Efficacy of interventions to prevent eating disorders in people with type 1 diabetes: a systematic review
Neisha D’Silva, Nikka S. Sandoval, Kerri M. Gillespie, Line Wisting, Christel Hendrieckx, Eric Stice, Lee Jones, Sean N Gannon, Warren Ward, Melanie White, Selena E. Bartlett

TL;DR
People with type 1 diabetes are at higher risk of eating disorders, and this review evaluates interventions to prevent them, finding that cognitive dissonance-based programs are most effective.
Contribution
The study systematically reviews interventions for preventing eating disorders in type 1 diabetes patients, highlighting cognitive dissonance-based programs as most effective.
Findings
Cognitive dissonance-based programs showed the most consistent reduction in eating disorder risks and symptoms.
Most interventions had negligible impact on improving glycemia.
Studies were limited by small sample sizes, high drop-out rates, and short follow-up periods.
Abstract
Individuals with type 1 diabetes (T1D) are at increased risk of developing disordered eating (DE) and eating disorders (ED). Diabetes self-management focuses on food and insulin administration, which may contribute to development of EDs. The dual diagnosis may contribute to suboptimal glycemia, early diabetes-related complications and mortality. Evidence for ED prevention programs for this high-risk population remains limited. This systematic review aims to evaluate the feasibility and efficacy of available interventions to prevent EDs and improve glycemia in people with T1D. A literature search of PubMed, Embase, PsycINFO, CINAHL and Web of Science was conducted on 25 January 2025. Studies using randomized controlled, quasi-experimental or cohort design that targeted ED prevention in T1D population were included. Nine studies met the inclusion criteria, featuring interventions such…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
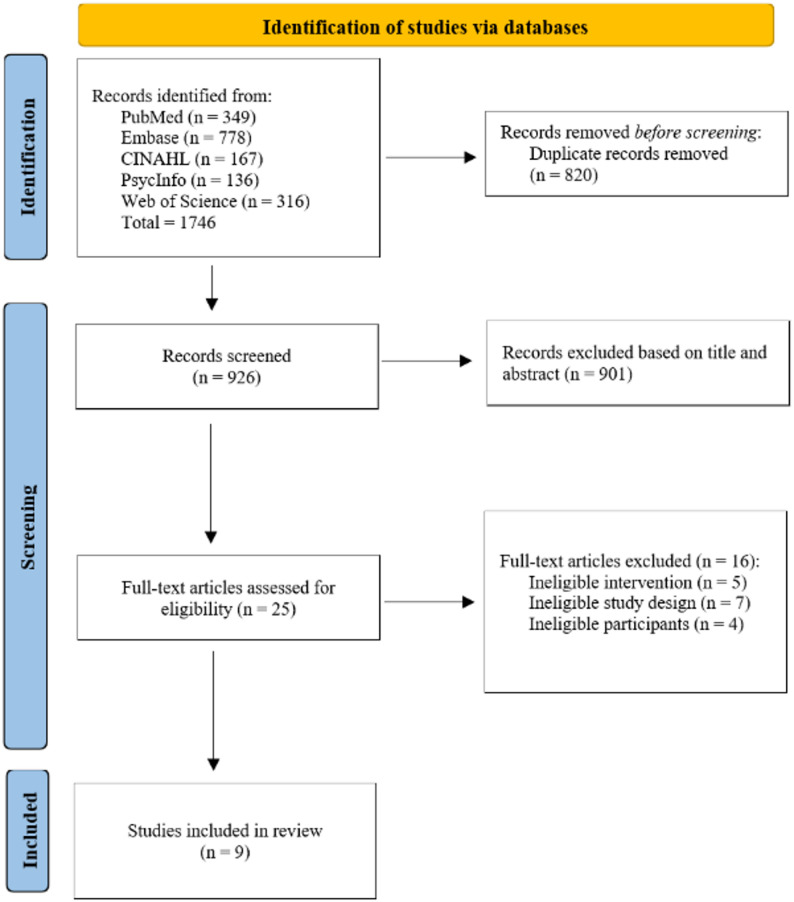 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetes Management and Research · Diabetes Management and Education · Eating Disorders and Behaviors
Introduction
The last 40 years have seen a greater awareness of the high prevalence of disordered eating (DE) and eating disorders (ED) in people with type 1 diabetes (T1D). The diagnostic criteria based on the DSM-5-TR [1], have been revised to include insulin omission, a unique ‘purging’ behavior employed by those with diabetes for weight loss (partially through inducing a catabolic state) [2]. DE occurs on a spectrum of severity from mildly disturbed thoughts and behaviors regarding weight, shape and eating to more concerning thoughts and behaviors with medical and mental health consequences that do not meet the formal criteria for an ED [3].
With the median age of onset at 14–19 years [4], the prevalence of DE in adolescent females with T1D may be as high as 40–50% and 13–18% in males [4, 5]. Adolescents with T1D are more than twice as likely to develop EDs compared to their peers without diabetes [4]. A recent systematic review and meta-analysis confirmed that T1D is associated with increased risk of ED compared with individuals without diabetes (RR = 2.47, 95% CI = 1.84–3.32, p < 0.00001) and reports a prevalence of insulin omission/restriction at 10.3%, predominantly in females [6]. This is partially due to the behavioral changes required for diabetes self-management (e.g. adjusting insulin doses with food intake and exercise) [7]. A longitudinal study found that 92% of female adolescents who reported DE at baseline continued to report DE at the 5-year follow-up, suggesting its persistent nature [8].
Prospective studies have identified risk factors that predict future onset of EDs, such as pressure for thinness, pursuit of the thin appearance ideal and body dissatisfaction [7, 9, 10]. Adolescents who report body dissatisfaction were more likely to restrict insulin, suggesting that this may be a particularly important risk factor for people with T1D [10]. Whilst females often strive for thinness, males may desire increased muscularity [5, 11]. In general, young people with T1D who perceive more significant disturbances with body image, shape and weight are more likely to omit insulin compared to those who do not, leading to glucose levels above target.
Evidence suggests that in addition to ED-specific complications, the dual diagnosis of T1D and ED (referred to as ED-T1D) can exponentially increase the risk of early onset of diabetes-related complications such as nephropathy, neuropathy and retinopathy [12]. Adolescents and young adults with T1D and ED have more than triple the risk of diabetic ketoacidosis (DKA) and nearly sixfold increased risk of death compared with their peers without eating disorders [13].
Local and international guidelines recommend regular assessment of psychological well-being in those with T1D [3, 14–17] with a view to early detection and management of DE to avoid the progression to an ED. The clinical inertia amongst health care professionals to screen, is partly due to a perceived lack of support and evidence-based interventions to prevent or treat DE in T1D [18].
A systematic review in 2017 [19] highlighted the limited evidence of interventions to prevent and/or treat DE or ED in T1D. After assessing the identified studies, based on the quality of intervention description and methodology, only six studies were deemed suitable for further analysis. Interventions identified were inpatient therapy, psychoeducation, cognitive behavioral therapy, multi-disciplinary approaches or family involvement. Whilst there were some improvements in ED psychopathology with some interventions, limited or no improvement in glycemia was observed.
Since this publication there have been substantial developments in interventions aimed at preventing ED-T1D. These have largely used cognitive dissonance theory to develop novel, co-designed programs that can be delivered in a variety of ways (such as online or with peer-facilitation). The methodologies in these studies vary from feasibility to large multicenter randomized controlled trials (RCT). Technological advancements in glucose monitoring (e.g., continuous glucose monitoring that measures glucose time-in-range) have allowed for better evaluation of interventions on glycemia. This systematic review evaluated the feasibility and efficacy of interventions to prevent ED and improve glycemia in people with T1D. Given the severe short- and long-term consequences of ED-T1D, there is a critical need for prevention strategies that target modifiable ED risk factors.
Methods
The review follows Preferred Reporting Items for Systematic reviews and Meta-analyses (PRISMA 2020) and was registered with PROSPERO international prospective register of systematic reviews (ID: CRD420250649449).
Search strategy
A comprehensive literature search (25 January 2025) was conducted across PubMed, Embase, PsycINFO, CINAHL and Web of Science (Appendix 1). Keywords included: “disordered eating”, “eating disorders”, “type 1 diabetes”, “intervention”. Subject headings (e.g. MeSH in PubMed) were employed. The search was limited to English-language, peer-reviewed publications. Citation chaining and hand searches identified no additional studies. Previous and current systematic reviews were searched in the databases listed, Cochrane Library and PROSPERO registry. One prior systematic review (2017) addressed ED prevention and treatment for people with T1D [19]. Our systematic review updates and narrows the focus to prevention, including two studies from that review.
Inclusion and exclusion criteria
- Included: Randomized Control Trials (RCT), quasi-experimental and cohort studies reporting primary data on ED prevention in T1D.
- Excluded: Cross-sectional, case-control, qualitative studies; non-primary data (reviews, commentaries, abstracts); non-English papers; studies aimed at treating (versus preventing) participants with either established ED or ED determined by a comprehensive clinical assessment using DSM-5-TR.
Study selection
Two authors (ND and NS) independently screened titles/abstracts in Covidence. Disagreements were resolved by a third reviewer (KG). Full-text articles were reviewed similarly.
Data extraction
Two authors (ND and NS) extracted data independently, with biostatistician input for accuracy. Extracted data included author, year, country, design, sample details, intervention/ control conditions, clinical measures, outcomes and study strengths/limitations.
Clinical measures
- Person-reported outcome measures PROMs: diabetes-specific ED symptoms, body dissatisfaction, thin-ideal internalization, diabetes distress and general psychopathology (symptoms of anxiety/ depression, general well-being).
- Glycemia measures: HbA1c (mean glucose concentration over 8–12 weeks) and TIR (percentage of time in target glucose range, >70% considered optimal [20]). Studies under 3 months’ duration were unable to assess HbA1c meaningfully.
Data synthesis and quality assessment
Meta-analysis was not feasible due to heterogeneity in design, intervention, population (particularly different age ranges and gender inclusion) and outcomes, making pooling results and direct comparisons difficult. Further, the number of identified studies was too small to provide sufficient statistical power for a meta-analytic review. A narrative synthesis was conducted. Studies were evaluated using the Joanna Briggs Institute (JBI) tools: 13-item (RCTs), 9-item (quasi-experimental), and 11-item (cohort). Two reviewers assessed quality; discrepancies were resolved by a third. Although quality was not used as an exclusion criterion due to the limited number of identified studies, JBI scores (refer to Appendix 2) were used to inform the interpretation and weighting of findings in the narrative synthesis.
Results
Study selection
From 1,746 records, 926 remained after de-duplication. Title/abstract screening yielded 25 full-texts; 9 studies met inclusion criteria [21–29]. No additional studies were identified through citation chaining and hand-searching. (Fig. 1)
Fig. 1PRISMA flow diagram
Quality assessment
Of the nine studies, methodological quality varied considerably. While one quasi-experimental study [28] achieved the maximum JBI score, indicating strong internal validity, others—particularly feasibility and pilot RCTs—scored lower due to limitations such as lack of blinding, small sample sizes, and short follow-up durations. Studies employing cognitive dissonance based interventions generally demonstrated higher methodological rigor, supporting the robustness of their findings on ED symptoms. The absence of blinding, particularly in psychoeducation and self-compassion interventions, raised concerns about bias. Full detail has been tabulated in Appendix 2.
Characteristics of included studies
Study design
Among the nine studies (Table 1): five were RCTs [22–26], two quasi-experimental [21, 28] and two were cohort studies [27, 29]. Three RCTs were feasibility trials. Studies were geographically diverse, with two conducted in Oceania [22, 28], four in North America [21, 25–27], two in Europe [24, 29], and one as a multinational collaboration between Europe and North America [23].
Recruitment strategies included social media, third-sector organizations (e.g. diabetes associations) and diabetes clinics.
Sample characteristics
Most studies recruited females with only one study including both sexes [22]. Age ranges varied considerably (reported individually in Table 1) with only four studies aimed at those less than 14 years [22, 24, 25, 28]. Sample sizes ranged from 14 to 293 with five studies having under 50 participants. Four studies incorporated family or carer involvement [24, 25, 27, 28] though conclusions are limited due to small sample size and age variability. Five out of the nine studies reported on ethnicity. Participants were predominantly ‘white,’ ranging between 59% [27] to 90% [24], and averaging 75% across the studies. No comparison of study outcome measures was reported based on ethnicity.
Interventions
Four studies used psychoeducation (resilience, body acceptance, media literacy, perfectionism, or self-esteem) [21, 24, 25, 28]; one used a self-compassion program [22] and four used cognitive dissonance based programs [23, 26, 27, 29]. The latter intervention is designed to create cognitive dissonance to reduce a key attitudinal risk factor (pursuit of the thin-ideal), which increases the risk for an ED. The cognitive dissonance based program was adapted for people with T1D from the Body Project program, an efficacious ED prevention program for the general population [30, 31]. Three of these studies used the Diabetes Body Project for ages 14–35 [23, 26, 29] and one used the Body Project T1D for adolescents aged 15–18 with caregiver sessions [27]. Five interventions were virtual [23, 24, 26, 27, 29], four in-person [21, 22, 25, 28]; none were delivered individually. Delivery mode effectiveness was inconclusive due to heterogeneity. Controls included usual care [22, 24, 25] or active educational video content [23, 26].
Drop-out rates measured from consent/randomization to follow-up, ranged from 0 to 40%. Higher retention was seen in studies with younger participants, parental involvement, and shorter durations, although this was inconsistent across studies. No pattern was found by intervention type.
Finally, three studies incorporated peer facilitators with T1D [23, 26, 29]. All three reported statistically significant improvements in ED-related symptoms and risk. However, as each also employed cognitive dissonance based methods, it is difficult to disentangle the independent effects of peer delivery from the intervention itself.
Clinical measures
Diabetes-specific ED symptoms
Diabetes-specific ED symptoms were primarily assessed using the Diabetes Eating Problem Survey-Revised (DEPS-R), a validated 16-item questionnaire used widely in clinical and research settings [32, 33]. It assesses general and diabetes-specific disordered eating behaviors including weight loss, dietary restriction, insulin omission, and vomiting.
Six studies included in this review utilised the DEPS-R. Four of the six studies, employed cognitive dissonance based interventions, and reported improvements; two showed significantly lower mean DEPS-R scores in intervention groups compared to controls: d = -0.7 [23] and d = -0.74 [26], another reported a significant reduction within-group at 6-month follow-up (d = -0.7) [29], and the fourth using the Body Project T1D showed a within-group improvement at 3-month follow-up (d = -0.49) [27]. The remaining studies did not report any statistical inferences [22, 24].
Body dissatisfaction
Body dissatisfaction is a well-established risk factor for EDs and was assessed with the Eating Disorder Inventory (EDI) with its body dissatisfaction subscale, the Body Dissatisfaction Scale (BD), the Satisfaction and Dissatisfaction with Body Parts Scale (BPS) [34], and the Screen for Early Eating Disorder Signs (SEEDS). Five studies employed one or more of these instruments [23, 25–27, 29]. All reported improvements in body dissatisfaction at follow-up. Four of these studies used cognitive dissonance based interventions [23, 26, 27, 29], and one used psychoeducation [25]. Improvements were consistent across all studies measuring this outcome, with effect sizes ranging from moderate d = -0.59 [27] to large d = -0.76 [29] for within-group effects, and from d = -0.46 [23] to d = -0.59 [26] for between-group differences.
Diabetes distress
Diabetes distress was assessed in six studies using validated tools, including Problem Areas in Diabetes (PAID: age-appropriate versions) [22, 23, 27, 29], , PAID-PR (parent-version) [24] and Diabetes Distress Scale (DDS) [26]. Cognitive dissonance based programs showed small to moderate improvements between-groups (e.g., Diabetes Body Project: d=-0.42 post-intervention [23]; d=-0.17 at 3-month follow-up [26]). Within-group improvements were also observed at 3-months (d=-0.49) [27] and 6-months (d=-0.84) [29]. No change was noted in parent-reported diabetes distress following a psychoeducation program (d=-0.07) [24] and one study found a non-significant increase in distress following a self-compassion program (mean change = + 2.0, SD = 7.9) [22].
Depressive symptoms
Depressive symptoms were assessed in three studies using interventions of psychoeducation programs [21, 28] and the Diabetes Body Project [26]. While some improvements were observed in depressive symptoms, these were generally modest and not statistically significant.
Glycemic measures
Glycemic outcomes included HbA1c and time-in-range (TIR). In three studies, follow-up durations were less than three months [21, 22, 28], making HbA1c outcomes unreliable due to the timeframe required to observe clinically meaningful changes. Among the remaining studies that reported post-intervention glycemic outcomes, none demonstrated significant improvements in HbA1c [25, 27] or TIR [23, 26].
Table 1. Characteristics of the studiesAuthor/ year/ countryStudy design and aimRecruitmentSample characteristicsInterventionFollow-up periodClinical measuresMajor findingsStudy strengths and study limitationsAlloway et al.,2001 [21]CanadaQuasi-experimentalAim:Evaluate efficacy of 6-week psychoeducation program on the primary outcomes of metabolic control, ED symptomatology, general psychopathology and diabetes treatment adherence.Community and diabetes clinic.Female age 20+Subclinical DE (based on EDI and EAT scores)Exclusion: self-reported bingeing with any compensatory behavior twice a week for 3-months, or BMI < 20.N = 14I: n = 8, age 32.5 (9.3)C: n = 6, age 31 (10.3)Psychoeducation:-Education on ED-Normal eating and healthy body weight-Assertiveness, stress management and self-esteem-Media influence, perfectionism and body image6x weeklyGroup sessionsIn-personFacilitator: dietitianWaitlist control1-month(both groups)6-month(treatment group only)BDIBSIEATEDIInsulin omissionRSESHbA1c (%)fructosamineNo statistically significant effect of intervention on any outcomes.Between-group effects at1-month follow-up:BDI: MD = -15.7BSI: MD = -0.8EAT: MD = -13.2EDI: MD = -1.1Insulin omission: MD = -1RSES: MD = -5.8HbA1c: MD = -0.1%Limitations:Small sample sizeSelf-selection biasOlder participants (average age 31.9)Short follow-upParticipants non-blinded.Control group had significantly greater general emotional distress (BSI) at baseline (p = 0.009)Strengths:14/14 completed (0% drop-out at 1-month).Boggiss et al., 2020 [22]New ZealandRCT(feasibility),although results are reported as single-group pre-post studyAim:Assess feasibility and acceptability of a self-compassion programDiabetes clinicMale or female age 12–16Mod to high DEB on DEPS-R (no inclusion/ exclusion scores provided)N – 27 were randomizedN = 19 completed studyI: n = 11, age 14 (1.2), F = 7C: n = 8, age 13.6 (1.3), F = 3Self-compassion program “Making friends with yourself”2x weeklyGroup sessions (2.5 h per session),In-personFacilitator: clinical psychologistWaitlist control2-weekPrimary outcome:Feasibility/acceptability qualitative measuresSecondary outcome:DEPS-RPAIDPSSSCS-SFSCI-RHbA1c (%)Pre-post measures from both groups pooled and reported as within-group effectsWithin-group effects immediately post-intervention:DEPS-R:Mean change = + 0.3 (5.8 SD)PAID:Mean change = + 2.0 (7.9 SD)PSSMean change = + 0.9 (6.1 SD)SCS-SFMean change = + 0.1 (0.5 SD)SCI-RMean change = + 1.5 (8.4 SD)HbA1c:Mean change = -0.2%Limitations:Small sample sizeLow attendance: ~ 50% attended both sessions.Short follow-up, particularly to note any metabolic improvementNo between-group comparisons reportedStrengths:19/27 completed (30% drop-out)Hennekes et al., 2025 [23]US and EuropeRCTAim:Evaluate efficacy of Diabetes Body Project (DBP) on primary outcomes of ED symptoms and behaviors, psychological constructs and glycemia outcomesSocial media andDiabetes clinicFemale age 14–35Report body image concerns.Exclusion: ED-related hospitalization or DKAN = 293I: n = 147, age 25.2 (5.43)C: n = 146, age 24.8 (5.58)Cognitive dissonance based program Diabetes Body Project 6 x weeklyGroup sessions(1-hour per session)OnlineFacilitator: diabetes clinicians and peer educator.Active control (Educational videos)1–2 weekBDDEPS-RDEBQ-RSEDDITIISPAIDPANAST1DALTIRBetween-group effects immediately post-intervention (adjusted for pre-intervention scores and study site):BD: aMD = -0.32 (d = -0.59,p < 0.001)DEPS-R: aMD = -4.04(d = -0.7, p < 0.001)DEBQ-RS: aMD = -0.18(d = -0.32, p = 0.021)EDDI: aMD = -1.95 (d = -0.3, p = 0.026)TIIS: aMD = -0.31 (d = -0.31,p < 0.001)PAID: aMD = -4.71 (d = -0.42, p = 0.002)PANAS: back-transformed mean difference not reported(d = -0.23, p = 0.091)T1DAL: aMD = + 3.21(d = 0.39, p = 0.004)TIR: back-transformed mean difference not reported(d = -0.08, p = 0.544)Limitations:Short duration follow-upSelection bias for digitally literate (social media)Strengths:Large sample size265/293 (9.6% drop out).Jones et al., 2024 [24]UKRCT(feasibility - parent program)Aim:Evaluate feasibility, acceptability and preliminary efficacy of a psychoeducational program for parents of children with T1D on DEPS-R as the primary outcome.Diabetes care teams and 3rd sector organizationsParents with children age 11–14N = 89 parentsI: n = 44 (child’s age 8.52 +/- 3.12)C: n = 45 (child’s age 7.89 +/- 3.39)Psychoeducation:PRIORITY intervention for parents-communication around food and weight-recognizing early DE-supporting identity and independence in T1D2x weeklyGroup sessions(2-hour sessions)OnlineFacilitator: psychologistWaitlist control3-monthPrimary outcome:Parent and child reported DEPS-RSecondary outcome:CEBQ: 8 subscalesPAID-PRWEMWBSOnly baseline HbA1cBetween-group effects at3-month follow-up:Parent-reported DEPS-R:d = -0.1 (95% CI -0.63 to 0.43)Child-reported DEPS-R:d = -0.5 (95% CI -1.26 to 0.3)CEBQ: No significant effect for any of the 8 subscales except Satiety Responsiveness,d = + 0.55 (95% CI 0.01 to 1.08)PAID-PR: d = -0.07(95% CI -0.6 to 0.46)WEMWBS: d = + 0.27 (95% CI -0.27 to 0.79)Limitations:Short follow-up55/89 completed (38% dropout rate)Effect sizes not reported on original scaleStrengths:Moderate sample sizeRobust methodology with independent randomization, blinded outcome assessmentOlmstead et al., 2002 [25]CanadaRCTAim:Evaluate the effectiveness of a psychoeducational program on ED psychopathology, ED risk factors, insulin omission and glycemiaDiabetes clinicFemales age 12–20Inclusion: DE based on EDI or DSED scores.N = 85 age 16 (2.0)I: n = 50C: n = 35Psychoeducation:Didactic information on healthy eating, DE and T1D.Parent and daughters6x weeklyGroup sessions(90-minute sessions)In-personFacilitators: ED clinician and adolescent DM clinicianControl: Usual care6-monthEDE,EDI,Insulin omissionHbA1c (%)Between-group effects over 6 months of follow-up:EDE:Restraint: p = 0.004Overeating: NSEating concern: p = 0.05Shape concern: NSWeight concern: NSEDI:Drive for thinness: p = 0.03Bulimia: NSBody dissatisfaction: p = 0.008Insulin omission days: NSHbA1c: NSLimitations:6% (n = 3) drop-out in psychoeducation arm, 31.4% (n = 11) in usual careStrength:Moderate sample sizeStice et al., 2023 [26]USARCT (pilot)Aim:Evaluate whether Diabetes Body Project can reduce ED risk factor and symptoms, diabetes distress and improve quality of life.Social media/emailFemales age 15–30Report body image concerns.Exclusion: ED-related hospitalization or DKAN = 55I: n = 30; age 23.5 (3.83)C: n = 25; age 22.06 (4.66)Cognitive dissonance based program Diabetes Body Project 6x weeklyGroup sessions(1-hour per session)OnlineFacilitators: diabetes clinician and peer educator.Active control (Educational video)3-monthBD,DDSDEPS-R,EDDI,TII,WHO-5TIR (where available)Between-group effects at 3-month follow-up (adjusted for pre-intervention scores):BD: aMD = -0.24, d = -0.35,p = 0.121DDS: aMD = -0.18, d = -0.17,p = 0.336DEPS-R: aMD = -5.6,d = -0.58, p = 0.002EDDI: aMD = -0.72, d = -0.46, p = 0.013TII: aMD = -0.21, d = -0.31,p = 0.116WHO-5: aMD = + 0.46, d = 0.46, p = 0.038TIR: aMD = + 0.05, d = 0.26,p = 0.126Limitations:Limited power of pilot studyShort follow-up.No HbA1c measureStrength:Moderate sample size.Trojanowski et al., 2022 [27]USALongitudinal cohort (feasibility)Aim:Evaluate feasibility, acceptability and preliminary efficacy of Body Project T1D on ED risk factor and symptoms, diabetes distress and quality of lifeDiabetes clinicFemales age 15–18N = 35, age 16.2 (1.12)Exclusion: active ED diagnosis noted by medical staff.Cognitive dissonance based program Body Project T1D. Caregiver session4x weeklyGroup sessions(60–90 min sessions)OnlineFacilitators: 2x psychologists3-monthDEPS-R,SEEDS,DREBQ,SATAQ-4,PAID-T,DAS,PedsQLWithin-group effects at 3-month follow-up:DEPS-R: MD = -4.06, d = -0.49 (-0.81, -0.19)SEEDS: MD = -7.43, d = -0.58 (-0.85, -0.32)DREBQ: MD = -0.49, d = -0.60 (-0.95, -0.25)PAID-T: MD = -28.58,d = -0.49 (-1.50, -0.80)SATAQ-4 (thin/low body fat subscale) = -0.65, d = -0.58 (-0.23, -0.85)DAS: MD = -5.24, d = -0.73(-1.06, -0.36)PedsQL: MD = -4.66, d = -0.42 (-0.74, -0.04)Limitations:Cohort study.No controlsSmall sample sizeStrength:Minimal drop-out rateWilksch et al., 2013 [28]AustraliaQuasi-experimentalAim:Evaluate the effectiveness of a psychoeducation program that enhances protective factors for ED.Diabetes clinic.Females age 10–12N = 20, age 11.06 (0.64)Psychoeducation: program targeting perfectionism, media literacy and self-esteem2x weeklyGroup sessions(4-hour session),Parents invited to separate sessionsFacilitator: psychologist and diabetes nurse educator4-week control period, followed by intervention1-monthPrimary outcome:CDI-SF,BES-C,DRFQMPS,SATAQ-3,SEDS,RSESSecondary outcome:HbA1c (%)Within-group effects at 1 month follow-up (adjusted for pre-intervention scores):CDI-SF: Not reportedBES-C: aMD = + 0.13, d = 0.32DRFQ: Not reportedMPS: aMD = -0.35, d = -0.65SATAQ-3: aMD = -0.46, d = -0.4SEDS: aMD = + 0.34, d = 0.56RSES: aMD = + 0.31, d = 0.57HbA1c: aMD = + 0.11%, d = + 0.13, not significant.Limitations:Small sample sizeShort follow-up periodStrengths:0% dropoutWisting et al., 2024 [29]NorwayLongitudinal cohort (pilot)Aim:Evaluate within -subject changes in ED risk factors and symptoms in those who received the Diabetes Body Project program.Social media, diabetes organizationFemale age 16–35Report body image concerns.Exclusion: ED-related hospitalization or DKAN = 24; age 25.62 (3.95)Cognitive dissonance based program Diabetes Body Project 6x weeklyGroup sessions(1-hour per session)OnlineFacilitator: diabetes clinicians and peer educator.6-monthPrimary outcomes:IBSS-R,BPS,DEPS-R,PANAS-X,DRES.Secondary outcomes:BIPQPAID,SATAQ-4R,SCSHbA1c (%): self-reportedWithin-group effects at 6-month follow-up:IBSS-R: Mean change = -0.23 (95% CI -0.43 to -0.03), d = -0.43BPS: Mean change = -0.45 (95% CI -0.66 to -0.25),d = -0.76DEPS-R: Mean change = -5.24 (95% CI -7.6 to -2.9), d = -0.70PANAS-X: Mean change = -5.3 (95% CI -10.5 to -0.07),d = -0.38DRES: Mean change = -0.46 (95% CI -0.71 to -0.2), d = -0.55BIPQ: Mean change = -3.7 (95% CI -6.05 to -1.35),d = -0.56PAID: Mean change = -10.1 (95% CI -14.9 to -5.3), d = -0.84SATAQ-4R: Mean change =-11.2 (95% CI -16.9 to -5.4),d = -0.60SCS: Mean change = + 3.2 (95% CI -1.3 to + 7.7), d = + 0.27HbA1c (%): Mean change = -0.57% (95% CI -0.31% to + 0.20%), d = -0.13.The Cohen’s d values presented here have been recalculated from original data using Eq. 2.3.5 of Cohen [35], to facilitate comparison with other studies.Limitations:Cohort studySmall sample sizeDropout rate 31.4%aMD: Adjusted Mean Difference, BD: Body Dissatisfaction, BDI: Beck Depression Inventory, BES-C: Body-Esteem Scale for Children, BIPQ: Brief Illness Perception Questionnaire, BPS: Body Parts Scale, BSI: Brief Symptom Inventory, C: Control group, CDI-SF: Children’s Depression Inventory - Short Form, CEBQ: Child Eating Behavior Questionnaire, d: Cohen’s d, DAS: Diabetes Acceptance Scale, DDS: Diabetes Distress Scale, DEBQ-RS: Dutch Eating Behavior Questionnaire - Restrained Eating Scale, DEPS-R: Diabetes Eating Problem Survey – Revised, DREBQ: Dutch Restrained Eating Behaviors Questionnaire, DRES: Diabetes-Related Eating Symptoms, DRFQ: Diabetes Family Responsibility Questionnaire, DSED: Diagnostic Survey for Eating Disorders, EAT: Eating Attitudes Test, EDDI: Eating Disorder Diagnostic Interview, EDE: Eating Disorder Examination, EDE-QS: Eating Disorder Examination Questionnaire - Short, EDI: Eating Disorder Inventory, F: Female, GAD-7: Generalized Anxiety Disorder-7, I: Intervention group, IBSS-R: Ideal-Body Stereotype Scale - Revised, MD: Mean Difference, MPS: Multidimensional Perfectionism Scale, PAID: Problem Areas in Diabetes, PAID-PR: Problem Areas in Diabetes - Parent Revised, PAID-T: Problem Areas in Diabetes - Teen, PANAS: Positive and Negative Affect Schedule, PANAS-X: Positive and Negative Affect Schedule - Revised, Parental Self-Efficacy for Diabetes, PedsQL: Pediatric Quality of Life - Core Scales, PHQ-9: Patient Health Questionnaire-9, PSS: Perceived Stress Scale, RSES: Rosenberg Self-Esteem Scale, SATAQ-3: Sociocultural Attitudes Toward Appearance Questionnaire, 3rd edition, SATAQ-4: Sociocultural Attitudes Toward Appearance Questionnaire, 4th edition, SATAQ-4R: Sociocultural Attitudes Toward Appearance Questionnaire, 4th edition Revised, SCI-R: Self-Care Inventory - Revised, SCS: Social Comparison Scale, SCS-SF: Self-Compassion Scale - Short Form, SEDS: Self-Efficacy for Diabetes Scale, SEEDS: Screen for Early Eating Disorder Signs, T1DAL: Type 1 Diabetes and Life, TIIS / TII: Thin-Ideal Internalization Scale, WEMWBS: Warwick Edinburgh Mental Wellbeing Scale, WHO-5: World Health Organization Well-Being Index
Discussion
This systematic review evaluated the feasibility and efficacy of interventions aimed at preventing ED in individuals with T1D and improving glycemia. The heterogeneity in methodological quality, as assessed using JBI tools, underscores the need for cautious interpretation of findings.
Most studies employed DEPS-R to assess change in diabetes-specific ED symptomatology. Cognitive dissonance based interventions reported statistically and clinically significantly lower mean DEPS-R scores in the intervention group, both between-groups and within-groups. These results underscore the potential of cognitive dissonance based techniques to reduce maladaptive eating behaviors and cognitions in T1D, putatively by reducing valuation of the thin-ideal. Due to overlapping variables—such as peer-facilitation in Diabetes Body Project or caregiver involvement in Body Project T1D which could potentially influence outcomes—causality remains unclear. Nonetheless, these results are promising.
Five studies assessed body dissatisfaction using the Eating Disorder Inventory (EDI), the Body Dissatisfaction Scale (BD), the Satisfaction and Dissatisfaction with Body Parts Scale (BPS) or the Screen for Early Eating Disorder Signs (SEEDS). Improvements were consistent across all studies measuring this outcome, with moderate to large effect sizes for within-group effects, and small to medium effect sizes for between-group effects when compared to a control group. Four of these five studies also utilised cognitive dissonance based approaches, reinforcing their value in addressing and enhancing body acceptance.
Cognitive dissonance based interventions also demonstrated moderate to large reductions in diabetes distress, with effects strengthening over time. In contrast, psychoeducation and self-compassion programs showed no improvements, though these studies were likely limited by study design and sample size. Symptoms of depression outcomes showed modest, non-significant improvements across interventions, suggesting that while some psychological benefits may occur, targeted strategies and longer follow-up are needed to meaningfully impact depressive symptoms in this population.
Metabolic outcomes such as HbA1c and time-in-range (TIR) were largely unaffected by the interventions. In four studies, the follow-up duration was less than three months, rendering HbA1c changes physiologically implausible and uninterpretable. In the remaining studies with follow-ups up to 6-months, no intervention demonstrated statistically significant improvements in glycemia. This suggests that while psychological interventions may successfully address cognitive and behavioral precursors to EDs, they do not directly improve metabolic outcomes in the short term. This is unexpected as there is a correlation between ED-T1D and insulin omission, suboptimal glycemic outcome, recurrent DKA and consequent diabetes-related complications [12, 35]. Insulin administration is the most potent influence on glycemia management. Whilst the DEPS-R incorporates a question on insulin omission, scoring of the tool does not specifically focus on this compensatory behavior. Future studies should analyse insulin omission separately, to gain further insight as to whether interventions are targeting this aspect of ED “purging” behavior which directly influences glycemic outcomes.
The integration of peer facilitators with lived experience of T1D was another notable feature of successful programs. Peer-led interventions appeared more relatable and may have enhanced outcomes, particularly in the adolescent and young adult populations. However, the overlap between peer delivery and cognitive dissonance content makes it difficult to disentangle the relative contributions of each component to the observed effects. Nonetheless, this combination appears to offer a promising model for future interventions.
Furthermore, family involvement—present in four studies—was associated with improved retention, particularly in younger populations. For instance, a paediatric intervention with concurrent parent sessions reported 0% drop-out [28]. However, inconsistency in participant age ranges, intervention formats and outcome reporting make it difficult to isolate and assess the specific impact of caregiver involvement on ED risk reduction in these four studies. Without consistent measurement of family dynamics or stratification by developmental stage, the role of caregiver participation in modifying ED risk remains unclear.
Overall, the cognitive dissonance based interventions appear promising in preventing ED in those with T1D. However, given that the onset of ED symptoms occur from age 14 (some would argue even younger), this program requires adaptation and evaluation in the paediatric space.
This systematic review applied rigorous standards in accordance with PRISMA 2020 and was prospectively registered on PROSPERO, which enhanced transparency and methodological accountability. A broad and inclusive search strategy, with the initial inclusion of both DE and established ED, across multiple databases, with citation chaining and hand searches for peer-reviewed papers, maximized the likelihood of capturing relevant studies. A major methodological strength was the dual-review process with conflict resolution and data extraction conducted independently by multiple reviewers, with the involvement of a biostatistician to ensure analytical clarity. This reduced risk of bias in study selection and data synthesis.
However, several limitations should be noted. First, the decision not to conduct a meta-analysis—whilst justified due to heterogeneity, as well as the relatively small number of studies —limits the ability to quantify overall intervention effects. Second, the exclusion of non-English studies may have geographically concentrated the locations to North America, Europe, and Oceania, with no representation from Asia, Africa, or South America. This exclusion and the fact that study participants were predominantly of European descent, limits the generalizability of findings to non-Western populations, especially considering cultural differences in body ideals.
The predominance of female participants is reflective of ED epidemiology but leaves male populations underrepresented, limiting gender-based conclusions. Recruitment through social media and healthcare settings may also bias the sample toward individuals with better access to resources and higher health literacy.
Most of the studies had small samples and high dropout rates (20–40%). This weakens statistical power as well as raises concerns about selection bias. These challenges highlight important considerations for future research. Interventions may benefit from being brief, co-designed with participants to improve acceptability, incorporating flexible delivery formats (e.g., digital or hybrid models), and including motivational or family-based components to support ongoing engagement. Embedding retention strategies, such as reminders, incentives, or tailored content may also help reduce dropout and improve study feasibility.
Finally, while all included studies utilised validated clinical tools, the diversity in outcome selection, duration of follow-up, and absence of standardised behavioral metrics complicates cross-study comparisons. Most follow-up periods were under six months, restricting conclusions about the long-term sustainability of intervention effects.
Conclusion
In summary, this review suggests that structured psychological interventions—particularly those using cognitive dissonance based strategies—may reduce key ED risk factors and ED pathology in people with T1D. Improvements were most notable in diabetes-specific ED symptomatology and body dissatisfaction, while glycemic outcomes remained unchanged. Though limited by sample size, heterogeneity, and geographic scope, this review provides valuable insight into the potential of preventive strategies. Future research should focus on larger, more diverse samples, younger age groups, longer follow-up durations, and integration of both psychological and metabolic outcomes to better understand the sustained impact of these interventions across global T1D populations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1National Institute for Health and Care Excellence. Type 1 diabetes in adults: diagnosis and management (NICE Guideline NG 17). 2022. Available from: https://www.nice.org.uk/guidance/ng 1732017485 · pubmed ↗
- 2Fitzgerald K, Jones C, Partridge H, Rouse L, Satherley RM. Exploring healthcare professionals’ attitudes to screening for disordered eating in type 1 diabetes. Diabet Med. 2025;e 70003. 10.1111/dme.70003.10.1111/dme.70003 PMC 1200656239948754 · doi ↗ · pubmed ↗