Bidirectional relationships between pain and alcohol use among older adults: a scoping review
Lisa R LaRowe, Heily Chavez Granados, Lisa L Philpotts, Ana-Maria Vranceanu, Christine S Ritchie

TL;DR
This review explores how pain and alcohol use influence each other in older adults, finding that pain can lead to alcohol use, but the long-term effects of alcohol on pain are unclear.
Contribution
The study provides a comprehensive synthesis of bidirectional relationships between pain and alcohol use in older adults, highlighting a gap in existing research.
Findings
Pain can motivate alcohol use among older adults.
The long-term effects of alcohol use on pain outcomes remain unclear.
There are significant research gaps in understanding these relationships in older adults.
Abstract
Pain and alcohol use are highly prevalent and frequently co-occur among older adults. An established reciprocal model suggests that pain and alcohol use interact in the manner of a positive feedback loop. However, older adults have been underrepresented in this work. We conducted a scoping review to answer the following research questions: (a) What is known regarding the effects of alcohol use on pain among older adults? and (b) What is known regarding the effects of pain on alcohol use among older adults? A total of 15 studies describing interrelationships between pain and alcohol use among older adults were identified and described in this review. Findings provided convergent evidence that pain can motivate alcohol use in older adults. The effects of alcohol use on longer-term pain outcomes are less clear in this population. Major gaps and directions for future research are…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
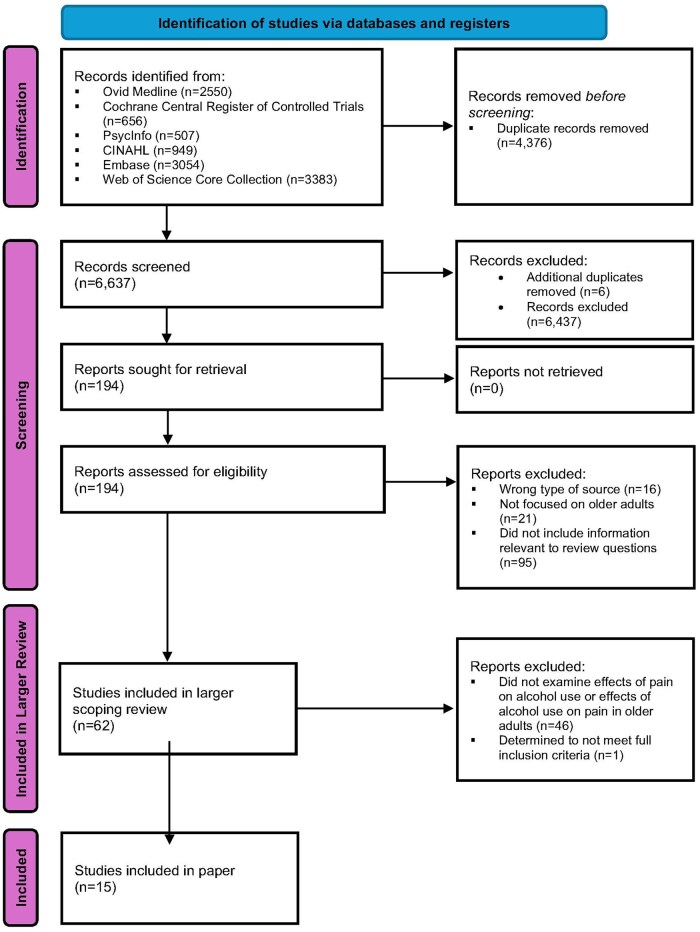 Figure 1
Figure 1| Reference | Country | Study design | Years of data collection | Sample description | Major findings | Alcohol variables | Pain variables |
|---|---|---|---|---|---|---|---|
| Acute alcohol analgesia | |||||||
|
| Sweden | Observational, cross-sectional | 2000-2001 | 294 adults aged ≥75 years who have chronic pain and are in need of help to manage activities of daily living | People living at home reported that alcohol was somewhat helpful for pain management (median = 2 on 1-5 scale), whereas people living in special accommodation reported that it is very helpful (median = 4). People living alone reported that alcohol was somewhat helpful (median = 2) for pain management, whereas people living with someone reported that it is somewhat to mostly helpful (median = 2.5). Alcohol was identified as one of the two most effective methods for pain management among those living in special accommodations. | Participants were asked about alcohol as a pain management method and helpfulness using the Pain Management Inventory (PMI). | Participants were asked about pain that lasts 3 months or longer. Individuals reporting at least “little pain” were asked to complete the Multidimensional Pain Inventory—Swedish version (MPI-S). |
|
| US | Observational, longitudinal | 2015-2016 | 55 adults aged ≥50 years who had HIV and chronic pain and screened positive for at-risk substance use | Use of alcohol to cope with pain was not a predictor of relief from pain ( | Participants were asked how many standard drinks were consumed in the last 24 hours. | Participants were asked if they had experienced pain in the last 24 hours. Participants reporting pain were asked about the worst pain in the last 24 hours, coping with pain and relief from pain were assessed using questions from the Brief Pain Inventory (BPI). |
|
| |||||||
|
| US | Retrospective cohort study | 1998-2006 | 26 545 veterans aged ≥65 years treated for a vertebral or hip fracture | Alcoholism was not a risk factor for musculoskeletal pain ( | Alcoholism status information was obtained from the VA Corporate Franchise Data Center. | Musculoskeletal pain (MSKP) data were obtained from patient records using ICD-9-CM codes compatible with MSKP, including codes for pain without a specific anatomic site (chronic pain), pain syndromes (generalized pain), or pain occurring at multiple sites that are not specified (joint pain, multiple sites). |
|
| UK | Observational, longitudinal | 2004-2005 and 2014-2015 | 2631 adults aged ≥50 years | Among participants who developed chronic pain, 25.6% reported drinking nearly every day, 40.7% reported drinking 5-6 days per week, 11.4% reported drinking 3-4 days per week, and 22.3% reported drinking 1-2 days per week. In comparison, among those who did not develop chronic pain, 29.3% reported drinking nearly every day, 42.5% reported drinking 5-6 days per week, 11.7% reported drinking 3-4 days per week, and 16.5% reported drinking 1-2 days per week. Lower alcohol consumption was associated with a greater likelihood of reporting chronic pain over the decade ( | Participants were asked about the frequency of alcohol consumption (1-2 days a week, 3-4 days a week, 5-6 days a week, daily). |
Participants were asked how often they were troubled by pain and the severity of their pain (mild, moderate, severe). Additionally, participants were asked to specify the location of pain. The study focused on moderate to severe pain reported by participants at any point during the 10-year follow-up. |
|
| US | Observational, longitudinal | 2006-2016 |
6132 adults aged ≥65 years with moderate to severe chronic pain. Participants were born between 1931 and 1941. | Alcohol consumption (days/week) was not associated with risk for developing moderate to severe chronic pain (RR = 1.00, CI: 0.98-1.03, | Alcohol consumption was determined from the number of days a participant drank per week. |
Participants were considered to have chronic pain if they indicated being troubled by pain often during an interview. They were then asked to rate the severity of pain and pain interference. Individuals reporting moderate or severe pain intensity or pain interfering with their usual activities were classified as having moderate to severe chronic pain. Those reporting no pain or pain without interference in activities were classified as not having moderate to severe chronic pain. |
|
| Finland | Observational, longitudinal | 2002, 2005, 2008, 2012 | 1954 adults born in 1926-1930, 1936-1940, and 1946-1950 | AUDIT-C scores were not associated with odds of remaining in a low pain intensity/low pain interference group (OR = 1.06, | Weekly alcohol consumption was measured with the AUDIT-C questionnaire. |
Frequency and severity of pain were assessed with the bodily pain portion of the SF-36 questionnaire. Pain was categorized into 4 pain intensity pain interference (PIPI) groups: PIPI I for none to mild pain intensity and interference, PIPI II for moderate to severe intensity with none to mild interference, PIPI III for none to mild intensity with moderate to extreme interference, and PIPI IV for moderate to severe intensity with moderate to extreme interference. |
|
| Australia | Observational, longitudinal | 2005-2007 | 1685 men aged ≥70 | The odds of reporting persistent pain at 24 months increased with each additional alcoholic drink per week (OR = 1.10, 95% CI: 1.01-1.22; | Standard number of drinks per week (0-12) was used to measure alcohol consumption. |
Participants self-reported the frequency and severity of low back pain in the past 12 months. At the time of enrollment, low back pain was defined as back pain that occurred some, most, or all of the time. |
| Reference | Country | Study design | Years of data collection | Sample description | Major findings | Alcohol variables | Pain variables |
|---|---|---|---|---|---|---|---|
| Pain as a motivator of drinking | |||||||
|
| US | Observational, longitudinal | 2015-2016 | 55 adults aged ≥50 years who had HIV and chronic pain and screened positive for at-risk substance use | The presence of any pain in the last 24 hours was not a significant predictor of same-day substance use (alcohol, marijuana, or other drug use). However, daily rating of worst pain in the last 24 hours was a significant predictor of alcohol use, such that for every one-unit increase in worst pain beyond an individual’s personal mean, alcohol use increased by a quarter drink. | Participants were asked how many standard drinks were consumed in the last 24 hours. | Participants were asked if they had experienced pain in the last 24 hours. Participants reporting pain were asked about the worst pain in the last 24 hours, coping with pain and relief from pain were assessed using questions from the Brief Pain Inventory (BPI). |
|
| |||||||
|
| Nepal | Qualitative | 2023 | 20 older adults aged ≥60 in Nepal | Qualitative results showed participants report using alcohol to reduce bodily pain. | Participants were asked if they currently consume alcohol. | Participants were asked about physical pain. |
|
| US | Observational, longitudinal | Not reported | 401 adults aged 55-65 who had consumed alcohol at some point in their lives |
Among men, 37.9% of problem drinkers report using alcohol to manage pain compared to 15.1% of non-problem drinkers ( Among women, 37.9% of problem drinkers report using alcohol to manage pain compared to 12.5% of non-problem drinkers ( Among both men and women, more bodily pain and more drinking problems at baseline were independent predictors of using alcohol to manage pain. A total of 49 participants initiated use of alcohol to manage pain over the 3-year follow-up interval and another 49 individuals stopped using alcohol to manage pain over the follow-up interval. |
Drinking problems were assessed with the Drinking Problems Index (DPI). At baseline, individuals were classified as current problem drinkers if their DPI responses indicated one or more drinking problems. Participants were asked to indicate how often in the past month they had used alcohol to manage pain (ranging from “never” to “very often”). |
Pain was assessed with the global bodily pain item from the Medical Outcomes Study (MOS) survey. Participants were asked to rate the amount of bodily pain experienced in the past month (none to very severe). A question from the MOS survey asked participant to rate the interference of bodily pain with their normal activities. |
|
| Sweden | Observational, cross-sectional | 2000-2001 | 294 adults aged ≥75 years who have chronic pain and are in need of help to manage daily activities of daily living | 3% of people living at home reported using alcohol for pain management compared to 2% of people living in special accommodation ( | Participants were asked about alcohol as a pain management method and helpfulness using the Pain Management Inventory (PMI). | Study questionnaire asked about pain that lasts 3 months or longer. Individuals reporting at least “little pain” were asked about their pain using the Multidimensional Pain Inventory—Swedish version (MPI-S). |
|
| US | Observational, cross-sectional | Not reported | 150 adults aged ≥65 years who had chronic pain and were prescribed opioid analgesics | Participants responded to an item stating: “At times, I drink alcohol to help my pain”, using a five-point Likert-type scale ranging from 0 (disagree) to 4 (agree). The modal response was 0, with a mean = 0.13 ( | Participants were asked to respond to an item stating: “At times, I drink alcohol to help my pain”. | Chronic pain was defined as pain that lasts for more than 3 months. |
|
| US | Observational, cross-sectional | Not reported | 1634 adults aged ≥65 years | When asked what they have done for specific symptoms in the past 12 months, 13% of older adults reported drinking alcohol for jaw joint pain, 24% for face pain, 16% for oral sores, 14% for burning mouth, and 22% for toothache. Male respondents were significantly more likely to report self-treating with alcohol than females for jaw joint pain (33% vs 7%, RR = 5.1, | Participants were asked how often they drink alcohol (wine, beer, or liquor). | Participants were asked about occurrence of jaw joint pain, face pain, oral sores, burning mouth, and toothache pain during the last 12 months. |
|
| US | Observational, longitudinal | Not reported | 719 adults aged 55-65 who had consumed alcohol at some point in their lives and had outpatient contact with a healthcare facility in the past 3 years | A total of 20% and 22% of older adults reported using alcohol to manage pain at the 10-year and 20-year follow-ups, respectively. At both follow-up time points, individuals who relied more on alcohol to manage pain drank more frequently and in heavier amounts. Those who relied more on alcohol to reduce pain also reported more warning signs of negative consequences of alcohol consumption and had more drinking problems ( |
Participants were asked to rate how often the individual had used alcohol to reduce pain in the past month. Frequency of alcohol consumption was determined based on how often participants consumed alcoholic drinks per week. Quantity of alcohol consumption was measured by asking participants the largest amount of alcohol consumed on one day in the past month. Individuals with no alcohol consumption in the past year prior to the study were considered abstainers. | Participants were asked about pain in the last 12 months. |
|
| |||||||
|
| US | Observational, longitudinal | 1998-2008 | 3105 men aged 50-65 years in 1998 who completed at least 3 interviews from 1998 to 2008 | A history of frequent pain significantly increased the likelihood that older men would report decreasing alcohol consumption (vs at-risk drinking) at follow-up (OR = 1.83, 95% CI: 1.17-2.88). A history of frequent pain also significantly increased the likelihood that older men would report decreasing alcohol consumption (vs moderate drinking) at follow-up (OR = 1.63, 95% CI: 1.12-2.37). | Participants that indicated recent drinking were asked about drinking habits in the past 3 months: which days of the week individuals drink on average, how many drinks are consumed on those days, and if more than 4 drinks were consumed on one occasion. | Participants were asked if they were often troubled by pain. |
|
| US | Observational, longitudinal | Not reported | 1291 adults aged 55-65 who reported at least occasional alcohol use and had contact with outpatient clinics within the past 3 years | Baseline number of painful medical conditions alone had no effect on the 10-year pattern of decline in drinking problems. However, interpersonal spouse/partner resources moderated the effect of painful medical conditions on 10-year change in drinking frequency, such that, among individuals with more spouse/partner resources, having more painful medical conditions at baseline hastened decline in drinking frequency, whereas they had no effect on drinking frequency of individuals with fewer spouse/partner resources. Age also moderated the relationship between baseline painful medical conditions and 10-year change in frequency of drinking problems, with painful conditions hastening the decline in drinking problem frequency in the slightly older (ie, age 61-65 at baseline) participants but having no effect in the younger (age 55-60) participants. |
Frequency of drinking was determined using 3 questions from the Health and Daily Living Form about weekly consumption of wine, beer, or distilled spirits in the last month. This was asked at baseline, 1-year, 4-year, and 10-year follow-ups. Frequency of drinking problems was assessed using the Drinking Problem Index. | Painful medical conditions were assessed using items in the health stressors subscale from the Life Stressors and Resources Inventory (LISRES). Participants were asked if they had experienced painful medical conditions (including back pain, chest pain, headache, stomach pain, and joint pain) in the past year. |
|
| US | Observational, longitudinal | 1998, 2000, 2002, 2004 | 5446 adults aged 55-65 | More numerous painful medical conditions had no effect on the 8-year rate of change in participants’ likelihood of consuming alcohol. Effects of baseline pain severity and pain interference followed a similar pattern. That is, more severe pain and pain interference at baseline were each associated with lower likelihood of consuming alcohol at baseline. More severe pain at baseline predicted a slightly increased rate of decline in the amount of alcohol consumed over the next 8 years among participants who drank. With respect to drinking frequency, having more numerous painful medical conditions, more severe pain, and more debilitating pain at baseline were each associated with a lowered likelihood of drinking alcohol more often than once a week. Among individuals who drank at least weekly, all of the baseline pain predictors were associated with lower frequency of drinking, and all of them contributed to a faster rate of decline over the 8-year interval in weekly frequency of alcohol consumption. |
Amount of alcohol was defined as the number of drinks per day consumed by participants, on days they drank, during the last 3 months. Frequency of alcohol consumption was defined as the number of days per week that alcohol was consumed, during the last 3 months. |
Participants were asked about the number of experienced painful medical conditions (chest, joint, headache, or back pain) since their last HRS assessment. Pain severity asked how severe pain was at the time of study interview (from no pain to severe pain). Pain interference was a dichotomous question asking participants about the difficulty to perform their usual activities due to pain. |
- —National Institute on Aging10.13039/100000049
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPain Management and Opioid Use · Opioid Use Disorder Treatment · Substance Abuse Treatment and Outcomes
Introduction
Pain and alcohol use are highly prevalent and associated with detrimental health effects among older adults.1-4 Chronic pain (pain persisting longer than 3 months) affects 38% of adults aged ≥65 years,4 and contributes to suffering, disability, social isolation, poorer aging outcomes, and cognitive decline.5-7 Alcohol is the most commonly used substance among older adults.1-3 Of particular concern to older adults are hazardous alcohol use (ie, drinking that increases risk for harmful consequences, though specific thresholds vary across studies and contexts8) and alcohol use disorder (AUD; ie, a condition characterized by an impaired ability to stop or control alcohol use despite adverse social, occupational, or health consequences). These patterns of drinking impede healthy aging by increasing functional impairment and risk for morbidity and mortality from numerous chronic and serious illnesses (eg, cardiovascular disease, liver cirrhosis, cancer, pancreatitis).9-11 Despite this, rates of hazardous drinking and AUD have increased substantially among older adults in recent years.9^,^12
Moreover, most older adults with pain consume alcohol, and up to 28% of older adults with pain engage in hazardous patterns of alcohol use.13 One recent analysis of Health and Retirement Study data revealed that over a quarter of adults aged ≥65 with persistent or recurrent pain reported drinking alcohol at least once per week, with nearly half of these individuals engaging in hazardous patterns of drinking.14 Other studies have revealed that rates of hazardous drinking are higher in older adults with (vs without) pain,15-18 although the evidence is somewhat inconsistent.13 Nonetheless, these findings are concerning, given that pain and hazardous drinking may combine to produce synergistic burdens on individuals, providers, and healthcare systems.19^,^20
Indeed, an established reciprocal model of pain and substance use posits that pain and alcohol use interact in the manner of a positive feedback loop, resulting in the onset, progression, and maintenance of both chronic pain and hazardous alcohol use over time.19 Research in this area is typically divided into 2 directions of empirical inquiry: (1) the effects of alcohol use on pain and (2) the effects of pain on alcohol use. In terms of the effects of alcohol use on pain, although alcohol confers acute analgesic effects,21 overtime, alcohol use can lead to increased pain severity, pain-related physical impairment, and the exacerbation of chronic pain.19^,^22^,^23 In terms of the effects of pain on alcohol use, pain can be a potent motivator of alcohol use,24^,^25 and people often report using alcohol for pain relief.26
Although a number of prior reviews have examined relationships between pain and alcohol use,19-21^,^27^,^28-31 none of these papers examined bidirectional relationships between pain and alcohol use among older adults, specifically. Older adults warrant specific empirical attention.32 High rates of multimorbidity and polypharmacy among older adults33^,^34 may influence bidirectional pain-alcohol effects. Moreover, age-related physiological changes in pharmacodynamics and pharmacokinetics35-37 increase sensitivity to alcohol and lead to higher blood alcohol concentration in response to an equivalent alcohol dose.38-40 Consequently, older (vs younger) adults are at greater risk for experiencing adverse alcohol-related effects,38^,^41^,^42 and it is possible that comparatively low levels of alcohol may exacerbate medical conditions, such as chronic pain, among this population.39
The objective of this paper is to examine what is known about bidirectional relationships between pain and alcohol use among older adults. We conducted a larger scoping review examining interrelationships between pain and alcohol use in older adults. This paper describes findings from studies in older adults that examined the effects of alcohol use on pain (eg, acute analgesic effects of alcohol as a risk factor for developing chronic pain), or the effects of pain on alcohol use (eg, pain as a motivator of alcohol use, use of alcohol for pain coping, and pain as a risk factor for developing alcohol-related disorders).
Methods
We conducted a scoping review following the Joanna Briggs Institute (JBI) methodological guidance for scoping reviews.43 Methods are reported in accordance with the PRISMA extension for scoping reviews (PRISMA-ScR44). The scoping review was preregistered45 and aimed to answer 4 primary research questions: (1) What has been estimated to be the prevalence of co-occurring pain and alcohol use among older adults?; (2) What is known regarding the effects of pain on alcohol use among older adults?; (3) What is known regarding the effects of alcohol use on pain among older adults?; and (4) What interventions have been developed/used to address co-occurring pain and alcohol use among older adults?. Evidence related to the first research question has been reported elsewhere.13 The current paper describes evidence related to the bidirectional relationships between pain and alcohol use in older adults (research questions #2 and #3).
Eligibility criteria
Eligibility criteria for the larger scoping review have been described elsewhere.45 In brief, we considered human studies that defined their sample as “older”, “geriatric”, “elder”, or “aged” adults. Though this search strategy was intended to prioritize samples of individuals who were aged 65 years and older (eg, the MeSH term “aged” is defined as “a person 65 years of age or older”), we did not exclude studies based on the specific age cutoff used. This decision was made for two primary reasons. First, the definition of “older adult” remains debated in the literature, and cutoffs vary widely across settings and are influenced by social, cultural, and economic factors. Second, given the nascent state of the literature, we elected to take a more inclusive approach since strict age thresholds could exclude potentially relevant studies. For this paper, we included studies that reported the effects of alcohol use on pain (eg, acute analgesic effects of alcohol, alcohol as a risk factor for the development or worsening of chronic pain) or the effects of pain on alcohol use (eg, pain as a motivator of alcohol use, use of alcohol for pain coping, pain as a risk factor for the development or worsening of alcohol use and related disorders). We included studies that utilized a range of measures to assess pain and alcohol use, as there was substantial heterogeneity in how these constructs are assessed across studies. Our goal was to ensure a comprehensive and inclusive review that captures the breadth of the existing literature, rather than limit findings based on measurement variability.
Types of sources
Primary literature, including analytical observational studies, descriptive observational studies, experimental and quasi-experimental study designs, and qualitative studies was considered for inclusion. We excluded case series and individual case reports to reduce potential bias in findings. We also excluded secondary literature, letters to the editor, commentaries, essays, conference abstracts, conference papers, books, book reviews, and book chapters.
Search strategy
The search strategy was informed by research questions and developed in consultation with content experts and a medical librarian. The search strategy aimed to identify studies published in English without date restriction using keywords and subject terms. Databases searched included Ovid Medline, Web of Science Core Collection, PsycInfo, Embase, CINAHL, and Cochrane Central Register of Controlled Trials. The search was initially conducted in February 2023 and was updated in April 2024. Details regarding the search strategy can be found in Supplementary Appendix 1.
Study selection
All identified citations were uploaded into Covidence for screening.46 Duplicates were removed. Two independent reviewers screened titles and abstracts using the predetermined eligibility criteria. Articles that were identified as potentially suitable for inclusion by at least one of the reviewers were reviewed in full. Exclusion justification of full texts that did not meet the inclusion criteria were recorded. Disagreements were resolved through discussion and/or with an additional reviewer.
Data extraction
Two independent reviewers extracted data using a template developed by the authors. Discrepancies were resolved by discussion and consensus between reviewers, with involvement of a third team member to resolve disagreements when necessary. Items extracted included: study information (authorship, publication date, etc.), study design, demographics (age, gender, race/ethnicity), and all key findings relevant to the review questions.
Results
Sources of evidence
Figure 1 displays the flow diagram for this scoping review. We identified 6637 studies for screening. Of these, 6 additional duplicates were identified and removed. Thus, we reviewed titles and abstracts for 6631 studies. We assessed 194 full texts for eligibility, and 132 did not meet eligibility criteria. Of the 62 studies determined to meet eligibility criteria for the larger scoping review, 16 studies addressed review questions #2 and #3 (ie, “What is known regarding the effects of alcohol use on pain among older adults?” and “What is known regarding the effects of pain on alcohol use among older adults?”). We elected to exclude 1 additional paper from this review47 because, although the population was initially described as comprising “aging adults” (thus, we initially felt it met eligibility criteria as described above), those aged 40 and older were included and the “Discussion section” referred to the population generically as “middle-aged and older adults”. Thus, a total of 15 studies were included in the current paper. Of these, 5 studies reported the effects of alcohol use on pain among older adults, 8 studies reported the effects of pain on alcohol use among older adults, and 2 studies reported both.
PRISMA flow diagram.
Effects of alcohol use on pain in older adults
Table 1 shows results of studies examining the effects of alcohol use on pain in older adults.
Acute analgesic effects of alcohol
Two studies reported the acute pain-relieving effects of alcohol among older adults.48^,^49 First, in a descriptive cross-sectional study (involving a postal questionnaire and structured personal interviews) of 294 adults aged ≥75 years who had chronic pain and were in need of help to manage activities of daily living, those living at home reported that alcohol was somewhat helpful for pain management.49 In contrast, those living in special accommodations (eg, nursing homes, group-dwellings) reported that alcohol was very helpful for pain management, identifying drinking as one of the two most effective methods for pain management. A more recent study collected ecological momentary assessment data from 55 adults aged ≥50 years who had HIV and chronic pain and screened positive for at-risk substance use.48 Daily reports of using alcohol to cope with pain did not predict self-reported daily reports of relief from pain (“How much relief did doing the [coping activity/activities] provide?”).
Alcohol as a risk factor for pain
Five studies examined alcohol as a risk factor for chronic pain, with mixed findings. A longitudinal study of 1685 older men ≥70 in Australia found that the odds of reporting persistent pain at 2-year follow-up increased by 10% with each additional alcoholic drink per week.50 In contrast, a study of 2631 older adults (≥50 years) in the UK revealed that those who developed chronic pain over a 10-year follow-up period were less likely to have consumed alcohol on 5 or more days per week at baseline.51 Several other studies found no association between alcohol use and risk for developing pain. First, using clinical and administrative data obtained from clinical encounters during the years of 1998-2006 at the US Department of Veterans Affairs (VA), alcoholism (determined based on administrative codes) was not a significant risk factor for incident musculoskeletal pain among 26 545 US veterans aged ≥65 treated for a vertebral or hip fracture.52 Second, a Finnish study of 1954 adults explored variables associated with odds that a participant would remain pain-free over the course of a 10-year follow-up period.53 Weekly alcohol consumption (assessed using the Alcohol Use Disorders Identification Test consumption questions) was not associated with pain status. Third, a US study of 6132 older adults (age ≥65) with moderate to severe chronic pain revealed that frequency of alcohol consumption was not associated with risk for developing moderate to severe chronic pain.54 However, consuming alcohol on more days per week was associated with greater odds of recovery from high-impact chronic pain within 2 years, after adjusting for sociodemographic variables and the duration of previous high-impact chronic pain.
Effects of pain on alcohol use in older adults
Table 2 shows results of studies examining the effects of pain on alcohol use.
Pain as a motivator of alcohol use
One study examined pain as a motivator of drinking among 55 US adults aged ≥50 years who had HIV and chronic pain.48 Ecological momentary assessment methods were used to obtain once-daily assessments of past 24-hour pain and substance use (alcohol, cannabis, or other drug use). Results indicated that reports of any pain in the last 24 hours did not predict same-day alcohol use (number of alcoholic beverages consumed). However, daily rating of worst pain in the last 24 hours was a significant predictor of alcohol consumption, such that for every one-unit increase in worst pain beyond an individual’s personal mean, alcohol use increased by a quarter drink.
Use of alcohol to cope with pain
Six studies examined alcohol use for pain coping. One qualitative study conducted among 20 older adults (age ≥60) in Nepal revealed that older adults often report drinking to reduce pain.55 Quantitative work has found similar patterns, with one study revealing that over 1 in 5 older adults use alcohol for pain coping.56 Specifically, this study included 719 adults aged 55-65 with a history of alcohol use (individuals who had never consumed alcohol in their lives were excluded) who were recruited from the community in a western part of the United States. Although there was a significant rise in the proportion of individuals who abstained from alcohol over time, a total of 20% and 22% of older adults reported using alcohol to manage pain at the 10-year and 20-year follow-ups, respectively. Similarly high rates of alcohol use for pain coping were observed among a sample of 1634 community-dwelling adults aged ≥65 in the US state of Florida.57 Indeed, 13% reported drinking alcohol for jaw joint pain, 24% for face pain, 16% for oral sores, 14% for burning mouth, and 22% for toothache.
However, two other studies revealed lower rates of drinking for pain coping.49^,^58 One of these was a study of 294 Swedish adults aged >75 who have chronic pain, which found that only 3% of people living at home and 2% of people living in special accommodation reported using alcohol for pain management.49 Moreover, 4% of those living alone and 2% of people living with someone reported using alcohol to manage pain. The other study evaluated the factor structure of the Pain Medication Questionnaire, which includes an item asking participants to rate how often the following statement applies to them on a scale ranging from 0 (never) to 4 (always): “At times, I drink alcohol to help my pain”.58 Among 150 older adults (mean age = 72.7) recruited from pain management clinics and receiving opioid medications, the mean score on this item was 0.13, with both the median and mode equal to 0, indicating that participants generally denied using alcohol for pain relief.
There is also some evidence that the use of alcohol for pain coping may vary as a function of sex, engagement in hazardous alcohol use, and pain severity. For example, the aforementioned study of 1634 community-dwelling adults aged ≥65 in the US state of Florida found that male older adults are significantly more likely to report self-treating with alcohol than females for jaw joint, face pain, painful oral sores, and toothache pain.57 In addition, in a study of 401 adults aged 55-65, 37.9% of men who reported at least one drinking problem (eg, being intoxicated or drunk, alcohol dependence, or withdrawal) also reported using alcohol to manage pain, compared to 15.1% of those who did not report drinking problems.59 Similarly, 37.9% of women who reported drinking problems reported using alcohol to manage pain, compared to 12.5% of those who did not. Among those with moderate to very severe pain, 56.5% of men and 58.6% of women who reported drinking problems reported using alcohol to manage pain. Among both men and women, more bodily pain and more drinking problems at baseline were independent predictors of the use of alcohol to manage pain.
Pain as a risk factor for developing alcohol-related disorders
Three studies examined pain as a risk factor for the onset, progression, and maintenance of alcohol use and related disorders. In a longitudinal study of 1291 US adults aged 55-65 who reported at least occasional alcohol use, baseline number of painful medical conditions alone had no effect on the 10-year pattern of decline in drinking problems.60 However, interpersonal spouse/partner resources moderated the effect of painful medical conditions on 10-year change in drinking frequency, such that, among individuals with more spouse/partner resources, having more painful medical conditions at baseline hastened decline in drinking frequency, whereas they had no effect on drinking frequency of individuals with fewer spouse/partner resources. Age also moderated the relationship between baseline painful medical conditions and 10-year change in frequency of drinking problems, with painful conditions hastening the decline in drinking problem frequency in older (ie, age 61-65 at baseline) participants, but having no effect in younger (age 55-60) participants.
In a second study of 5446 US adults aged 55-65, more numerous painful medical conditions had no effect on the 8-year rate of change in participants’ likelihood of consuming alcohol.16 Effects of baseline pain severity and pain interference followed a similar pattern. That is, more severe pain and pain interference at baseline were each associated a with lower likelihood of consuming alcohol at baseline. More severe pain at baseline predicted a slightly increased rate of decline in alcohol consumption over the next 8 years among participants who drank. With respect to drinking frequency, having more numerous painful medical conditions, more severe pain, and more debilitating pain at baseline were each associated with a lowered likelihood of drinking alcohol more often than once a week. Among individuals who drank at least weekly, all of the baseline pain predictors were associated with lower frequency of drinking, and all of them contributed to a faster rate of decline over the 8-year interval in weekly frequency of alcohol consumption.
Finally, in a third study of 3105 men aged 50-65 who participated in the Health and Retirement Study, a history of frequent pain significantly increased the likelihood that older men would report decreasing alcohol consumption (vs moderate or at-risk drinking) at follow-up.61
Discussion
This scoping review identified 15 studies describing interrelationships between pain and alcohol use among older adults. In the sections that follow, we discuss: (1) the state of the extant literature on bidirectional relationships between pain and alcohol use in older adults; (2) potential third variables that may influence these relationships; (3) clinical implications; and (4) limitations of the current evidence and directions for future research.
Bidirectional relationships between alcohol use and pain in older adults
Results of this review extend research on bidirectional associations between pain and alcohol use to older adults. Although some findings from this review of older adults align with the reciprocal model of pain and addiction,19 we also observed key differences, which suggest that the interplay between pain and alcohol may differ between older versus younger adults and underscores the need for targeted research in the older adult population.
Effects of alcohol use on pain
Consistent with evidence of acute analgesic effects among general adult populations,21 one study found that older adults often report that alcohol is helpful for pain management.49 However, a more recent study conducted among a small sample of older adults with HIV found that using alcohol to cope did not predict pain relief.48 Although one possible interpretation of this finding is that alcohol may not provide meaningful analgesic effects in this specific population, it is also important to note that alcohol may reduce pain acutely without improving overall coping or perceptions of “relief”. Notably, no studies experimentally tested the analgesic effects of alcohol in older adults, specifically, despite prior calls for research examining the effects of age on acute alcohol analgesia.21 Moreover, no studies examined the effects of acute alcohol abstinence on pain in older adults, despite reason to believe that pain reactivity may be exacerbated during alcohol withdrawal.19^,^62 Additional work is needed to systematically manipulate alcohol intoxication/deprivation to test the effects on pain reactivity in older adults.
In general adult samples, heavy alcohol use is associated with an increased risk for the onset, worsening, and maintenance of chronic pain,31^,^63^,^64 however, the current review identified mixed evidence in older adults. Although one study found that each additional alcohol drink per week increases an older person’s odds for poorer pain outcomes by ∼10%,50 another study found that alcohol use may instead be associated with a lower likelihood of chronic pain,51 and several studies found no association between alcohol use and chronic pain.52-54 Given that the relationship between alcohol consumption and the development of pain may be curvilinear,20 it is possible that the statistical models used in these studies did not fully capture the complexity of this relationship or identify levels of consumption at which the direction of effects changes. Indeed, there is reason to believe that hazardous alcohol consumption would increase the risk for the development and worsening of chronic pain in older adults. One prior study of older adults with HIV and chronic pain found that higher daily alcohol consumption predicted greater ratings of daily worst pain (ie, pain at its worst in the past 24 hours), suggesting that alcohol use may contribute to heightened pain severity.48 There is also evidence that heavy drinking can contribute to pathological changes to neural structures (eg, amygdala, prefrontal cortex, insula), perpetuated allostatic load in pain neurocircuitry, and central opioid deficiency.19^,^20 In addition, alcohol can reduce the effectiveness of pain treatments (eg, pharmacological/surgical interventions) through substance-specific (eg, cross-tolerance) and general neurobiological (eg, allostatic load) effects.19^,^20 Longitudinal studies that determine how various levels and patterns of alcohol consumption affect the development of chronic pain, utilization/effectiveness of pain treatments, and pain trajectories over time are needed.
Effects of pain on alcohol consumption
There is evidence that pain motivates alcohol use in older adults, with one study showing that for every one-unit increase in worst pain beyond an individual’s mean, alcohol use increases by a quarter drink.48 This finding is consistent with experimental findings that pain induction (vs a no-pain control condition) increases alcohol consumption.24 However, prior experimental work excluded participants aged 65 and older, thus, additional research is still needed to test pain as a causal motivator of alcohol consumption among older adults. In line with the hypothesis that pain can motivate alcohol use among older adults, the current review identified several studies suggesting that older adults often use alcohol for pain coping. Indeed, as many as 1 in 5 older adults use alcohol for pain coping.56 This finding is particularly alarming because individuals who rely more on alcohol to manage pain drink more frequently and in heavier amounts, report more warning signs of negative consequences of alcohol consumption, and have more drinking problems.56 Though one study found that older adults generally denied using alcohol for pain coping,58 it is important to note that this study comprised solely of patients receiving prescription opioids, who may be more likely to underreport alcohol use due to concerns about jeopardizing their access to pain medication.
Despite reason to believe that pain may contribute to the onset, progression, and maintenance of alcohol use/related disorders and interfere with alcohol cessation, only 3 studies examined this hypothesis. Moreover, each of these studies found that pain may actually be associated with a decline in drinking frequency among older adults.16^,^60^,^61 These findings differ from those observed in general adult samples, which have found that greater pain and pain-related functional impairment are associated with an increased likelihood of escalating from alcohol use to AUD.65 Moreover, evidence derived from general adult samples suggests that pain is associated with poorer rates of abstinence, drinking lapses, and greater post-intervention alcohol consumption.66-68 It is possible that older adults with pain are more likely to receive advice from their medical providers to reduce or quit drinking, and that this may explain the inverse association observed between pain and alcohol use in this population. It is also possible that high rates of comorbid medical conditions and concomitant medications in older adults69 may further influence the effects of pain on alcohol use in this population. Additional comparative studies are needed to examine differences in older versus younger cohorts with more attention to comorbid conditions.
Third variables
Prior work has underscored the importance of considering third variables, including sociodemographic factors and comorbid psychopathology, when examining interrelations between pain and alcohol use.19^,^20 Two studies identified in this review examined gender differences in the use of alcohol for pain coping, with one study finding that older men are more likely than women to report using alcohol to cope with pain,57 and another finding no gender-specific effects in use of alcohol for pain coping.59 Another study examined the moderating effects of demographic characteristics (ie, age, gender, race, marital status, education, income) on relationships between pain and alcohol use in older adults.16 This study revealed that, although overall alcohol use declined among study participants from 1996 to 2004, older adults who were African American and/or reported lower income were less likely to follow this trend when experiencing greater pain severity or interference. Aside from these 3 exceptions, most studies did not examine the role of sociodemographic factors or comorbid psychopathology. Instead, many accounted for these factors by including them as covariates in statistical analyses.50-54^,^59-61 Although covariation can help to clarify unique variance in bidirectional pain-alcohol relations, it does little to clarify whether these variables function as underlying mechanisms driving these associations.
It is also likely that there are third variables underlying pain-alcohol comorbidity that are unique to older adults. For example, complex interactions among multimorbidity, pain, and alcohol use are particularly salient in later life, as 80% of those aged ≥65 have ≥2 chronic conditions.33 It is possible that older adults with multiple health conditions may reduce their drinking due to medical advice or the “sick quitter” effect. Alternatively, these same conditions may exacerbate pain and increase the perceived need to use alcohol to cope. Although several studies included in this review controlled for comorbid conditions or number of comorbidities,50^,^51^,^54^,^56 none explicitly examined these factors as mediators or moderators of pain–alcohol associations. Similarly, no studies explored the role of cognitive function, which is surprising given that cognitive decline could alter risk perception, coping strategies, and the capacity for self-regulation in both pain and alcohol use contexts.70
Loneliness and social isolation also warrant attention as potential third variables. One study included in this review found that living alone (vs living with someone) did not influence the use of alcohol for pain management,49 and another controlled for social isolation in examining risk factors for chronic pain.51 Additional work is clearly needed to better understand how social isolation influences associations between pain and alcohol use.
Additional work is also needed to explore the role of drinking history. Older adults often have complex drinking histories, including the potential for prior alcohol-related diagnoses, treatment histories, or long-term abstinence, all of which may shape current pain coping behaviors and the effects of alcohol use on pain outcomes. One study included in this review found that problem drinking was associated with a greater likelihood of using alcohol to manage pain,59 and another controlled for history of alcohol problems.61 Future research is needed to more comprehensively assess lifetime alcohol use patterns, including history of alcohol use, treatment, and periods of abstinence, to better understand how these trajectories relate to current experiences of pain and drinking behavior in older adults.
Finally, prior research has highlighted the importance of identifying transdiagnostic factors that may influence bidirectional pain-alcohol effects and represent promising targets for intervention development.71 Notably, several transdiagnostic constructs have emerged as promising candidates, including anxiety sensitivity, distress intolerance, pain-related anxiety, and pain catastrophizing. For instance, pain-related anxiety has been linked to greater alcohol-related consequences and an increased likelihood of alcohol-opioid co-use among adults with chronic low back pain.72 However, despite their theoretical and empirical relevance, none of the studies included in this review examined the potential role of these transdiagnostic factors in shaping bidirectional pain–alcohol associations.
Clinical implications
Despite mixed findings and the need for additional research, results from this scoping review suggest that pain and alcohol use share a complex and nuanced relationship that should be considered when treating either condition. Clinicians working with older adults should assess both pain (eg, chronic pain status, pain intensity, physical impairment) and alcohol use when providing treatment for either condition. In the context of alcohol use, pain and related factors should be monitored throughout treatment. In the context of pain, it is important to consider patterns of alcohol use when evaluating and treating clinical pain. It will also be important for future research to prioritize the development and refinement of integrated intervention strategies that address co-occurring pain and alcohol use specifically in older adults. Although initial work has found that age-tailored substance use interventions may simultaneously lead to reductions in alcohol use and pain,73 additional work is still needed.
Limitations and future research directions
An important limitation of this scoping review is the heterogeneity of the included studies in terms of age-related eligibility criteria. Because we did not apply strict age cutoffs, our sample encompassed studies with varying definitions of “older adults”, with the majority of studies (56%) including samples that were not limited to those aged 65 and older. Our decision to use a more inclusive search strategy was informed by evidence that aging-related vulnerabilities may be influenced by social, cultural, and economic factors and emerge earlier in populations with chronic conditions such as cancer or HIV, and by our desire to capture a broad range of evidence given the nascent state of research in this area. However, this approach introduced variability as there was substantial heterogeneity of the populations represented across studies. Indeed, younger cohorts of older adults (eg, those aged 50–64) may differ in important ways from those aged 65 and older, including potential differences in employment status, functional abilities, social roles, and health-related factors. These factors could meaningfully influence the relationship between chronic pain and alcohol use and thus warrant further exploration. Furthermore, although some included studies recruited participants for whom biological aging may occur earlier (eg, due to chronic illness), additional research is still needed to examine the differential effects of biological age (ie, a marker of aging that considers biological and physiological development factors, such as genetics, lifestyle, and comorbidities) and chronological age (ie, the amount of time a person has been alive) on bidirectional effects of pain and alcohol use. Additional work should also prioritize the recruitment of individuals who fall within the National Institutes of Health’s categorization of older adults (ie, aged ≥65).
Several additional limitations of this scoping review should be noted. First, there was significant heterogeneity in terms of how alcohol use (eg, current use, frequency, quantity, hazardous use) and pain (eg, pain ratings, chronic pain status, pain interference) were defined and assessed across studies, which poses challenges in comparing findings across studies and in drawing generalizable conclusions. Future research must prioritize the use of consistent, well-defined, validated measurement strategies. Additional research should also seek to understand how pain type, duration, and location may influence its relations with alcohol use. Second, generational differences can substantially influence attitudes, norms, and behaviors related to substance use.74 In addition to generational cohort effects, year of data collection may have also influenced study findings. For example, the Coronavirus disease 2019 (COVID-19) pandemic was associated with higher rates of anxiety/depression, social isolation, and loneliness,75-77 all of which are known risk factors for both chronic pain and alcohol use in older adults.78^,^79 Future research should explicitly account for generational cohort and period effects when examining pain and alcohol use in older adults. Third, we elected to include studies conducted across the world. However, there were not enough studies identified to examine cross-cultural differences. Given the potential influence of cross-cultural variance in drinking norms, motives, and behaviors80 and pain prevalence, beliefs, and coping responses,81-83 additional work is needed to determine whether differences in bidirectional pain–alcohol associations exist as a function of country/culture/context. Fourth, longitudinal studies examining interrelationships between pain and alcohol use may be affected by attrition due to mortality, and attrition may be even greater among older adults who have histories of heavier drinking, more severe pain, and multimorbidity. This has the potential to bias results and limit generalizability. Despite these limitations, the current scoping review represents an important contribution to the growing literature on bidirectional relationships between pain and alcohol use among older adults.
Supplementary Material
glaf258_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kuerbis A. Substance use among older adults: an update on prevalence, etiology, assessment, and intervention. Gerontology. 2020;66:249-258. 10.1159/00050436331812954 · doi ↗ · pubmed ↗
- 2Kuerbis A , Sacco P, Blazer DG, Moore AA. Substance abuse among older adults. Clin Geriatr Med. 2014;30:629-654. 10.1016/j.cger.2014.04.00825037298 PMC 4146436 · doi ↗ · pubmed ↗
- 3Moore AA , Karno MP, Grella CE, et al. Alcohol, tobacco, and nonmedical drug use in older U.S. Adults: data from the 2001/02 national epidemiologic survey of alcohol and related conditions. J American Geriatrics Society. 2009;57:2275-2281. 10.1111/j.1532-5415.2009.02554.x · doi ↗
- 4La Rowe LR , Miaskowski C, Miller A, et al. Prevalence and sociodemographic correlates of chronic pain among a nationally representative sample of older adults in the United States. J Pain. 2024;25:104614. 10.1016/j.jpain.2024.10461438936750 PMC 11402580 · doi ↗ · pubmed ↗
- 5Domenichiello AF , Ramsden CE. The silent epidemic of chronic pain in older adults. Prog Neuropsychopharmacol Biol Psychiatry. 2019;93:284-290. 10.1016/j.pnpbp.2019.04.00631004724 PMC 6538291 · doi ↗ · pubmed ↗
- 6Wilkie R , Tajar A, Mc Beth J. The onset of widespread musculoskeletal pain is associated with a decrease in healthy ageing in older people: a population-based prospective study. P Lo S One. 2013;8:e 59858. 10.1371/journal.pone.005985823555810 PMC 3612101 · doi ↗ · pubmed ↗
- 7Whitlock EL , Diaz-Ramirez LG, Glymour MM, Boscardin WJ, Covinsky KE, Smith AK. Association between persistent pain and memory decline and dementia in a longitudinal cohort of elders. JAMA Intern Med. 2017;177:1146-1153. 10.1001/jamainternmed.2017.162228586818 PMC 5588896 · doi ↗ · pubmed ↗
- 8Saunders JB , Aasland OG, Babor TF, de la Fuente JR, Grant M.II. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption. Addiction. 1993;88:791-804. 10.1111/j.1360-0443.1993.tb 02093.x 8329970 · doi ↗ · pubmed ↗