Characteristics of indeterminate QuantiFERON-TB Gold PLUS results in pediatric lupus nephritis at Beijing Children’s Hospital, 2023–2024
Yue Xi, Huiwen Zheng, Yonghong Wang, Yajie Guo, Jing Xiao, Feina Li, Hui Qi, Weiwei Jiao, Nan Zhou, Zhi Chen, Lin Sun

TL;DR
This study finds that nearly half of children with lupus nephritis had unclear tuberculosis test results, likely due to immunotherapy and high triglycerides.
Contribution
The study identifies immunotherapy use and elevated triglycerides as novel predictors of indeterminate QFT-Plus results in pediatric lupus nephritis patients.
Findings
44.14% of pediatric lupus nephritis patients had indeterminate QFT-Plus results, mostly due to positive control failure.
Immunotherapy use and high triglyceride levels were independently associated with indeterminate test outcomes.
A triglyceride level of 2.155 mmol/L had a 75.1% accuracy in predicting indeterminate results.
Abstract
Tuberculosis screening in pediatric lupus nephritis (LN) patients presents unique diagnostic challenges. This study aimed to analyze the frequency of indeterminate QuantiFERON-TB Gold Plus (QFT-Plus) results among children with LN and the potential influence factors. A retrospective cohort study was conducted among patients under 18 years old with a confirmed diagnosis of LN screened for tuberculosis infection from January 2023 and August 2024. Demographic and clinical data were extracted from their electronic medical record, with categorical variables presented as frequencies and continuous variables as medians. Using SPSS 18.0 (Chicago, IL), we first performed univariate logistic regression to identify factors associated with indeterminate IFN-γ results (P < 0.05), then entered significant variables into multivariate models to determine independent predictors, reporting results as…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
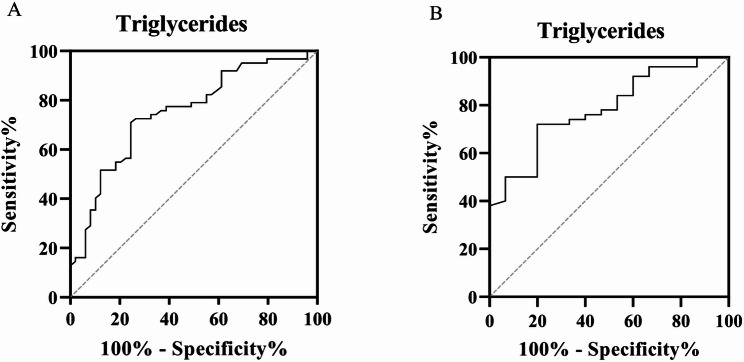 Figure 1
Figure 1- —Beijing Municipal Science & Technology Commission Proof of Concept Center
- —https://doi.org/10.13039/501100001809National Natural Science Foundation of China
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSystemic Lupus Erythematosus Research · Cytomegalovirus and herpesvirus research · Tuberculosis Research and Epidemiology
Introduction
Tuberculosis (TB), a leading infectious cause of death globally, latently infects approximately one-quarter of the world’s population, of whom 10% will progress to active TB disease during their lifetime [1, 2]. The risk of reactivation from latent TB infection (LTBI), defined as Mycobacterium tuberculosis (MTB) infection without active symptoms, is substantially higher in infants (30%-40%) and children (10%-20%) than in adults [3]. Thus, early detection and initiation preventive treatment of LTBI are critical priorities for pediatric TB control.
Given the elevated risk of reactivation, comprehensive LTBI screening is widely recommended and represents a key standard of care for patients prior to initiating treatment with corticosteroids, immunosuppressants, or biologic agents [4–8]. This is particularly critical for patients with systemic lupus erythematosus (SLE), a multisystem autoimmune disorder characterized by immune dysregulation and pathogenic autoantibody production [9, 10]. Among the most severe clinical manifestations of SLE, lupus nephritis (LN) exhibits both higher prevalence and greater severity in pediatric populations compared to adults [11, 12]. Moreover, the aggressive immunosuppressive therapies in this population highlight the importance of implementing comprehensive screening for LTBI before pre-treatment, which can substantially reduce active TB incidence.
Current diagnostic approaches for pediatric LTBI screening rely on the tuberculin skin test (TST) and interferon-gamma release assays (IGRAs) [13–15]. The IGRA assay is an in vitro blood test that measures IFN-γ production by T cells following stimulation with MTB-specific antigens, which are unaffected by BCG vaccination status or most nontuberculous mycobacterial exposures [16]. The fourth-generation QuantiFERON-TB Gold Plus (QFT-Plus) IGRA assay utilizes an enzyme-linked immunosorbent assay (ELISA) platform featuring four distinct tubes: a negative-control (nil) tube for background IFN-γ quantification, a positive-control (mitogen) tube containing nonspecific T-cell stimulants to assess immune competence, and two antigen tubes (TB1 and TB2) incorporating novel CD8 + T-cell stimulating peptides to enhance detection sensitivity for MTB infection [17, 18]. Despite these technological advances, a significant limitation of IGRA persists in the form of indeterminate results, which occur more frequently in pediatric populations than adults, comprising accurate diagnosis of MTB infection [19]. While existing evidence indicates QFT-Plus generates fewer indeterminate results compared to its predecessor, QuantiFERON-TB Gold In-Tube (QFT-GIT), in pediatric populations [20, 21], the frequency of indeterminate results among children with LN and the potential influence of associated clinical and laboratory parameters remain poorly characterized. To address this knowledge gap, this study aims to analyze factors associated with indeterminate QFT-Plus results in pediatric LN patients, which may help optimize the timing of TB screening in patients requiring immunosuppressive therapy.
Methods
Participants
This retrospective study was performed at the Nephrology Department, Beijing Children’s Hospital, between January 2023 and August 2024. Eligible participants were under 18 years of age, with a confirmed diagnosis of LN based on clinical, endoscopic, radiographic, or histopathological criteria, and who had complete QFT-Plus test results and clinical data available. Patients with non-lupus nephritis-related kidney disorders (e.g., primary nephrotic syndrome, diabetic nephropathy) were excluded. Patients with incomplete clinical data, improper sample handling (e.g., delayed testing > 16 h), hemolysis or coagulation abnormalities affecting QFT-Plus results were also excluded.
Analysis of clinical and laboratory characteristics
Clinical data included age, sex, disease duration, comorbid conditions, hospitalization frequency, medications and complications. Laboratory data included complete blood count: white blood cells (WBC), red blood cells (RBC), hemoglobin (Hb), platelets (PLT), neutrophils, lymphocytes, monocytes; blood biochemistry: albumin, C-reactive protein (CRP), albumin/globulin ratio (A/G ratio), urea, creatinine, total cholesterol, uric acid, alkaline phosphatase (ALP), aspartate aminotransferase (AST)/alanine aminotransferase (ALT), total bilirubin, cholinesterase, lactate dehydrogenase (LDH), triglycerides; erythrocyte sedimentation rate (ESR); coagulation: prothrombin time (PT), fibrinogen, thrombin time (TT), activated partial thromboplastin time (APTT), D-dimer, antithrombin III activity (AT-III); complement system: complement 3 (C3), complement 4 (C4); early kidney injury biomarkers: urinary IgG, urinary microalbumin, urinary transferrin, urinary α1-microglobulin, urinary β2-microglobulin, N-acetyl-β-D-glucosaminidase (NAG).Data were categorized by QFT-Plus results, with subsequent comparison of clinical and laboratory findings between determinate and indeterminate test result groups. For CRP, values below 10 mg/L are considered normal, while values equal to or above 10 mg/L are considered abnormal. The immunotherapy consisted of immunoglobulin (IVIg) or/and immunosuppressor or/and corticosteroids. Disease severity was assessed using the Systemic Lupus Erythematosus Disease Activity Index – Responder (SLEDAI-R) [22].
QFT-plus assay
Following the manufacturer’s protocol, venous blood (3 mL) was collected into lithium heparin tubes and aliquoted into four separate QFT-Plus tubes. The tubes were incubated at 37 °C for 16–24 h, followed by centrifugation at 2000 × g for 15 min to harvest supernatants for IFN-γ quantification (IU/mL) via ELISA. IFN-γ levels in the antigen tubes that >10 IU/ml were classified as 10 IU/mL. Positive results were defined as either IFN-γ values of TB1-nil or TB2-nil ≥ 0.35 IU/mL, and ≥ 25% of the nil value; and negative when they were < 0.35 IU/mL. Nil value of >8.0 IU/mL and /or a mitogen minus nil tube value of <0.5 IU/mL were considered indeterminate. Positive and negative results were categorized as “determinate”.
Statistical analysis
Categorical variables were expressed as frequencies and percentages, while continuous variables were presented as median and interquartile range (IQR). Univariate logistic regression analysis for all candidate variables were performed to identify factors associated with indeterminate IFN-γ results. Least Absolute Shrinkage and Selection Operator (LASSO) regression was employed for variable selection to effectively mitigate the risk of model overfitting. Additionally, non-collinear variables showing a significant association (P < 0.1), as well as clinically relevant predictors, were incorporated into the final multivariate logistic regression analysis. Results were reported as odds ratios (ORs) with corresponding 95% confidence intervals (CIs). All statistical analyses were performed using SPSS version 18.0 software (SPSS, Chicago, IL, USA).
Results
Patient characteristics
A total of 111 patients with LN underwent QFT-Plus testing were enrolled from 2023 to 2024, consisting of 2 (1.80%) positive, 60 (54.04%) negative and 49 (44.14%) indeterminate results. The median age of the study participants was 13 years and the majority were female (81.08%). The median frequency of hospitalization was 10 times. Regarding the 49 indeterminate results, 43 (87.76%) were due to positive control failure, one (2.04%) due to negative control failure, and five (10.20%) due to both positive control and negative control failure. In the 30-day period prior to the QFT-Plus test, 46 (41.44%) of the study cohort were treated with immunotherapy (Table 1).
Table 1. Demographic and clinical characteristicsVariableMedian (IQR)Age (year)13 (11–14) Sex Male Female21 (18.92)90 (81.08) Laboratory findings White blood cells (10^9^/L)6.14 (3.67–8.70) Red blood cells (10^12^/L)3.70 (3.13–4.17) Hemoglobin (g/L)103 (87–120) Platelets (10^9^/L)215 (153–263) Neutrophils (10^9^/L)4.42 (2.31–6.98) Lymphocytes (10^9^/L)1.13 (0.73–1.75) Monocytes (10^9^/L)0.37 (0.23–0.55) Blood biochemistry Albumin (g/L)30.70 (26-36.30) A/G ratio1.03 (0.79–1.40) Urea (mmol/L)8.42 (4.98–13.52) Creatinine (µmol/L)59.30 (43.20-90.83) Total cholesterol (mmol/L)4.48 (4.00-6.36) Uric acid (µmol/L)375.60 (271.20-503.25) ALP (U/L)85 (66–120) AST/ALT1.50 (1–2) Total bilirubin (µmol/L)7.56 (6.07–10.25) Cholinesterase (U/L)7576 (5228–10000) LDH (U/L)238 (186–315) Triglycerides (mmol/L)2.12 (1.69–3.32) Coagulation Prothrombin time (second)10.90 (10.20-11.59) Fibrinogen (g/L)2.94 (2.21–3.41) Thrombin time (second)17.30 (15.90–19.40) APTT (second)31.30 (27.10–35.60) D-dimer (mg/L)0.46 (0.19–0.82) Antithrombin III activity (%)112 (96–122) Complement system Complement 3 (g/L)0.38 (0.24–0.57) Complement 4 (g/L)0.06 (0.03–0.12) Early kidney injury biomarkers Urinary IgG (mg/L)106 (23.38-283.25) Urinary microalbumin (mg/L)804 (57.30–2360) Urinary transferrin (mg/L)88.90 (31.30–231) Urinary α1-microglobulin (mg/L)37.20 (18.55–94.65) Urinary β2-microglobulin (µg/L)510 (152.75-2666.25) NAG (U/L)21.45 (11.48–35.28) Erythrocyte sedimentation rate (mm/h) 27 (12.50–61.50) Hospitalization frequency 10 (3–15) SLEDAI-R 13 (8–17) N (%)
Co-morbidity Respiratory disease50 (45.05) Cardiovascular disease80 (72.07) Hepatic disease29 (26.13) Nephropathy30 (27.03) Other autoimmune disorder26 (23.42) Multi-system disease99 (89.19) None12 (10.81) Immunotherapy Yes46 (41.44) No65 (58.56) C-Reactive Protein Abnormal9 (8.11) Normal102 (91.89) QFT-Plus Positive2 (1.80) Negative60 (54.05) Indeterminate49 (44.14)A/G: albumin/globulin ratio; ALP: alkaline phosphatase; AST/ALT: aspartate aminotransferase /alanine aminotransferase; LDH: lactate dehydrogenase; APTT: activated partial thromboplastin time; NAG: N-acetyl-β-D-glucosaminidase; SLEDAI-R: Systemic Lupus Erythematosus Disease Activity Index – Responder
Univariate analysis of factors influencing indeterminate QFT-Plus results
Univariable logistic regression analysis indicated that the indeterminate group had significantly lower levels of hemoglobin, albumin, and ALP, fewer hospitalizations, and more frequent use of immunotherapy compared to the determinate group. In contrast, triglyceride and D-dimer levels were significantly elevated in the indeterminate group (Table 2).
Table 2. Univariate analyses of association with indeterminate QFT-Plus testVariableDeterminate(n = 62)Indeterminate(n = 49)Odds Ratio(95% CI)P valueMedian (IQR)Median (IQR)Age13 (11–14)13 (11–14)1.054(0.907–1.226)0.491Male sex12 (19.35)9 (18.37)0.938(0.359–2.446)0.895 Laboratory findings White blood cells (10^9^/L)6.35(4.65–8.17)4.90(3.27–9.55)0.958(0.859–1.069)0.441 Hemoglobin (g/L)115(94.75–126)95(77-105.50)0.968(0.950–0.987)0.001 Lymphocytes (10^9^/L)1.34(0.78–1.96)1.07(0.71–1.44)0.705(0.437–1.138)0.152 Blood biochemistry Albumin (g/L)34.40(28.28–39.83)29.10(24.30-30.75)0.866(0.809–0.927)<0.001 Creatinine (µmol/L)50.10 (42.20–78)69.90(45.85-108.35)1.001(0.996–1.005)0.784 ALP (U/L)90.50(70.75-145.24)81 (60.50–111)0.988(0.98–0.997)0.011 Triglycerides (mmol/L)1.82(1.30–2.38)2.89 (2.11–3.95)1.999(1.382–2.891)<0.001 Coagulation D-dimer (mg/L)0.21 (0.10–0.49)0.72 (0.46–1.10)2.221(1.214–4.064)0.01 Complement system Complement 3 (g/L)0.43 (0.31–0.71)0.29 (0.22–0.42)0.28(0.07–1.122)0.072 Early kidney injury biomarkers Urinary microalbumin (mg/L)528 (32.95–1970)1130 (156–2920)1 (0.9999–1.0002)0.714 Erythrocyte sedimentation rate (mm/h) 23 (12-48.25)34 (20–69)1.012(0.999–1.026)0.064 Hospitalization frequency 12 (6.75-17)6 (2-12.50)0.914(0.861–0.971)0.003 SLEDAI-R 12.5 (7–18)14 (12–16)1.052(0.995–1.112)0.077 N (%)
N (%)
C-Reactive Protein Normal3 (4.84)6 (12.24)Reference Abnormal59 (95.16)43 (87.76)2.744(0.650-11.588)0.170 Immunotherapy No50 (80.65)15 (30.61)Reference Yes12 (19.35)34 (69.39)9.444(3.936–22.661)<0.0001ALP: alkaline phosphatase. SLEDAI-R: Systemic Lupus Erythematosus Disease Activity Index – Responder
Multivariate analysis of factors influencing indeterminate QFT-Plus results
The final multivariate logistic regression analysis was shown in supplementary Tables 1, and the correlation matrix was performed to assure model integrity (supplementary Table 2). Moreover, multivariable logistic regression analysis revealed that triglycerides level (OR 1.847; 95% CI 1.195–2.856; P = 0.006), and immunotherapy use (OR 12.306; 95% CI 3.937–38.463; P < 0.0001) were independently associated with increased risk of indeterminate QFT-Plus results (Table 3).
Table 3. Multivariate analysis of predictors for an indeterminate QFT-Plus resultVariableOdds Ratio95% Confidence IntervalP-valueErythrocyte sedimentation rate (mm/h)1.0070.986–1.0290.501Hemoglobin (g/L)0.9920.966–1.0180.527Albumin (g/L)0.9410.858–1.0310.192Triglycerides (mmol/L)1.8471.195–2.8560.006D-dimer (mg/L)1.8430.825–4.1160.136SLEDAI-R0.9700.892–1.0550.473Received immunotherapy12.3063.937–38.463<0.0001CRP abnormal2.1600.329–14.1900.423LN: lupus nephritis; CRP: C-reactive protein. SLEDAI-R: Systemic Lupus Erythematosus Disease Activity Index – Responder
Cut-Off values for prediction of indeterminate QFT-Plus results
ROC analysis was performed to evaluate the ability of triglyceride levels to predict indeterminate QFT-Plus results (Fig. 1; Table 4). At a cutoff value of 2.155 mmol/L, the area under the ROC curve was 0.751 (95% CI: 0.660–0.842; P < 0.0001), with a sensitivity of 70.97% and a specificity of 75.51% in all patients. Among patients who had not received immunotherapy, a cutoff of 2.210 mmol/L produced an AUC of 0.783 (95% CI: 0.663–0.904; P < 0.001), with corresponding sensitivity and specificity values of 72% and 73.33%, respectively.
Fig. 1ROC curves illustrating the ability of triglyceride levels to discriminate indeterminate QFT-Plus results in all patients (A) and in patients who had not received immunotherapy (B)
Table 4AUCs of triglycerides for discriminating indeterminate QFT-Plus results from determinate resultsVariablePopulationAUC(95% CI)P valueStd. ErrorYouden’s indexCut-off valueSensitivity (%)(95% CI)Specificity (%)(95% CI)Triglycerides (mmol/L)All patients0.751(0.660–0.842)<0.00010.04746.482.15570.97(58.71–80.78)75.51(61.91–85.40)Patients without immunotherapy0.783(0.663–0.904)<0.0010.06145.332.21072.00(58.33–82.53)73.33(48.05–89.10)
Patients with indeterminate QFT-Plus results with negative control failure
In total, six patients demonstrated indeterminate QFT-Plus results, including five cases with concurrent negative and positive control failures and one case with negative control failure. Notably, five of these patients (83.3%) were female. Laboratory investigations revealed consistent patterns of cytopenia and inflammatory activation: hemoglobin levels, serum albumin, and complement C3 levels were all subnormal, while acute-phase reactants including D-dimer and erythrocyte sedimentation rate were markedly elevated. Four patients with negative control failures were presented with concomittant hepatic dysfunction, and only one patient was naïve to immunotherapy (supplementary Table 3).
Discussion
Indeterminate QFT-Plus results were associated with significant uncertainty when making a clinical decision on whether treatment for LTBI is required. Our study identified a remarkably high prevalence of indeterminate QFT-Plus results (44.14%) in pediatric LN, substantially exceeding the 3.0% rate previously reported in rheumatic disease populations [23]. Indeterminate results may occur due to two mechanisms: failure of the positive control tube with low IFN-γ production following phytohemagglutinin stimulation, or failure of the negative control tube with elevated IFN-γ levels in the unstimulated sample. Our analysis revealed that 87.76% indeterminate cases were due to positive control failure, reflecting LN-associated immune dysregulation. Excessive exposure of autoantigens in LN induces T-cell exhaustion, impairing Th1-mediated IFN-γ production and consequently compromising test sensitivity [24]. Two thirds of patients with negative control failures presented with concurrent hepatic dysfunction, which may stem from disease-associated systemic inflammation promoting nonspecific IFN-γ secretion - a phenomenon also documented in patients with malignancies, active TB, or metabolic disorders including hypertension and diabetes [25–27]. These findings suggest that the diverse underlying disease conditions may create an internal environment conducive to aberrant IFN-γ secretion. In addition to disease activity, numerous potential factors can also affect T-cell responses through multiple mechanisms, potentially compromising the reliability of IGRAs.
We revealed that immunotherapy agent usage, which may impair T cell activation, was an independent factor associated with the indeterminate QFT-Plus results in pediatric LN patients. However, the association between immunosuppressive agents and indeterminate IGRA results remains controversial across different clinical populations. While several studies involving immunocompromised or oncology patients have demonstrated this relationship with QFT-GIT results [28–31], a large-scale investigation of 408 rheumatic disease patients failed to establish this relationship [23]. These conflicting findings reflect several key variables, including fundamental differences in the underlying pathophysiology of various diseases, substantial heterogeneity in study population characteristics, and considerable variation in immunosuppressive regimens regarding drug class, dosage intensity, and treatment duration. Such methodological and clinical diversity across studies poses significant challenges in deriving consistent conclusions on attributable to the indeterminate IGRA result.
Additionally, elevated triglyceride levels were independently associated with indeterminate QFT-Plus results in our cohort. As a component of the triglyceride-glucose index, triglyceride may modulate immune cell function and polarization, potentially leading to the type of dysregulated immune responses that could contribute to an indeterminate assay outcome [32]. The role of triglyceride in TB immunopathology, however, is complex and seemingly paradoxical. For instance, while some studies associate higher baseline levels with TB treatment failure [33], others report lower triglyceride levels in active TB patients alongside more severe inflammation [34], highlighting a multifaceted relationship. Besides, triglycerides are linked to BMI, and underweight individuals with low levels are at higher TB risk [35]. Whereas our analysis revealed that triglycerides exhibited high predictive performance in patients not receiving immunotherapy, indicating their potential utility as immunodiagnostic biomarkers for predicting indeterminate QFT-Plus outcomes. These findings could help guide clinical decisions regarding the optimal timing of QFT-Plus testing in high-risk populations.
Our study has several limitations. First, due to the diversity of immunotherapy agents and limited sample size per agent, which could introduce selection bias and unreliable estimates if analyzed separately, we consolidated the original treatment categories into a binary variable. An expanded cohort will be enrolled to enable future stratified analyses of specific drug classes, doses, and treatment durations related to indeterminate QFT-Plus results. Second, the ROC analyses for triglycerides have not been subjected to internal and external validation. Finally, given the retrospective nature of this study and lack of systematic follow-up, we are unable to report the proportion of children with indeterminate QFT-Plus results who subsequently developed active TB. Future prospective studies incorporating larger sample sizes and systematic long-term follow-up will be conducted to address these issues.
Conclusions
Hospitalized patients with LN had a high rate of an indeterminate QFT-Plus result, predominantly in positive control failure. Besides, our data showed that the use of immunotherapy agents and high triglycerides level represent factors associated with indeterminate QFT-Plus results in our cohort of pediatric lupus nephritis patients.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pennesi M, Benvenuto S. Lupus nephritis in children: novel perspectives. Medicina-Lithuania. 2023;59(10).10.3390/medicina 59101841 PMC 1060795737893559 · doi ↗ · pubmed ↗
- 2Pai M, Riley l W JM. Interferon-gamma assays in the immunodiagnosis of tuberculosis: a systematic review. lancet Infect Dis. 2004;4(12):761–776.10.1016/S 1473-3099(04)01206-X 15567126 · doi ↗ · pubmed ↗
- 3Shafeque A, Bigio J, Hogan CA, Pai M, Banaei N. Fourth-generation Quanti FERON-TB gold plus: what is the evidence? J Clin Microbiol. 2020;58(9).10.1128/JCM.01950-19PMC 744865032493779 · doi ↗ · pubmed ↗
- 4Buonsenso D, Delogu G, Perricone C, Grossi R, Careddu A, De Maio F, Palucci I, Sanguinetti M, Valentini P, Sali M. Accuracy of Quanti FERON-TB gold plus test for diagnosis of infection in children. J Clin Microbiol. 2020, 58(6).10.1128/JCM.00272-20PMC 726939732229602 · doi ↗ · pubmed ↗
- 5Ahn SS, Kim HW, Park Y. Frequency and factors of indeterminate Quanti FERON-TB gold In-Tube and Quanti FERON-TB gold PLUS test results in rheumatic diseases. J Clin Med. 2021; 10(19).10.3390/jcm 10194357 PMC 850970334640376 · doi ↗ · pubmed ↗