Imbalances in the Content of Sleep and Pain Assessments in Patients with Chronic Pain: A Scoping Review
Katsuyoshi Tanaka, Yuichi Isaji, Kosuke Suzuki, Kohei Okuyama, Yasuyuki Kurasawa, Masateru Hayashi, Takashi Kitagawa, Brett D Neilson, Katsuyoshi Tanaka

TL;DR
This review finds that most studies on chronic pain rely on self-reported sleep and pain assessments, with few using objective measures.
Contribution
The study highlights imbalances in assessment methods for sleep and pain in chronic pain research.
Findings
90.1% of studies used self-report sleep assessments, while only 9.9% used objective measures.
Visual analog and numeric rating scales were most common for pain assessment.
Multidimensional assessment tools are underutilized in sleep and pain research.
Abstract
Sleep disturbances frequently occur in concomitance with chronic pain, exacerbating its detrimental effects and diminishing patients’ quality of life. Although various studies have explored the relationship between chronic pain and sleep disturbances, comprehensive evidence on detailed assessment methods and their bidirectional interactions remains limited. This scoping review aimed to examine the characteristics and prevalence of assessment methods for sleep and pain-related outcomes in individuals with chronic pain. A comprehensive search of nine databases identified observational and interventional studies examining the relationship between sleep disturbances/disorders and chronic pain in adults. A literature search was conducted in MEDLINE, the Cochrane Central Register of Controlled Trials, Embase, PsycINFO, Web of Science, Cumulative Index to Nursing and Allied Health Literature…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
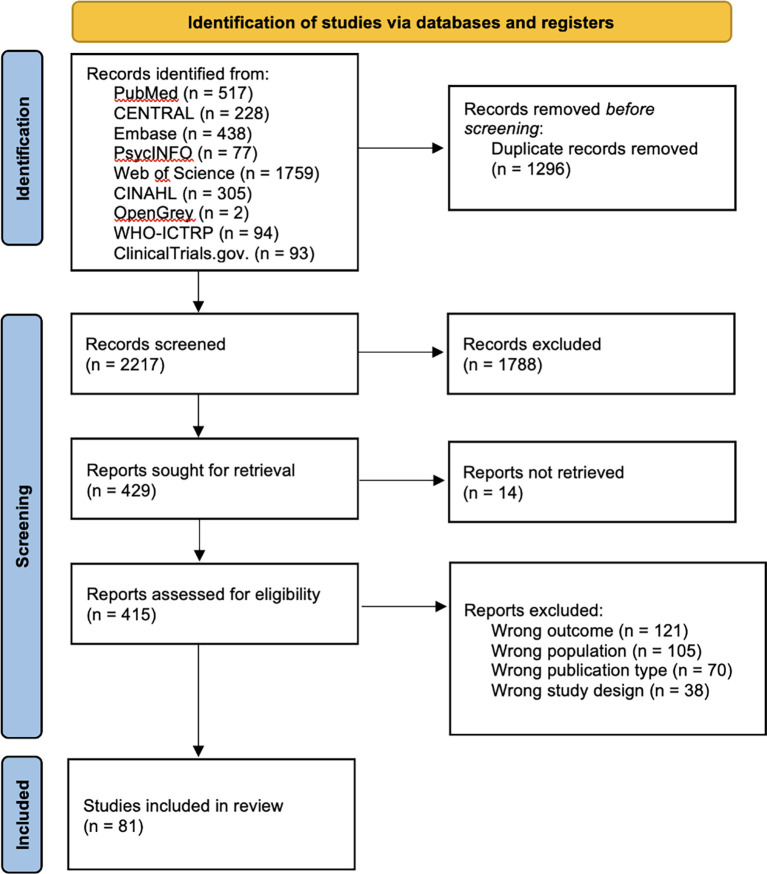 Figure 1
Figure 1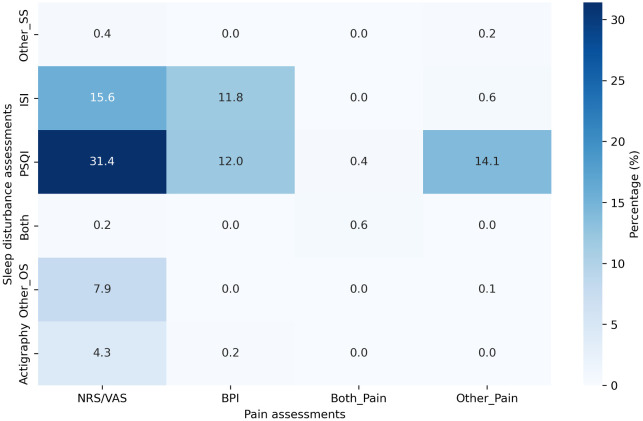 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSleep and related disorders · Musculoskeletal pain and rehabilitation · Obstructive Sleep Apnea Research
1. Introduction
The World Health Organization recognizes chronic pain as a disease, making it one of the most prevalent conditions worldwide. ^ 1 ^ Chronic pain results in significant disability and imposes a substantial economic strain on society. ^ 2 ^ In addition to persistent pain, individuals with chronic pain experience various consequences, including deterioration in the quality of life (QOL), higher prevalence of depressive symptoms, and greater levels of disability compared with those without pain. ^ 3 ^ The financial impact of chronic pain, including healthcare expenses and reduced work efficiency, is substantial. This underlines the extensive influence of pain on the individual and the community as a whole. Furthermore, chronic pain often coexists with sleep disturbances, which exacerbate the adverse effects of pain, adding to the overall strain on individuals and society. ^ 4, 5 ^
Patients with chronic pain frequently develop sleep problems and disorders. ^ 6– 8 ^ Sleep problems, such as inadequate sleep, and sleep disorders, including insomnia and obstructive sleep apnea, represent significant and widespread health concerns. ^ 9, 10 ^ Notably, the prevalence of sleep problems and sleep disorders is high among patients with chronic musculoskeletal pain, affecting approximately 75% and 44% of such individuals, respectively. ^ 8, 11 ^ Previous studies have suggested a correlation between compromised sleep and reduced QOL, adverse general health outcomes, elevated levels of depression, and diminished physical function. ^ 12 ^ Additionally, the concomitance of chronic pain and sleep disturbances leads to further deterioration in overall health and QOL. A bidirectional association has also been suggested, wherein pain negatively affects sleep, and sleep disturbances contribute to increased pain. ^ 13 ^
Polysomnography, which is considered the gold standard for the objective assessment of sleep, has been used in various chronic pain conditions, such as fibromyalgia, rheumatoid arthritis, osteoarthritis, and temporomandibular pain. ^ 6, 14 ^ In addition to polysomnography, sleep assessment, encompassing sleep duration and quality, has been conducted using several tools, such as actigraphy, questionnaires, and wearable devices. ^ 15, 16 ^ Moreover, although several studies have investigated the relationship between sleep and chronic pain, most existing reviews have focused on specific populations, such as those with postsurgical pain, pediatric pain, or low back pain. ^ 17– 19 ^ Thus, comprehensive evidence on detailed methods for assessing the relationship between chronic pain and sleep disturbance remains scarce.
Therefore, this scoping review (ScR) aimed to examine the characteristics and prevalence of methods used to assess sleep and pain-related outcomes in individuals with chronic pain and to identify gaps in the evidence, with the objective of guiding future studies.
2. Methods
This ScR was conducted according to the Joanna Briggs Institute methodology. ^ 20 ^ The study was registered with the Open Science Framework ( https://osf.io/jc5qh/) on March 29, 2024. The inclusion criteria were established based on the participants, concept, and context of the study.
2.1 Eligibility criteria
This ScR included studies on individuals with chronic pain lasting for >3 months. Studies on individuals with malignancy-related or cancer-related pain or acute pain conditions, such as postoperative pain, were excluded. Moreover, studies that included children (≤18 years) and/or participants with other conditions besides chronic pain were excluded. No restrictions were imposed with respect to the sex, location, race, country, or language of the participants. This review evaluated the measurement tools used for sleep assessment in individuals with chronic pain conditions, including polysomnography, wearable devices, and questionnaires. Additionally, we identified various types of pain-related assessments, including pain intensity, severity, disability, catastrophizing, threshold, and tolerance. In other words, we included studies that involved sleep assessments in individuals with chronic pain conditions.
This ScR included randomized controlled trials (RCTs), crossover trials, quasi-RCTs, non-RCTs, cross-sectional studies, and prospective and retrospective cohort studies, encompassing both observational and interventional designs. Protocols and conference abstracts were included in the initial screening, with a secondary screening conducted to verify the existence of published articles. Case reports, case-control studies, systematic reviews, meta-analyses, and narrative reviews were excluded.
2.2 Search strategy
The search strategy was designed to identify both published and unpublished studies. A literature search was conducted in MEDLINE, the Cochrane Central Register of Controlled Trials, Embase, PsycINFO, Web of Science, Cumulative Index to Nursing and Allied Health Literature (CINAHL) as well as gray literature sources, Open Grey. In addition, the following trial registries were searched for ongoing or unpublished trials: the World Health Organization International Clinical Trials Registry Platform and ClinicalTrials.gov.
The text words found in the titles and abstracts of relevant articles, along with the index terms used to describe the articles, were used to develop a comprehensive search strategy across nine databases (Table S1). Previous studies were also referenced. ^ 17, 21, 22 ^ Studies published in any language were included, with no restrictions on the publication date. The final comprehensive search was conducted on March 29, 2024.
2.3 Study selection and source of evidence
All identified citations were collated and uploaded into Rayyan (Qatar Computing Research Institute, Ar Rayyan, Qatar, https://www.rayyan.ai/), and duplicates were removed. Following a pilot test, two or more independent reviewers (K.T. and Y.I.) screened the study titles and abstracts based on the eligibility criteria. The full text of relevant sources was retrieved, and their citation details were imported into Rayyan. Two or more independent reviewers (K.T., Y.I., K.S., M.H., K.O., and Y.K.) assessed the full text of the selected studies based on the eligibility criteria. The reasons for excluding sources that did not meet the eligibility criteria were documented and reported in this ScR. Any disagreements between reviewers at each stage of selection were resolved through discussion or by consulting additional reviewers.
The results of the search and study inclusion process were comprehensively reported in the final ScR and illustrated in a Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for ScR flow diagram. ^ 23 ^
2.4 Data extraction
Data were extracted from the included studies using Microsoft Excel (Microsoft Corp., Redmond, WA, USA) by the first author (K.T.), with the assistance of ChatGPT-4o (San Francisco, CA, USA) and NotebookLM (Mountain View, CA, USA). ^ 24, 25 ^ The extracted data included the first author’s name, country of origin, study design, sample size, participant characteristics (age, sex, and diagnosis), and tools used for assessing sleep disturbance and pain-related outcomes. The draft data extraction tool was modified and refined as necessary throughout the data extraction process. Where necessary, the authors of the included studies were contacted to obtain any missing or additional data.
3. Results
3.1 Study selection
A total of 3,513 articles were retrieved during the database search. After eliminating 1,296 duplicates, the titles and abstracts of 2,217 articles were screened. Thereafter, the full texts of the remaining 415 articles were assessed for eligibility. Ultimately, only 81 studies that met the eligibility criteria were included in the analysis ( Figure 1).
PRISMA flow diagram illustrating the structure of the search and screening process.
3.2 Study and participant characteristics
Of the 81 included studies, 26 (32.1%) were RCTs, ^ 26– 51 ^ while the remaining studies were non-RCTs. ^ 52– 106 ^ The included studies were published between 1998 and 2024, with nearly half (45.7%, 37 of 81) published within the last 5 years. ^ 28– 30, 32– 34, 38, 39, 41, 46, 49– 52, 56, 57, 61, 65, 66, 71, 74, 76– 80, 83– 85, 88– 91, 93, 94, 99, 104 ^ The distribution of participants varied across studies: 31 studies (38.3%) focused on examining patients with chronic pain, irrespective of pain type, accounting for 40.5% of the total participants (7,413 out of 18,316). ^ 30, 36, 40, 45, 49, 50, 52, 55, 56, 63, 65, 67– 71, 74, 77, 78, 80, 83, 86, 87, 89, 90, 92, 95, 97, 99, 101, 104 ^ Eleven studies (13.6%) investigated patients with chronic low back pain, accounting for 12.4% of the total participants (2,266 participants). ^ 31, 34, 44, 46, 54, 79, 88, 93, 96, 105, 106 ^ Eight studies (9.9%) examined patients with chronic musculoskeletal pain, irrespective of location, accounting for 9.1% of the total participants (1,667 individuals). ^ 39, 60– 62, 75, 76, 84, 103 ^ Six studies (7.4%) assessed patients with chronic neck pain, comprising 5.2% of the total participants (950 participants). ^ 32, 38, 58, 59, 94, 98 ^
3.3 Outcome measurements
An overview of the included studies is presented in supplemental materials (Table S2, S3). Various methods have been used to assess sleep problems and pain-related outcomes, with patient-reported outcomes (PROs) being the most frequently utilized.
The Pittsburgh Sleep Quality Index (PSQI) and Insomnia Severity Index (ISI) were the most commonly used tools for the assessment of sleep problems. Other self-reported sleep assessment methods used included the Athens Insomnia Scale and sleep diaries. Sleep problems were predominantly assessed based on the participant’s entries in sleep diaries. In terms of study methodology, 73 of 81 studies (90.1%) relied solely on PROs (90.1% [73/81]). ^ 28– 51, 58– 106 ^ Only 2 of 81 studies (2.5%) relied solely objective assessments, ^ 56, 57 ^ such as actigraphy, whereas 6 of 81 studies (7.4%) used a combination of PROs and objective assessments. ^ 26, 27, 52– 55 ^ Other objective sleep assessment methods used included polysomnography and electroencephalography.
For PRO assessments, the outcomes were frequently evaluated using the numeric rating scale (NRS) or visual analog scale (VAS) (58.0% [47/81]). ^ 30, 32– 39, 42, 43, 47, 48, 50, 51, 53– 60, 62– 64, 68– 70, 75, 77, 79, 83, 85, 86, 88, 89, 92– 96, 98, 101, 103, 105, 106 ^ The Brief Pain Inventory (BPI) was the second most frequently used pain assessment tool (28.4% [23/81]). ^ 26, 28, 29, 31, 40– 42, 44, 45, 49, 55, 61, 65– 67, 71, 74, 76, 78, 80, 84, 87, 97 ^ Additional pain-related outcome measures included the Multidimensional Pain Inventory and Pain Disability Questionnaire. Psychometric factors were evaluated in more than half of the included studies (60.5% [49/81]). ^ 28, 30, 33– 36, 39, 40, 42, 45, 47, 48, 50, 52, 53, 56, 58– 61, 67– 77, 81– 83, 85, 88– 93, 95– 97, 100, 101, 103, 104, 106 ^ Objective pain assessment was rarely performed, with only one study utilizing quantitative sensory testing. ^ 96 ^
Figure 2 presents the detailed percentages of the combined use of sleep problems and pain-related outcome assessments. The NRS/VAS was frequently used in combination with the PSQI (31.4%), followed by combination of the NRS/VAS with the ISI (15.6%). The simultaneous use of both self-report and objective sleep assessments, along with the NRS or VAS and the BPI, was extremely rare, occurring in only 0.6% of studies ( Figure 2).
Percentage of the combined use of sleep problem and pain-related outcome assessments.
4. Discussion
This ScR highlighted the use of various measurement tools for assessing sleep and pain. The review emphasized the diversity of assessment tools used to evaluate sleep and pain, revealing substantial inconsistencies and the lack of standardization. Despite the large body of research on this topic, critical gaps persist, particularly the absence of generalizable objective measurements for sleep assessment, which may hinder the reliability and applicability of the current findings.
A key finding of this review is the predominant reliance on self-report measures for evaluating sleep disturbances. Over 90% of the included studies utilized PROs, such as the PSQI or the ISI. Although these tools provide practical and accessible methods of assessing perceived sleep quality, they are inherently limited by individual biases and self-reported variability. ^ 107, 108 ^ In contrast, objective measures such as actigraphy and polysomnography provide precise and quantifiable data on sleep architecture, including sleep stages, latency, and fragmentation. ^ 109, 110 ^ However, these tools were employed by only a small portion of the included studies, with objective methods utilized by 9.9% (8/81) of studies. This imbalance likely stems from the challenges, which traditionally include cost and other constraints, hindering the use of objective measures, thereby complicating the comprehensive assessment of sleep disturbances. ^ 111, 112 ^ Future research should prioritize the integration of these objective tools to provide a more robust understanding of sleep problems in individuals with chronic pain.
Beyond sleep assessment, this review also identified variability and potential bias in the pain-related outcome evaluations. Most studies focused primarily on examining pain intensity, often measured using the NRS or the VAS. Although these tools are widely used and validated, ^ 113, 114 ^ they only capture one aspect of the complex pain experience. ^ 115– 117 ^ Approximately half of the studies assessed the psychological factors associated with pain, but other important domains, such as pain-related disability and sensitization, were less frequently explored. Notably, only one study included in this review utilized quantitative sensory testing. ^ 96 ^ This limited focus restricts the understanding of pain mechanisms and hinders the development of targeted treatment strategies. More comprehensive pain assessment protocols that incorporate these additional dimensions are necessary to produce clinically relevant evidence. ^ 118 ^
The complex relationship between sleep disturbances and chronic pain necessitates a multidimensional research approach. Existing evidence suggests that sleep disturbances can exacerbate pain through mechanisms such as increased central sensitization, impaired descending pain inhibition, and heightened emotional distress. ^ 119– 121 ^ Addressing these gaps in assessment methodologies is crucial for advancing the field. Incorporating objective sleep assessments and multidimensional pain measures into research and clinical practice will enhance the quality of evidence and support the development of precision medicine approaches tailored to individual patient needs. Furthermore, interdisciplinary collaboration that brings together experts in neurology, psychology, and bioinformatics could facilitate the development of innovative assessment tools and therapeutic interventions.
This review has some limitations. The lack of synthesis of the findings restricted our ability to evaluate methodological rigor and the overall reliability of the evidence. Additionally, the possibility of overlooking relevant studies cannot be completely excluded, which may have introduced selection bias. However, this review included gray literature and non-English studies to mitigate this potential bias.
5. Conclusions
This ScR highlights the imbalance in the content of sleep and pain assessments, indicating the need for a more comprehensive evaluation of sleep disturbances and pain-related outcomes. Addressing the gaps in objective and multidimensional assessments could facilitate the development of personalized interventions that improve patient outcomes and overall quality of care.
Ethics and consent
This scoping review did not involve human participants directly, and therefore ethical approval was not required.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Treede RD Rief W Barke A : Chronic pain as a symptom or a disease: the IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain. 2019;160:19–27. 10.1097/j.pain.0000000000001384 30586067 · doi ↗ · pubmed ↗
- 2GBD 2017 Disease and Injury Incidence and Prevalence Collaborators: Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1789–1858. 10.1016/S 0140-6736(18)32279-7 30496104 PMC 6227754 · doi ↗ · pubmed ↗
- 3Andersen LN Kohberg M Juul-Kristensen B : Psychosocial aspects of everyday life with chronic musculoskeletal pain: A systematic review. Scand. J. Pain. 2017;5:131–148. 10.1016/j.sjpain.2014.01.001 29913683 · doi ↗ · pubmed ↗
- 4Toprak Celenay S Karaaslan Y Mete O : Coronaphobia, musculoskeletal pain, and sleep quality in stay-at home and continued-working persons during the 3-month Covid-19 pandemic lockdown in Turkey. Chronobiol. Int. 2020;37:1778–1785. 10.1080/07420528.2020.1815759 32878506 · doi ↗ · pubmed ↗
- 5Finan PH Goodin BR Smith MT : The association of sleep and pain: An update and a path forward. J. Pain. 2013;14:1539–1552. 10.1016/j.jpain.2013.08.007 24290442 PMC 4046588 · doi ↗ · pubmed ↗
- 6Wu Y-L Chang L-Y Lee H-C : Sleep disturbances in fibromyalgia: A meta-analysis of case-control studies. J. Psychosom. Res. 2017;96:89–97. 10.1016/j.jpsychores.2017.03.011 28545798 · doi ↗ · pubmed ↗
- 7Koffel E Kroenke K Bair MJ : The bidirectional relationship between sleep complaints and pain: Analysis of data from a randomized trial. Health Psychol. 2016;35:41–49. 10.1037/hea 0000245 26076002 PMC 4900176 · doi ↗ · pubmed ↗
- 8Mathias JL Cant ML Burke ALJ : Sleep disturbances and sleep disorders in adults living with chronic pain: a meta-analysis. Sleep Med. 2018;52:198–210. 10.1016/j.sleep.2018.05.023 30314881 · doi ↗ · pubmed ↗