Impact of Living Place on the Prognosis of Aspiration Pneumonia in Elderly Patients: A Retrospective Study in Tokyo
Yuki Shimazu, Clara So, Torahiko Jinta, Tomoaki Nakamura, Kohei Okafuji, Atsushi Kitamura, Yutaka Tomishima, Naoki Nishimura

TL;DR
This study shows that elderly patients with aspiration pneumonia who live in nursing homes have better survival rates than those living at home.
Contribution
The study identifies living place as a novel social factor influencing the prognosis of aspiration pneumonia in elderly patients.
Findings
Patients in nursing homes had a 38% lower mortality rate compared to those living at home.
Home patients with two or more cohabitants had a higher mortality rate, though not statistically significant.
Social factors like living place should be considered in aspiration pneumonia care strategies.
Abstract
Introduction In Japan, aspiration pneumonia is a major cause of death among the elderly. While clinical factors are well-documented, the impact of social factors on the prognosis of aspiration pneumonia remains underexplored. This study investigates whether social factors, such as living place and caregiver presence, influence the prognosis of aspiration pneumonia. Methods This retrospective study analyzed patients aged 65 and older admitted for aspiration pneumonia at our hospital from January 2012 to December 2022. The study included 650 patients after excluding those with pneumonia onset after admission, interstitial pneumonia, and cancer or those on immunosuppressants. Clinical data, including age, sex, comorbidities, and Pneumonia Patient Outcomes Research Team (PORT) score, were collected alongside social factors such as the level of care needed, living place, and cohabitant…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
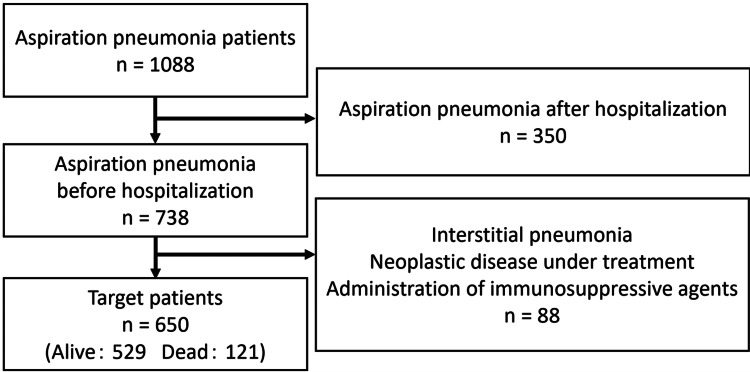 Figure 1
Figure 1| Level of care needed | Definition |
| Support level 1 | Individuals at this level require some assistance with daily activities but are relatively independent. They might need help with complex tasks such as meal preparation and cleaning but can manage personal care independently. |
| Support level 2 | These individuals need more assistance than those in support level 1. They require help with both personal care and household tasks more frequently but can still maintain some level of independence. |
| Care level 1 | Individuals need partial assistance with daily activities such as bathing, dressing, and eating. They may also require support with mobility and other basic personal care tasks. |
| Care level 2 | At this level, individuals require a higher degree of support, including significant help with personal care and some medical supervision. They often need assistance with most daily activities. |
| Care level 3 | Individuals need extensive assistance with daily activities and regular supervision. They require help with most personal care tasks and some medical needs. This level typically indicates a moderate degree of dependency. |
| Care level 4 | These individuals need intensive assistance with almost all daily activities and constant supervision. They require significant help with personal care and medical needs and may have limited mobility. |
| Care level 5 | The highest level of care, individuals at this level are almost entirely dependent on caregivers for all aspects of daily living. They need comprehensive support with personal care, medical care, and constant supervision. |
| Characteristics | Total (n = 650) | Alive (n = 529) | Dead (n = 121) | T value or chi value | P value |
| Age (years, mean ± SD) | 86.7 ± 7.5 | 86.3 ± 7.7 | 88.2 ± 6.5 | -2.69 | 0.016 |
| Sex | |||||
| Male (%) | 334 (51.4) | 261 (49.3) | 73 (60.3) | 4.33 | 0.037 |
| Female (%) | 316 (48.6) | 268 (50.7) | 48 (39.7) | ||
| Comorbidity | |||||
| Neoplastic disease (%) | 129 (19.8) | 103 (19.5) | 26 (21.5) | 0.14 | 0.71 |
| Liver disease (%) | 22 (3.4) | 18 (3.4) | 4 (3.3) | 0.4 × 10-28 | 1.0 |
| Cerebrovascular disease (%) | 255 (39.2) | 216 (40.8) | 39 (32.2) | 2.71 | 0.10 |
| Congestive heart failure (%) | 115 (17.7) | 81 (15.3) | 34 (28.1) | 10.2 | <0.001 |
| Renal disease (%) | 80 (12.3) | 59 (11.2) | 21 (17.4) | 2.96 | 0.085 |
| PORT score (mean ± SD) | 140 ± 26.9 | 137 ± 26.6 | 153 ± 24.7 | -6.055 | <0.001 |
| Characteristics | Total (n = 650) | Alive (n = 529) | Dead (n = 121) | T value or chi value | P value |
| Level of care needed | |||||
| No care application or applied but unclear (%) | 152 (23.4) | 125 (23.6) | 27 (22.3) | 0.036 | 0.85 |
| Support level 1 to care level 3 (%) | 206 (31.7) | 165 (31.2) | 41 (33.9) | 0.22 | 0.64 |
| Care level 4 to care level 5 (%) | 292 (44.9) | 239 (45.2) | 53 (43.8) | 0.030 | 0.86 |
| Living place | |||||
| Nursing home (%) | 264 (40.6) | 223 (42.2) | 41 (33.9) | 2.46 | 0.12 |
| Home (%) | 386 (59.4) | 306 (57.8) | 80 (66.1) | ||
| The number of cohabitants at home | |||||
| Zero cohabitant (%) | 60 (9.2) | 46 (7.1) | 14 (2.2) | 0.66 | 0.42 |
| One or more cohabitants (%) | 326 (50.2) | 260 (40.0) | 66 (10.2) | 0.94 | 0.33 |
| Zero or one cohabitant (%) | 262 (40.3) | 208 (39.3) | 54 (44.6) | 0.94 | 0.33 |
| Two or more cohabitants (%) | 124 (19.1) | 98 (18.5) | 26 (21.5) | 0.38 | 0.54 |
| Characteristics | Total (n = 650) | Home (n = 386) | Nursing home (n = 264) | T value or chi value | P value |
| Age (years, mean ± SD) | 86.7 ± 7.5 | 85.8 ± 7.6 | 88.0 ± 7.1 | -3.82 | <0.001 |
| Sex | |||||
| Male (%) | 334 (51.4) | 222 (57.5) | 112 (42.4) | 13.7 | <0.001 |
| Female (%) | 316 (48.6) | 164 (42.5) | 152 (57.6) | ||
| Comorbidity | |||||
| Neoplastic disease (%) | 129 (19.8) | 75 (19.4) | 54 (20.5) | 0.049 | 0.83 |
| Liver disease (%) | 22 (3.4) | 15 (3.9) | 7 (2.7) | 0.40 | 0.53 |
| Cerebrovascular disease (%) | 255 (39.2) | 141 (36.5) | 114 (43.2) | 2.64 | 0.10 |
| Congestive heart failure (%) | 115 (17.7) | 72 (18.7) | 43 (16.3) | 0.45 | 0.50 |
| Renal disease (%) | 80 (12.3) | 49 (12.7) | 31 (11.7) | 0.058 | 0.81 |
| PORT score (mean ± SD) | 140 ± 26.9 | 134 ± 26.0 | 149 ± 25.9 | -7.07 | <0.001 |
| Level of care needed | |||||
| No care application or applied but unclear (%) | 152 (23.4) | 101 (26.2) | 51 (19.3) | 3.73 | 0.05 |
| Support level 1 to care level 3 (%) | 206 (31.7) | 140 (36.3) | 66 (25.0) | 8.68 | 0.003 |
| Care level 4 to care level 5 (%) | 292 (44.9) | 145 (37.6) | 147 (55.7) | 20.07 | <0.001 |
| Mortality | 121 (18.6) | 80 (20.7) | 41 (15.5) | 2.46 | 0.12 |
| Odds ratio (95% CI) | P value | |
| Modified PORT score | 1.03 (1.02-1.03) | <0.001 |
| Level of care needed | ||
| No care application or applied but unclear/care level 4 to care level 5 | 1.04 (0.61-1.77) | 0.87 |
| Support level 1 to care level 3/care level 4 to care level 5 | 1.05 (0.65-1.68) | 0.85 |
| Living place | ||
| Nursing home/home | 0.62 (0.40-0.95) | 0.030 |
| Odds ratio (95% CI) | P value | |
| Modified PORT score | 1.03 (1.02-1.03) | <0.001 |
| Level of care needed | ||
| No care application or applied but unclear/care level 4 to care level 5 | 1.05 (0.61-1.78) | 0.87 |
| Support level 1 to care level 3/care level 4 to care level 5 | 1.05 (0.65-1.69) | 0.84 |
| Living place and the number of cohabitants at home | ||
| Zero or one cohabitant/nursing home | 1.60 (1.00-2.58) | 0.053 |
| Two or more cohabitants/nursing home | 1.67 (0.94-2.94) | 0.076 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDysphagia Assessment and Management · Palliative Care and End-of-Life Issues · Nosocomial Infections in ICU
Introduction
In Japan, which has an aged society, aspiration pneumonia is a major cause of death [1]. Aspiration pneumonia significantly affects the lifespan of the elderly. In fact, the one-month mortality rate of aspiration pneumonia is 17.2% [2], and the three-month mortality rate of it is 38.6% [3]. Therefore, predicting the prognosis is important for both patients and their families. The cause of aspiration pneumonia is associated with aspiration episodes, so not only clinical factors but also social factors, such as the patient's level of independence in daily living, where the patient lives, and who the patient's caregiver is, might be related to the prognosis of aspiration pneumonia.
Previous studies have identified age, sex, comorbidities, the severity of dysphagia, the level of daily living independence, nutritional status, the presence of alternative nutrition, and oral hygiene as prognostic factors for aspiration pneumonia [4-9]. To the best of our knowledge, few studies have investigated the social factors that impact the prognosis of aspiration pneumonia.
According to Tomonaga et al.'s study, half of aspiration pneumonia cases occur at home, and half occur in nursing homes [10]. This study surveyed social factors such as the patient's living place and who the patient's caregiver is. Many patients with aspiration pneumonia are elderly, so caregiving to prevent aspiration is crucial for aspiration pneumonia. It is highly possible that the prognosis differs between patients with well-established social services and those without.
This study aims to investigate whether social factors are associated with the prognosis of aspiration pneumonia and to understand how we can adjust for social factors to improve the prognosis of aspiration pneumonia.
Materials and methods
Subjects
This retrospective study was conducted targeting patients aged 65 years and older who were admitted to the Department of Pulmonary Medicine or General Medicine at our hospital for aspiration pneumonia between January 2012 and December 2022. The Institutional Review Board of St. Luke's International Hospital issued approval 23-J007. The diagnostic criteria for aspiration pneumonia were based on the diagnostic flowchart for aspiration pneumonia described in the Japanese Guidelines for the Management of Nursing- and Healthcare-Associated Pneumonia. Specifically, aspiration pneumonia was diagnosed in patients who showed radiographic evidence of pneumonia on chest X-ray or chest CT and had elevated C-reactive protein (CRP) levels, together with either witnessed aspiration or a suspected decline in swallowing function [11].
Exclusion criteria included the onset of aspiration pneumonia after hospitalization, concurrent interstitial pneumonia, concurrent neoplastic disease requiring treatment, and the ongoing administration of immunosuppressive agents.
Data collection
We set mortality as the primary outcome. Data on clinical factors such as age, sex, comorbidities (neoplastic disease, liver disease, cerebrovascular disorder, congestive heart failure, and kidney disease), and Pneumonia Patient Outcomes Research Team (PORT) score were extracted [12]. The PORT score, which is used as a prognostic score for community-acquired pneumonia, includes a wide range of prognostic factors, such as comorbidities and vital signs at admission. The PORT score includes clinical factors so broadly that using the PORT score as an independent variable is useful when considering the influence of only social factors in multivariable analysis.
The level of care needed, where the patient lives, and who the patient's caregiver is were extracted as social factors. In Japan, the long-term care system is structured to provide support to individuals who need assistance due to aging, illness, or disability. The system includes different levels of care: support level 1 or 2 and care levels 1-5. Table 1 shows that each level signifies a different degree of care needed [13]. We categorized the patients' living place as either living at home or residing in a nursing home. In the case of the patients who live at home, the numbers of their cohabitants were also extracted.
Statistical analyses
A univariate analysis was performed using t-tests and chi-square tests, and a multivariable analysis was performed using logistic regression analysis. In the multivariable analysis, the "nursing home resident" item of the PORT score was confounded with the independent variable of whether the patient resides in a nursing home or at home. Therefore, we used the modified PORT score, which excludes the "nursing home resident" item of the PORT score, for the multivariable analysis. We utilized the patient's living place, the level of care needed, and the number of cohabitants at home as independent variables representing social factors. The number of cohabitants at home was treated as a categorical variable, classified into either "one or zero" or "two or more."
The significance level was set at P < 0.05. All statistical analyses were conducted using R (R Foundation for Statistical Computing, Vienna, Austria) and RStudio (Posit Software, Boston, MA) software.
Results
Figure 1 illustrates the flowchart for selecting the study participants. Among 1088 patients who met the diagnostic criteria for aspiration pneumonia, 350 developed aspiration pneumonia after admission. A total of 88 patients had concurrent interstitial pneumonia, ongoing treatment for malignant tumors, or immunosuppressive agents. Thus, the analysis included 650 patients, 529 survivors and 121 deceased patients, resulting in a mortality rate of 18.6%.
Flowchart of patient selection
The patients' clinical characteristics are presented in Table 2. Age, sex, the presence of congestive heart failure, and PORT score showed significant differences. Conversely, no significant differences were observed in social factors, such as the level of care needed (classified as no care application or applied but unclear/support level 1 to care level 3/care level 4 to care level 5) and living environment (nursing home/home) (Table 3). Table 4 compares the characteristics of patients in the nursing home group and the home group. Patients in the nursing home group were older, had a higher PORT score at admission, and more often had a higher level of care need. However, no significant difference in mortality was observed between the two groups. A multivariable analysis using a modified PORT score and social factors as independent variables revealed significant differences, with lower mortality rates observed in the nursing home group than in the home group (Table 5) (odds ratio, 0.62; 95% CI, 0.40-0.95).
Furthermore, the multivariable analysis categorizing the home group based on the number of cohabitants showed that even patients residing at home with two or more cohabitants tended to have a higher mortality rate compared to those in nursing homes, although there was no significant difference (Table 6) (odds ratio, 1.67; 95% CI, 0.94-2.94).
Discussion
This study highlights that the living place of elderly patients is a significant social determinant of mortality in aspiration pneumonia, with an overall mortality rate of 18.6%. Aspiration pneumonia primarily affects elderly individuals, largely due to their multiple comorbidities and repeated episodes of aspiration resulting from a decline in swallowing function [14]. Furthermore, a multivariable analysis considering a wide range of clinical factors and social factors showed that the level of care needed and the number of the patient's cohabitants at home did not significantly affect the prognosis of aspiration pneumonia, whereas the patient's living place did.
This study is the first to suggest the potential influence of the patient's living place on the prognosis of aspiration pneumonia. The lower mortality rates observed among patients in nursing homes compared to those at home may be due to better nutritional status in nursing homes [14]. At home, preparing meals adapted to the patient's swallowing ability and assisting with their meals can be burdensome for families. In contrast, nursing homes can consistently provide well-balanced, dysphagia-friendly meals, with staff available to assist during mealtime. These nutritional advantages may contribute to greater physical resilience against aspiration pneumonia.
Another factor may be oral hygiene, which tends to be better maintained in nursing homes [15]. Poor oral hygiene can lead to increased oral bacterial growth, especially in elderly individuals who produce less saliva. Patients with weakened swallowing and cough reflexes are particularly susceptible to aspirating these bacteria, increasing their risk of infection. In institutional settings, oral care practices are typically routine and supervised, potentially lowering the bacterial burden that contributes to aspiration pneumonia.
Additionally, caregivers in nursing homes are generally more familiar with preventive strategies for aspiration [16], including monitoring patients' eating pace and posture [17]. These factors are critical in preventing aspiration events. In contrast, at home, family members may not recognize the early signs of aspiration pneumonia, leading to delays in seeking medical care. Prompt recognition and early intervention can significantly improve outcomes, highlighting the importance of trained caregivers and structured care environments.
The limitations of this study include its retrospective nature in a single institution and the lack of outcome tracking after discharge. As discussed above, this study proposes possible mechanisms, such as differences in nutritional management, oral hygiene, and caregiver expertise, to explain the better prognosis observed in nursing homes. However, these factors were not directly measured in our analysis. Therefore, the proposed explanations remain speculative and should be explored in future prospective studies that incorporate these variables. Future research should also examine how differences in caregiving services among nursing homes, or the frequency of home care and nursing visits, affect the prognosis of aspiration pneumonia.
Conclusions
This study demonstrates that the living place, specifically residing in a nursing home, is associated with a lower mortality rate in elderly patients with aspiration pneumonia, whereas other social factors, such as the level of care needed and the number of cohabitants at home, do not significantly impact prognosis.
The findings suggest that the comprehensive care provided in a nursing home may contribute to improved outcomes. Recognizing the importance of living place as a prognostic factor could help inform care strategies and early intervention practices to reduce mortality in patients with aspiration pneumonia.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Overview of the annual population statistics monthly report for the year 4 of Reiwa era 11 2024 2022 https://www.mhlw.go.jp/toukei/saikin/hw/jinkou/geppo/nengai 22/dl/gaikyou R 4.pdf
- 2Risk factors for aspiration in community-acquired pneumonia: analysis of a hospitalized UK cohort Am J Med Taylor JK Fleming GB Singanayagam A Hill AT Chalmers JD 995100112620132405417610.1016/j.amjmed.2013.07.012 · doi ↗ · pubmed ↗
- 3Clinical features and outcomes of aspiration pneumonia compared with non-aspiration pneumonia: a retrospective cohort study J Infect Chemother Hayashi M Iwasaki T Yamazaki Y 4364422020142483486610.1016/j.jiac.2014.04.002 · doi ↗ · pubmed ↗
- 4Medium- to long-term survival and prognostic factors for patients with aspiration pneumonia (Article in Japanese)Jpn J Dysphagia Rehabil Tsukatani T Kobayashi S Kanehara H 247257242020
- 5Aspiration pneumonia: dental and oral risk factors in an older veteran population J Am Geriatr Soc Terpenning MS Taylor GW Lopatin DE Kerr CK Dominguez BL Loesche WJ 5575634920011138074710.1046/j.1532-5415.2001.49113.x · doi ↗ · pubmed ↗
- 6The current definition, epidemiology, animal models and a novel therapeutic strategy for aspiration pneumonia Respir Investig Teramoto S 455560202210.1016/j.resinv.2021.09.01234782300 · doi ↗ · pubmed ↗
- 7Aspiration pneumonia: a key concept in pneumonia treatment Intern Med Ebihara S Miyagi M Otsubo Y Sekiya H Ebihara T 132913306020213328117110.2169/internalmedicine.6576-20PMC 8170232 · doi ↗ · pubmed ↗
- 8Poor oral health in the etiology and prevention of aspiration pneumonia Clin Geriatr Med Scannapieco FA 2572713920233704553210.1016/j.cger.2023.01.010 · doi ↗ · pubmed ↗