Association of comorbidities and socioeconomic deprivation among people who died from dementia in England between 2013 and 2023: analysis of death certificates
Sedigheh Zabihi, Michael Jackson, Elizabeth L Sampson, Sube Banerjee, Charlotte Kenten, Claudia Cooper

TL;DR
This study analyzed death certificates in England to understand the link between dementia, comorbidities, and socioeconomic factors from 2013 to 2023.
Contribution
The study reveals that people in more deprived areas had more comorbidities at death from dementia, highlighting health inequities.
Findings
Dementia was the primary cause of death for 70.2% of cases, with women and those aged 85+ being most affected.
Common comorbidities included influenza/pneumonia, heart disease, cancer, hypertension, and diabetes.
Higher socioeconomic deprivation correlated with more comorbidities, even after adjusting for age and sex.
Abstract
To describe the sociodemographic characteristics and comorbidities of people who died from dementia between 2013 and 2023 in England. We analysed death certificates reported in England from 2013 to 2023. We report the number, age, sex, country of origin and socioeconomic status of people who died with a dementia diagnosis recorded (as a primary or contributory cause); the dementia subtype diagnoses and recorded comorbidities. We tested the hypothesis that number of comorbid disorders would be higher in more deprived areas. There were 987 719 certificates in this period that recorded dementia as a cause of death, of which 693 663 (70.2%) recorded dementia as the primary cause of death. In total, 62.2% (n = 614 419) of those who died from dementia were women, 65% (n = 643 026) were aged 85+, and most (846 584, 85.7%) were born in England. Fifteen percent (n = 149 447) of included death…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
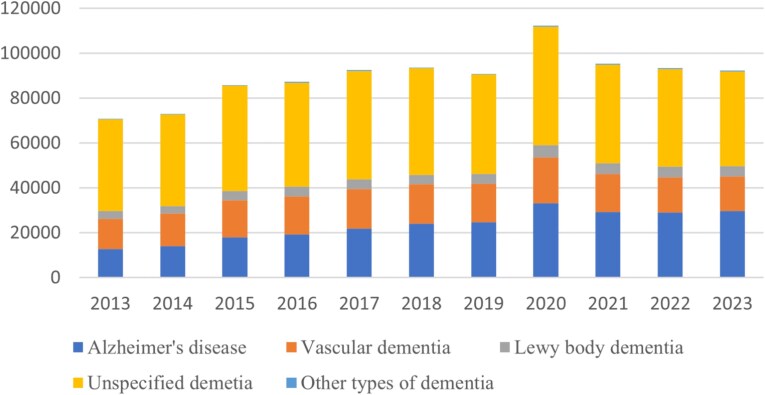 Figure 1
Figure 1| IMD quintile | Number of conditions recorded on death certificate | ||||||
|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | 5 | ≥6 | |
| 1 (most deprived) | 27 610 | 67 631 | 48 935 | 24 156 | 8807 | 2561 | 823 |
| 2 | 29 147 | 72 588 | 51 345 | 25 368 | 8850 | 2560 | 832 |
| 3 | 32 893 | 81 953 | 55 239 | 25 779 | 8858 | 2393 | 836 |
| 4 | 33 476 | 83 612 | 55 200 | 25 099 | 8520 | 2469 | 774 |
| 5 (least deprived) | 32 926 | 80 963 | 51 694 | 23 127 | 7818 | 2215 | 662 |
| Total | 156 052 | 387 747 | 262 413 | 123 529 | 42 853 | 12 198 | 3927 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPalliative Care and End-of-Life Issues · Dementia and Cognitive Impairment Research · Chronic Disease Management Strategies
Key Points
The number of deaths from dementia in England increased slightly between 2013 and 2023.Level of deprivation was associated with number of comorbidities recorded on death certificates of those who died from dementia.Policies are needed to drive higher quality care for people with multiple long-term conditions especially from deprived areas.
Introduction
Most people who die from dementia have co-existing physical and mental comorbidities, which are associated with more rapid cognitive and functional decline, and lower quality of life [1]. Providing care for this group is resource-intensive in terms of health and social care services [2]. The UK government’s 2025 health mission plans to tackle persistent inequalities in health by shortening the amount of time people spend in ill-health and earlier identification and management of chronic conditions [3]. Knowing more about the comorbidities people with dementia experience in their final years, and who is most at risk within the population could support delivery of this mission, by informing how policymakers plan and prioritise services. Death certificates are an important source of information about people who die with dementia, as they can avoid bias related to the lesser likelihood of more deprived populations taking part in research in this area [4].
The cause of death in a person with advanced dementia commonly involves pneumonia, because neurodegenerative processes diminish coughing and swallowing abilities, increasing the likelihood of aspiration and subsequent pneumonia. Such illnesses can be conceptualised as consequences of end-stage dementia. Some conditions, such as cardiovascular disease share aetiologies with dementia, which often has a vascular component. Other comorbidities such as cancers, are independent, co-occurring conditions. Acknowledging this heterogeneity, we investigated how the number of illnesses present at death in people recorded as having dementia varied with area deprivation. Building on previous work by Public Health England [5], we aimed to provide health and social care policymakers and commissioners with data on those dying from dementia. We explored conditions recorded alongside dementia on death certificates and tested the hypothesis that more conditions would be recorded at death in more deprived areas.
Methods
We analysed death certificates for people aged 18+ at the time of death, obtained from the Office for National Statistics (ONS): Public Health England Annual Mortality Extract. This dataset includes information recorded on the Medical Certificate of Cause of Death (MCCD) from civil registry records, which ONS converts to ICD-10 (International Statistical Classification of Diseases and Related Problems version 10) codes using automatic coding software [6].
We defined the primary (also termed underlying) cause of death as the disease that initiated the train of events directly linked to death; and the contributory cause of death as part of the causal sequence of events contributing to death [5]. Each death certificate includes one primary and up to 15 contributory causes. When a person with a diagnosis of dementia dies from an unrelated cause, dementia may not be listed on the death certificate. Therefore, this report does not describe the whole population who die with dementia; but it enables us to describe those for whom dementia was a cause of death—in other words who died from dementia.
We defined dementia as the presence of any ICD-10 dementia diagnostic code (Appendix 1). Comorbidity was defined as any condition recorded as a cause of death (primary or contributory) in addition to dementia. We included conditions with ≥5% occurrence in the cohort, categorised using ONS short list of cause of death [6] (Appendix 2).
We report the number of people in England who died with a dementia diagnosis recorded on their death certificate (as a primary or contributory cause) between 2013 and 2023; the dementia subtype diagnoses, year of death registration; sex; age at death; country of birth and area deprivation, using Index of Multiple Deprivation (IMD) quintiles, with quintile 1 (IMD 1–2) representing the highest socioeconomic deprivation level and quintile 5 (IMD 9–10) the lowest.
We report the proportion of deaths of people with dementia in which each common comorbidity was recorded. We conducted a multiple linear regression analysis to test our hypothesis that number of comorbid disorders was associated with area-level deprivation, after controlling for age and sex.
Results
Between 2013 and 2023, there were 987 719 deaths recorded with dementia as a cause (primary and contributory), of which 693 663 (70.2%) recorded dementia as the primary cause of death. Consistent with the previous report [5], unspecified dementia (497 416; 50%) was the most commonly recorded subtype, followed by Alzheimer’s disease (256 180; 26%) and vascular dementia (182 527; 19%). The proportion of people dying with unspecified dementia subtype increased with deprivation level, from 47.5% (n = 94 760/199405) of deaths in quintile five to 52.9% (n = 95 454/180 523) of deaths in quintile one.
Figure 1 shows the number of deaths with dementia (and subtypes) recorded as a primary or contributory cause of death, by year. The higher number of deaths from dementia in 2020 can be attributed to the COVID-19 pandemic [7].
Deaths with dementia as a primary or contributory cause (specifying subtype) by year (N = 987 719).
Of these deaths from dementia (primary or contributory), 614 419 (62.2%) were recorded in women and 373 300 (37.8%) in men. In total, 65% (n = 643 026) were aged 85+ (Appendix 3). Most were born in England (846 584; 85.7%), Scotland (22 706; 2.3%), Ireland (22 991; 2.3%), Wales (18 166; 1.8%) or India (11 630; 1.1%). These figures are similar to those reported from 2012 to 2014 [5].
Causes of death
In total, 15.1% (n = 149 447) of included death certificates recorded dementia as sole cause of death, while others recorded up to 15 comorbidities as primary or contributory causes of death (median = 1; IQR = 1–2). We conducted a multiple linear regression, with the number of comorbidities on the death certificate as the dependent variable, and deprivation levels as an independent variable, also adjusting for age and sex. The model was significant overall (R^2^ = 0.01, F(6, 987 719) =1726, P < .001). We found that death certificates of people living in areas with the least deprivation included significantly less comorbidities compared with those living in areas with the highest deprivation (β = −0.04; P < .001) (Table 1).
In cases where dementia was a contributory cause of death, most common primary causes were diseases of the circulatory (107 136; 36.4%), respiratory (31 431; 10.7%) and digestive systems (18 637; 6.3%); and cancers (54 538; 18.5%).
Where dementia was the primary cause, most commonly recorded contributory causes were: ‘senility’ (254 437; 25.7%), influenza and pneumonia (183 203; 18.5%), ischaemic heart diseases (114 871; 11.6%), cancers (107 444; 10.8%), hypertensive diseases (99 517; 10%) and diabetes (98 517; 10%).
Conclusion
A small increase in deaths from dementia from 2013 to 2023, reflects the ageing population [8], pandemic-related excess deaths [7] and increasing dementia diagnosis rates [9]. People living in more deprived areas who died from dementia had more conditions recorded on their death certificates than those who died with dementia in less deprived areas. The associations of socioeconomic deprivation and poor health including premature mortality with higher dementia risk are well established [10–12]. Our results suggest that one reason for this inequity may be the negative sequelae of living with multiple comorbidities. As the number of comorbidities increases, healthcare needs become more complex, especially in people with dementia [13].
In line with previous evidence, we found that people with dementia commonly died with cardiometabolic diseases [14, 15], long-term conditions that are implicated in the aetiology of dementia and which affect its prognosis and quality of life [16]. One in ten people dying with dementia had diabetes mellitus. This has implications for end-of-life care, as there are complexities to managing diabetes in people with dementia, including challenges with administering medication, regulating eating habits and monitoring of blood glucose [17].
One in ten people who died with dementia had cancer. People diagnosed with dementia at the same time as, or after their cancer diagnosis, are less likely to receive cancer treatment or end-of-life care appropriate to their needs [18]. Our findings highlight the need for improved understanding of the complexities of delivering appropriate care for people with long-term conditions co-existing with dementia [19]. This could help reduce care inequalities.
There are several limitations to the study. Our sample was limited to deaths where dementia was recorded as a significant contributory factor. Death certificates do not record conditions not considered causally related to death. It is less likely dementia will be recorded on death certificates completed in hospital settings. While the accuracy of death certificates as a means of recording dementia diagnosis has increased in recent years, it remains under recorded [20].
Dementia is often accompanied by other physical and mental disorders, especially towards the end of life [21]. Policies to drive higher quality care for people with multiple long-term conditions especially from deprived areas need to ensure that treatment and care, including end-of-life care is tailored to complex needs including those posed by dementia as a comorbidity. Policy shifts outlined in the UK 10-year health plan, towards more integrated, neighbourhood care [22] could reduce unhelpful boundaries between physical and mental health care, which disadvantage those living with multiple long-term conditions; as well as driving the concept of brain health and public health initiatives particularly in more deprived areas.
Supplementary Material
aa-25-1656-File002_afaf340
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bunn F, Burn AM, Goodman C et al. Comorbidity and dementia: a scoping review of the literature. BMC Med 2014;12:192. 10.1186/s 12916-014-0192-4.25358236 PMC 4229610 · doi ↗ · pubmed ↗
- 2Steinmetz JD, Seeher KM, Schiess N et al. Global, regional, and national burden of disorders affecting the nervous system, 1990–2021: a systematic analysis for the global burden of disease study 2021. The Lancet Neurol 2024;23:344–81. 10.1016/S 1474-4422(24)00038-3.38493795 PMC 10949203 · doi ↗ · pubmed ↗
- 3Prime Minister’s Office 10 Downing Street . Build an NHS Fit for the Future. 2025. https://www.gov.uk/missions/nhs (1 September 2025, date last accessed).
- 4Cooper C, Ketley D, Livingston G. Systematic review and meta-analysis to estimate potential recruitment to dementia intervention studies. Int J Geriatr Psychiatry 2014;29:515–25. 10.1002/gps.4034.24706605 · doi ↗ · pubmed ↗
- 5Public Health England . Dying with Dementia. 2016. https://assets.publishing.service.gov.uk/media/5b 6c 4b 34e 5274 a 2970 ab 5e 72/Dying_with_dementia_data_analysis_report.pdf (24 June 2024, date last accessed).
- 6Office for National Statistics (ONS) . User Guide to Mortality Statistics. 2024. https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/methodologies/userguidetomortalitystatisticsjuly 2017#cause-of-death-coding (24 June 2024, date last accessed).
- 7Office for National Statistics (ONS) . Excess Deaths in England and Wales: March 2020 to December 2022. 2023. https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/articles/excessdeathsinenglandandwalesmarch 2020 todecember 2022/2023-03-09#comparison-of-excess-deaths-measures (24 June 2024, date last accessed).
- 8Office for National Statistics (ONS) . National Population Projections: 2022-Based. 2025. https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationprojections/bulletins/nationalpopulationprojections/2022 based#cite-this-statistical-bulletin (22 April 2025, date last accessed).