 (25.47)ICE Race-Income^2^ Tertile 1126,474 (32.78)85,971 (26.10)36,344 (74.73)4,159 (53.46) Tertile 2131,770 (34.15)120,526 (36.59)8,979 (18.46)2,265 (29.23) Tertile 3127,581 (33.07)122,912 (37.31)3,314 (6.81)1,335 (17.42)Age at delivery Median (IQR)29 (20–38)29 (21–37)25 (16–34)25 (16–34) 35 or more years60,191 (15.60)55,783 (16.93)3,820 (7.85)588 (7.56)Education Less than high school17,631 (4.50)10,448 (3.17)5,991 (12.32)922 (11.85) High school or equivalent72,6109 (18.82)54,474 (16.54)15,890 (32.67)2,246 (28.87) Some college77,625 (20.12)61,308 (18.61)14,022 (28.83)2,295 (29.50) College degree218,229 (56.56)203,179 (61.68)12,734 (26.18)2,316 (29.77)Insurance type Private274,291 (71.09)250,057 (75.91)20,236 (41.61)3,998 (51.39) Public99,920 (25.90)69,422 (21.07)26,916 (55.34)3,582 (46.05) Other11,614 (3.01)9,930 (3.01)1,485 (3.05)199 (2.56)WIC participation Yes104,298 (27.03)67,941 (20.63)32,210 (66.23)4,147 (53.31) No279,721 (72.50)259,841 (78.88)16,277 (33.47)3,603 (46.32) Unknown1,806 (0.47)1,627 (0.49)150 (0.31)29 (0.37)Rurality Urban289,341 (74.99)241,940 (73.45)41,483 (85.30)5,918 (76.08) Rural96,484 (25.01)87,469 (26.55)7,154 (14.70)1,861 (23.92)Adequacy of prenatal care Inadequate28,222 (7.31)20,507 (6.23)6,792 (13.96)923 (11.87) Intermediate58,202 (15.09)47,714 (14.48)9,100 (18.71)1,388 (17.84) Adequate299,401 (77.60)261,188 (79.29)32,745 (67.33)5,468 (70.29)Gestational age at delivery 37th week24,844 (6.44)20,280 (6.16)4,080 (8.39)484 (6.22) 38th week52,607 (13.63)43,400 (13.18)8,059 (16.57)1,148 (14.76) 39th week121,592 (31.51)103,235 (31.34)15,827 (32.54)2,530 (32.52) 40th week127,687 (33.09)110,322 (33.49)14,829 (30.49)2,536 (32.60) 41 st week59,095 (15.32)52,172 (15.84)5,842 (12.01)1,081 (13.90) Induction of labor214,272 (55.54)184,267 (55.94)25,770 (52.98)4,235 (54.44)Prepregnancy BMI (kg/m2) Underweight (< 18.5)16,989 (4.40)14,286 (4.34)2,321 (4.77)382 (4.91) Normal (18.5–25)218,121 (56.53)191,303 (58.62)21,378 (43.95)3,640 (46.79) Overweight (25–29.9.9)86,691 (22.47)72,402 (21.98)12,398 (25.49)1,891 (24.31) Obese (≥ 30)64,024 (16.59)49,618 (15.06)12,540 (25.78)1,866 (23.99)Primary attendant for birth M.D./D.O.335,780 (87.03)286,926 (87.10)42,166 (86.70)6,688 (85.98) Midwife^3^49,303 (12.78)41,855 (12.71)6,372 (13.10)1,076 (13.83) Other742 (0.19)628 (0.19)99 (0.20)15 (0.19)Birthweight for gestational age SGA37,298 (9.67)28,807 (8.50)8,344 (17.16)947 (12.17) AGA316,226 (81.96)272,051 (82.59)37,923 (77.97)6,252 (80.37) LGA32,301 (8.37)29,351 (8.91)2,370 (4.87)580 (7.46)Comorbidities Any hypertension^4^46,993 (12.18)38,206 (11.60)7,776 (15.99)1,011 (13.00) Pregestational5,857 (1.52)4,723 (1.43)1,016 (2.09)118 (1.52) Gestational20,297 (5.26)17,033 (5.17)2,822 (5.80)442 (5.68) Preeclampsia18,195 (4.72)14,305 (4.34)3,496 (7.19)394 (5.06) Any diabetes26,888 (6.97)23,377 (7.10)3,097 (6.37)414 (5.32) Pregestational2,521 (0.65)2,060 (0.63)412 (0.85)49 (0.63) Gestational24,367 (6.32)21,317 (6.47)2,685 (5.52)365 (4.69)Abbreviations: WIC The Special Supplemental Nutrition Program for Women, Infants, and Children, BMI body mass index, M.D. Doctor of Medicine, D.O. Doctor of Osteopathic Medicine, SGA small for gestational age, AGA appropriate for gestational age, LGA large for gestational age^1^Biracial refers to individuals who identified as two races: Black and White^2^ICERace−Income is the relative concentration of low-income Black households vs. high income White households in mothers’ ZIP code of residence; tertile one is the highest relative concentration of low-income Black households, and tertile three is the lowest^3^A midwife includes a certified nurse midwife, licensed midwife, or other midwife^4^The type of diagnosed hypertension was not always specified, leaving more individuals included in the “any hypertension” category than the subtypes
Descriptively, compared with the White population, the Black and Biracial populations had a younger median age at delivery (25 vs. 29 years), were more likely to be obese (Black: 25.8%; Biracial: 24.0%, White: 15.0%), and receive inadequate prenatal care (Black: 13.9%; Biracial: 11.9%, White: 6.2%;). The prevalence of public insurance, WIC enrollment, and small birthweight for gestational age among Biracial individuals fell in between those of Black and White individuals. Compared with Black individuals, the Biracial population was more similar to the White population in terms of living in a rural area and being diagnosed with preeclampsia.
Regression results
The highest prevalence of low-risk CD was in Black individuals (30.7%), followed by Biracial (25.4%) and White individuals (24.9%) (Table 1). There was little heterogeneity in this risk by ICE tercile (p_int_ >0.05), except for a slightly lower risk among White individuals from tertiles 1 to 3 (Table 2). Black individuals had a consistent increased risk for CD compared to White individuals across all tertiles, although estimates were fairly similar across tertiles (aRR_tertile1_: 1.34; 95% CI: 1.21, 1.36, aRR_tertile2_: 1.35; 95% CI: 1.30, 1.39, aRR_tertile3_: 1.40; 95% CI: 1.33, 1.47). After age adjustment, Biracial individuals had an increased risk for CD compared to White individuals in all tertiles, but lower than Black individuals (aRR_tertile1_: 1.16; 95% CI: 1.10, 1.22, aRR_tertile2_: 1.18; 95% CI: 1.10, 1.27, aRR_tertile3_: 1.18; 95% CI: 1.08, 1.29). Among Biracial individuals, there was no heterogeneity in CD risk estimates by ICE tercile (p_int_ >0.05). On the absolute scale, the difference in the risk of CD between Black and White individuals was also consistent across tertiles, and the disparity was largest in tertile 3 (aRD_tertile1_: 7.63%; 95% CI: 7.07%, 8.19%, aRD_tertile2_: 7.57%; 95% CI: 6.60%, 8.53%, aRD_tertile3_: 8.79%; 95% CI: 7.23%, 10.35%). The difference in the risk of CD between Biracial and White individuals increased after age adjustment (aRD_tertile1_: 3.69%; 95% CI: 2.35%, 5.03%, aRD_tertile2_: 4.05%; 95% CI: 2.26%, 5.84%, aRD_tertile3_: 4.09%; 95% CI: 1.83%, 6.35%).Table 2. Association between race and ethnicity and low-risk CD by ICE_Race-Income_, California 2011-2019Abbreviations: CD cesarean delivery, RD risk difference, RR risk ratio
Mediation results
In mediation analyses comparing Black and White individuals, being overweight or obese (BMI 25+) was the most substantial mediator (tertile 1: 19.00%, tertile 2: 21.13%, tertile 3: 21.93%) (Table 3). WIC enrollment slightly mediated the low-risk CD disparity in tertiles 1 and 2 (tertile 1: 9.63%, tertile 2: 12.90%, tertile 3: 5.11%), whereas having public insurance mediated approximately 12% in tertiles 1 and 3. Hypertension contributed to a small part of the low-risk CD disparity, with a greater effect in tertile 1 (tertile 1: 9.98%, tertile 2: 8.15%, tertile 3: 6.29%). Similar patterns were observed in the mediation analyses comparing Biracial to White individuals. Having a BMI ≥ 25 was the most substantial mediator (tertile 1: 27.49%, tertile 2: 35.28%, tertile 3: 26.19%), and WIC enrollment mediated more of the disparity among Biracial individuals compared to Black individuals (tertile 1: 31.68%, tertile 2: 17.68%, tertile 3: 13.10%) (Table 4). Primary attendant at birth, induction, adequacy of prenatal care, rurality, and diabetes did not act as mediators.Table 3. Age-adjusted risk ratios for low-risk CD comparing black to white individuals by ICE_Race-Income_, California 2011–2019Tertile 1 (most segregated)Tertile 2Tertile 3 (least segregated)High School or Less vs. Some College or Higher Natural Direct Effect1.33 (1.30, 1.36)*1.35 (1.29, 1.40)1.38 (1.30, 1.48) Natural Indirect Effect1.01 (1.00, 1.01)*1.00 (1.00, 1.00)1.00 (1.00, 1.01) Proportion mediated2.52%*0.98%*2.51%*Midwife vs. other primary attendant at birth Natural Direct Effect1.35 (1.32, 1.38)1.34 (1.29, 1.40)1.39 (1.31, 1.48) Natural Indirect Effect0.98 (0.98, 0.99)1.00 (0.99, 1.01)1.00 (0.99, 1.02) Proportion mediated0.0%0.0%0.0%Induction Natural Direct Effect1.34 (1.31, 1.37)*1.34 (1.29, 1.40)1.40 (1.31, 1.48) Natural Indirect Effect1.00 (1.00, 1.00)*1.00 (1.00, 1.00)1.00 (1.00,1.00) Proportion mediated0.03%*0.47%0.53%Overweight or Obese Natural Direct Effect1.27 (1.24, 1.30)1.27 (1.22, 1.32)1.31 (1.23, 1.39) Natural Indirect Effect1.05 (1.04, 1.05)1.06 (1.05, 1.06)1.07 (1.06, 1.07) Proportion mediated19.00%21.13%21.93%Public vs. Private insurance Natural Direct Effect1.30 (1.27, 1.33)1.32 (1.27, 1.38)*1.34 (1.26, 1.42) Natural Indirect Effect1.03 (1.03, 1.04)1.02 (1.01, 1.03)*1.04 (1.03, 1.04) Proportion mediated12.59%7.13%*12.52%Inadequate Prenatal Care Natural Direct Effect1.34 (1.20, 1.37)1.34 (1.29, 1.40)1.39 (1.31, 1.48) Natural Indirect Effect1.00 (1.00,1.00)1.00 (1.00, 1.00)1.00 (1.00, 1.00) Proportion mediated0.72%0.98%0.70%WIC Natural Direct Effect1.28 (1.25, 1.32)*1.33 (1.27, 1.39)1.32 (1.23, 1.42) Natural Indirect Effect1.02 (1.02, 1.04)*1.00 (0.99, 1.02)1.01 (1.00, 1.03) Proportion mediated9.63%*12.90%*5.11%*Rural vs. Urban Natural Direct Effect1.36 (1.32, 1.39)1.37 (1.31, 1.42)1.40 (1.32, 1.50) Natural Indirect Effect0.99 (0.98, 0.99)0.98 (0.98, 0.99)0.99 (0.99, 1.00) Proportion mediated0.0%0.0%0.0%Any Hypertension^1^ Natural Direct Effect1.30 (1.27, 1.33)1.32 (1.27, 1.37)1.37 (1.29, 1.46) Natural Indirect Effect1.03 (1.02, 1.03)1.02 (1.02, 1.03)1.02 (1.01, 1.02) Proportion mediated9.98%8.15%6.29%Any Diabetes^2^ Natural Direct Effect1.34 (1.31, 1.37)1.34 (1.29, 1.40)1.39 (1.31, 1.48) Natural Indirect Effect1.00 (1.00, 1.00)1.00 (1.00, 1.00)1.00 (1.00, 1.00) Proportion mediated0.0%1.05%0.58%*Indicates and interaction was present between the mediator and race^1^Any hypertension includes preeclampsia, unspecified, pregestational, and gestational hypertension^2^Any diabetes includes unspecified, pregestational, and gestational diabetesTable 4Age-adjusted risk ratios for low-risk CD comparing biracial to white individuals by ICE_Race-Income_, California 2011–2019Tertile 1 (most segregated)Tertile 2Tertile 3 (least segregated)High School or Less vs. Some College or Higher Natural Direct Effect1.14 (1.08, 1.22)1.17 (1.07, 1.27)1.16 (1.04, 1.29) Natural Indirect Effect1.00 (1.00, 1.01)1.00 (1.00, 1.01)1.01 (1.00, 1.01) Proportion mediated1.92%2.37%4.39%Midwife vs. other primary attendant at birth Natural Direct Effect1.16 (1.09, 1.24)1.20 (1.11, 1.31)1.19 (1.07, 1.32) Natural Indirect Effect0.99 (0.98, 1.00)0.97 (0.96, 0.99)1.00 (0.98, 1.02) Proportion mediated0.0.%0.0.%0.0.%Induction Natural Direct Effect1.16 (1.09, 1.23)*1.18 (1.09, 1.28)1.18 (1.06, 1.31) Natural Indirect Effect1.00 (1.00, 1.00)1.00 (1.00, 1.00)1.00 (1.00,1.01) Proportion mediated0.0.%0.50%1.66%Overweight or Obese Natural Direct Effect1.11 (1.04, 1.18)1.12 (1.03, 1.21)1.13 (1.02, 1.26) Natural Indirect Effect1.05 (1.04, 1.05)1.06 (1.05, 1.07)1.04 (1.03, 1.05) Proportion mediated27.49%35.28%26.19%Public vs. Private insurance Natural Direct Effect1.13 (1.06, 1.21)1.15 (1.06, 1.25)1.19 (1.06, 1.33) Natural Indirect Effect1.02 (1.01, 1.02)1.02 (1.01, 1.02)1.00 (0.99, 1.02) Proportion mediated11.71%10.15%1.51%*Inadequate Prenatal Care Natural Direct Effect1.15 (1.08, 1.23)1.18 (1.09, 1.28)1.18 (1.06, 1.32) Natural Indirect Effect1.00 (1.00,1.00)1.00 (1.00, 1.00)1.00 (1.00, 1.00) Proportion mediated0.68%0.63%0.58%WIC Natural Direct Effect1.11 (1.04, 1.18)1.14 (1.05, 1.24)1.15 (1.03, 1.27) Natural Indirect Effect1.05 (1.04, 1.05)1.03 (1.02, 1.03)1.02 (1.01, 1.02) Proportion mediated31.68%17.68%13.10%Rural vs. Urban Natural Direct Effect1.16 (1.10, 1.24)1.19 (1.10, 1.29)1.19 (1.07, 1.32) Natural Indirect Effect0.99 (0.99, 1.00)0.99 (0.99, 0.99)1.00 (0.99, 1.00) Proportion mediated0.0.%0.0.%0.0.%Any Hypertension^1^ Natural Direct Effect1.14 (1.07, 1.21)1.17 (1.08, 1.27)1.17 (1.05, 1.31) Natural Indirect Effect1.01 (1.01, 1.02)1.01 (1.00, 1.02)1.01 (1.00, 1.02) Proportion mediated9.78%5.95%5.71%Any Diabetes^2^ Natural Direct Effect1.15 (1.08, 1.23)1.18 (1.09, 1.29)1.18 (1.06, 1.32) Natural Indirect Effect1.00 (0.99, 1.00)1.00 (0.99, 1.00)1.00 (1.00, 1.00) Proportion mediated0.0.%0.0.%0.0.%*Indicates and interaction was present between the mediator and race^1^Any hypertension includes preeclampsia, unspecified, pregestational, and gestational hypertension^2^Any diabetes includes unspecified, pregestational, and gestational diabetes
Discussion
In this study, the prevalence of CD was greatest in Black individuals (30.71%), followed by Biracial (25.47%) and White (24.98%) individuals, equating to approximately 4–9 excess low-risk CDs in Biracial and Black individuals, respectively, per 100 deliveries after age adjustment. The prevalence is slightly lower compared to other studies which is likely due to the decrease in CD incidence in more recent years [4, 29]. We did not find support for our hypothesis of differential risk by census-level racial and economic segregation, as there was little difference in risk estimates across tertiles. In mediation analyses, BMI, insurance type, hypertension and WIC enrollment had the strongest mediating effects.
Our findings were consistent with another study investigating low-risk CD among California individuals using a neighborhood deprivation index, which found that Black individuals had an increased risk of CD compared to White individuals at all levels of advantage [29]. Despite overlapping confidence intervals across tertiles, we observed a very modest increase in the disparity with decreasing racial and economic segregation, with the highest risk disparities occurring in areas with the least racial and economic segregation. This differed from our hypothesis that the racial disparity would be largest in the areas that experience the most structural racism. The results appear to be due to the slight decline in prevalence of low-risk CD among White individuals in areas of less racial and economic segregation that was not observed among Black and Biracial individuals. This study was novel in its examination of potential mediators that could explain the observed low-risk CD disparity by race and ethnicity. The greater mediating effect of WIC enrollment on the low-risk cesarean delivery disparity in tertiles 1 and 2 supports its role as a proxy for income status. This suggests that a larger proportion of Black and Biracial individuals may experience low-income status and food insecurity than White individuals, contributing to the low-risk CD disparity. We also found that being overweight or obese mediated 19–22% of the Black-White low-risk CD disparity across tertiles. In this analysis, Black individuals had a higher prevalence of obesity and hypertension than White individuals, which is a known risk factor for CD along with gestational hypertension and diabetes [32, 33].
Policy and program recommendations
The lack of substantial variation in the low-risk CD disparity by racial and economic segregation, as well as the relatively modest contribution of mediators, suggests that future intervention efforts need to use data sources that capture a larger and more contextual framework of risk factors. However, the persistent racial disparities noted across studies call for actions. Research has revealed that Black individuals who had a CD in their first pregnancy have low rates of shared decision making with their providers [34]. CD rates are consistently lower in birth centers that follow models involving prenatal care around birth preparation, relationship building between the patient and midwife, and shared decision making [35]. Clinicians’ education should include continuous cultural competency training that addresses implicit biases and shows how to create a supportive relationship with their patients [36]. Shifting typical hospital care to focus on building patient relationships, shared decision making, and increasing opportunities for racially concordant care can improve the maternal experience, promote agency, and increase health literacy [35, 37]. Implementing a standardized labor induction protocol at hospitals is also associated with a decreased CD rate among Black individuals, indicating that having clear labor management guidelines can mitigate the potential for implicit bias from physicians in the CD decision process [38]. While these findings need confirmation, our data suggest that obesity prevention could be a beneficial pathway for public health interventions among Black and Biracial populations to reduce the CD rate and promote maternal health. In addition, Black and Biracial individuals enrolled in WIC may be an important priority population for maternal health interventions to reduce stress and improve healthy food access before, during, and after pregnancy.
Limitations and strengths
Strengths of this study include its large sample and ability to include the Biracial population. This study was restricted to Black and White racial groups; although other racial and ethnic minorities experience significant disparities in maternal and birth outcomes, these populations were not included due to the study’s scope [39]. To better inform public health practices, we calculated both relative and absolute risks and performed a mediation analysis instead of adjusting for maternal characteristics to avoid blocking pathways that can be evaluated as intervention targets. The ICE_Race−Income_ score allowed us to capture the collective impact of census tract level racial and economic segregation on the low-risk CD disparity; However, it does not recognize the extent of travel between neighborhoods, individual level exposures to racism, or residential mobility during pregnancy. Due to ACS data limitations, the score was modeled to include only Black and White individuals and could not include Biracial individuals. We also relied on administrative data which may fail to capture the reasons for CD and other factors that influence the disparity. Finally, we were not able to examine institutional practices or norms for thresholds for CD, which may affect findings and limit generalizability of our results.
Conclusion
In this California cohort, the Black-White low-risk CD disparity persisted but was not affected by racial and economic segregation. Biracial individuals also experienced a higher risk of CD than White individuals, but a lower risk of CD than Black individuals suggesting that they experience simultaneous advantages and disadvantages to their monoracial counterparts. Further research should examine the role of indications for CD. Additionally, a qualitative assessment of an individual’s experiences in the hospital during labor could contextualize the persistent disparity in CD by race and ethnicity. Finally, further research is recommended to understand the potentially unique experiences of Biracial populations.
Supplementary Information
Supplementary Material 1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Teal EN, Anudokem K, Baer RJ, Jelliffe-Pawlowski L, Mengesha B. Racial disparities in the rates of and indications for Cesarean delivery in california: are they changing over time? Am J Perinatol. 2024;41(1):31–8. 10.1055/s-0041-1740071. Epub 2 Dec 2021. PMID: 34856615.10.1055/s-0041-174007134856615 · doi ↗ · pubmed ↗
- 2Latoya Hill A, Rao S, Artiga, Ranji U. Racial Disparities in Maternal and Infant Health: Current Status and Efforts to Address Them. 2024. Available from: https://www.kff.org/racial-equity-and-health-policy/racial-disparities-in-maternal-and-infant-health-current-status-and-efforts-to-address-them/. Cited 26 Oct 2025.
- 3Tobin-Tyler L. Black Mothers Matter: The Social, Political and Legal Determinants of Black Maternal Health across the Lifespan. SSRN Electron J. 2021. Available from: https://www.ssrn.com/abstract=3926765. Cited 30 Oct 2024.
- 4Bayrampour H, Heaman M. Advanced maternal age and the risk of Cesarean birth: A systematic review. Wiley Online Libr. 2010. https://onlinelibrary.wiley.com/doi/10.1111/j.1523-536X.2010.00409.x.10.1111/j.1523-536X.2010.00409.x 20887538 · doi ↗ · pubmed ↗
- 5NM-IBIS -The Kotelchuck Index. https://ibis.doh.nm.gov/resource/Kotelchuck.html.
- 6Bane S, Mujahid MS, Main EK, Carmichael SL. Socioeconomic disadvantage and racial/ethnic disparities in low-risk cesarean birth in California. Am J Epidemiol. 2024. Available from: https://academic.oup.com/aje/advance-article/doi/10.1093/aje/kwae 157/7699733. Cited 17 Sep 2024.10.1093/aje/kwae 157PMC 1173596938932570 · doi ↗ · pubmed ↗
- 7Shuler TO. Promoting Shared Decision-making in Maternal Health Care. N C Med J. 2023;84(1). Available from: https://ncmedicaljournal.com/article/67779-promoting-shared-decision-making-in-maternal-health-care. Cited 21 Apr 2025.
- 8Rf H, Sk S, Ld L. A standardized labor induction protocol: impact on racial disparities in obstetrical outcomes. Am J Obstet Gynecol MFM. 2020;2(3). Available from: https://pubmed.ncbi.nlm.nih.gov/33345879/. Cited 29 Oct 2024.10.1016/j.ajogmf.2020.10014833345879 · doi ↗ · pubmed ↗