The association between hearing impairment and incident depression in older adults: a longitudinal analysis
Malcolm P Forbes, Mark W Cox, Katharine Brewster, Mojtaba Lotfaliany, Mohammadreza Mohebbi, Gary Rance, Robyn L Woods, Carlene Britt, John J Mcneil, Michael Berk

TL;DR
Older adults with moderate to severe hearing loss are at higher risk for depression, but this risk is reduced with regular hearing aid use.
Contribution
This study longitudinally links time-varying hearing measures to incident depression and shows hearing aid use reduces depression risk.
Findings
Moderate to severe hearing loss increases depression risk (adjusted HR: 1.24) in older adults.
Hearing aid use for ≥6 hours/day reduces depression risk (adjusted HR: 0.65) in those with hearing loss.
Abstract
Hearing loss (HL) is common in older adults and is associated with several adverse health outcomes. Although previous research has demonstrated a link between hearing impairment and depression, most studies have been cross-sectional or relied on a single baseline measure of hearing. To investigate the association between longitudinal, time-varying audiometric measures of hearing and incident depression in older adults. A secondary aim was to assess whether hearing aid use modifies this association over time in those with moderate to severe HL. We included 1260 participants who underwent pure-tone audiometry at baseline, 18 months, and 36 months. Depression was defined using the CES-D-10 scale, with a cut-score of ≥8. Cox proportional hazards analyses were used to examine the link between hearing status (normal, mild HL, moderate/severe HL) and depression, adjusted for demographic,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
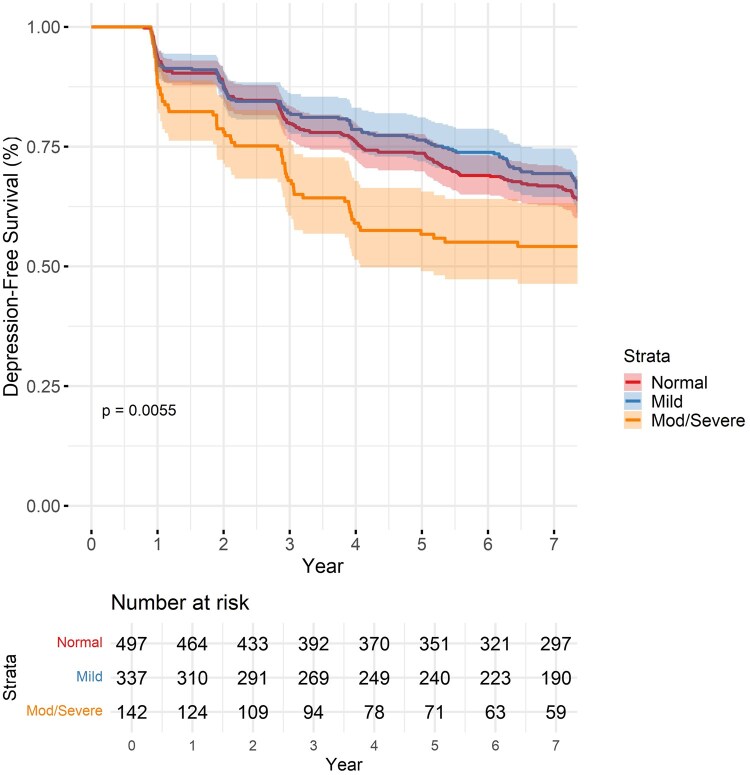 Figure 1
Figure 1|
|
|
|
| |
|---|---|---|---|---|
|
| 73.4 (3.17) | 74.9 (4.45) | 76.5 (4.94) | 74.4 (4.10) |
|
| ||||
|
| 257 (40.5) | 248 (56.8) | 98 (51.9) | 603 (47.9) |
|
| 377 (59.5) | 189 (43.2) | 91 (48.1) | 657 (52.1) |
|
| ||||
|
| 178 (28.1) | 122 (27.9) | 70 (37.0) | 370 (29.4) |
|
| 454 (71.6) | 313 (71.6) | 119 (63.0) | 886 (70.3) |
|
| ||||
|
| 16 (2.5) | 20 (4.6) | 4 (2.1) | 40 (3.2) |
|
| 241 (38.0) | 199 (45.5) | 78 (41.3) | 518 (41.1) |
|
| 377 (59.5) | 218 (49.9) | 107 (56.6) | 702 (55.7) |
|
| ||||
|
| 521 (82.2) | 364 (83.3) | 149 (78.8) | 1034 (82.1) |
|
| 31 (4.9) | 15 (3.4) | 13 (6.9) | 59 (4.7) |
|
| 82 (12.9) | 58 (13.3) | 27 (14.3) | 167 (13.3) |
|
| 333 (52.5) | 254 (58.1) | 121 (64.0) | 708 (56.2) |
|
| 94.1 (4.34) | 93.0 (4.37) | 92.7 (4.21) | 93.5 (4.36) |
|
| 3.46 (3.41) | 3.57 (3.76) | 3.51 (3.08) | 3.51 (3.49) |
|
| 70 (11%) | 52 (11.9%) | 24 (12.7%) | 146 (11.6%) |
|
| 74 (11.7) | 54 (12.4) | 20 (10.6) | 148 (11.7) |
|
| 107 (16.9) | 97 (22.2) | 37 (19.6) | 241 (19.1) |
|
| 14 (2.2) | 94 (21.5) | 139 (73.5) | 247 (19.6) |
| Normal hearing | Mild hearing loss | Moderate-severe hearing loss | |
|---|---|---|---|
|
| 19.3 (17.8-20.8) | 19.3 (17.8-20.8) | 23.9 (21.5-26.5) |
|
| 1.00 | 1.01 (0.90-1.13) | 1.24 (1.08-1.42) |
|
| 1.00 | 1.04 (0.92-1.16) | 1.25 (1.09-1.45) |
|
| 1.00 | 1.03 (0.92-1.16) | 1.24 (1.08-1.43) |
| No hearing aid use | Hearing aid use | |
|---|---|---|
|
| 23.8 (19.1-29.3) | 24.1 (21.2-27.4) |
|
| 1.00 | 1.03 (0.81-1.32) |
| < 6 h | ≥6 h | |
|---|---|---|
|
| 34.0 (26.4-43.1) | 22.0 (19.0-25.5) |
|
| 1.00 | 0.65 (0.49-0.87) |
- —National Institutes of Health10.13039/100000002
- —National Health and Medical Research Council of Australia
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHearing Loss and Rehabilitation · Vestibular and auditory disorders · Hearing, Cochlea, Tinnitus, Genetics
Introduction
Hearing loss (HL) affects more than 1.5 billion people worldwide, with more than 20% experiencing disabling hearing impairment.1 Although HL can be modified by amplification devices such as hearing aids, age-related HL typically progresses gradually, making it difficult to notice in the early stages.2 HL may lead older adults to withdraw from situations where they have difficulty hearing and communicating, contributing to isolation.3 In addition to barriers to social engagement, HL may threaten personal independence.4 Consequently, HL has been linked to a broad array of negative health outcomes, including reduced quality of life, cognitive impairment, and depression.5
A meta-analysis investigating the association between HL and depression in older adults revealed substantial study heterogeneity and mixed findings.6 Some studies have reported an increased risk of depression with HL,2^,^7-18 while others have reported no significant association.5^,^19-27 A limitation of most studies is the reliance on self-reported HL as the primary exposure measurement, rather than rigorous audiometric assessments. There is evidence that older adults with mild HL may be unaware of their impairment, leading to overestimation of their hearing abilities when self-reporting.28 Depressed older adults may be more likely to self-report HL, as late-life depression often presents in conjunction with somatic symptoms.29 Additionally, few longitudinal studies categorize HL by severity or consider the impact of hearing aid usage on depression.
There is a need for research in this area that addresses the methodological issues of the extant literature, given the prevalence and consequences of both age-related HL and depression. Evidence from regular hearing screening programs highlights the effectiveness of early detection and intervention, with auditory amplification devices improving listening ability and quality of life,30-32 as well as reducing dementia risk.33 Few studies have explored the dose–response relationship between audiometrically assessed HL and depression and whether hearing aid use can mitigate depressive symptoms. In response to this knowledge gap, this longitudinal study investigates the dose–response relationship between audiometrically assessed HL and depressive symptoms over several years and explores whether hearing aid use can mitigate these symptoms.
Methods
Study population
This study utilized data from the ASPREE (ASPirin in Reducing Events in the Elderly) trial and its extension, ASPREE-XT.34^,^35 ASPREE was an international, multicenter, randomized controlled trial designed to evaluate whether daily low-dose aspirin could prolong healthy, disability-free life in older adults by preventing age-related conditions, including cardiovascular disease, dementia, and depression. Conducted between 2010 and 2017, the trial enrolled 19 114 healthy participants aged 70 years or older (65 years for US minorities) who were free of dementia, independence-limiting physical disability, and known cardiovascular disease at the time of enrollment. Participants included 16 703 from Australia and 2411 from the United States. The ASPREE-XT extension study commenced in 2018, transitioning the cohort into a longitudinal observational study to further explore factors contributing to healthy aging, including cognitive and physical health outcomes. Participants were followed up face-to-face each year, and by telephone each 6 months. For this analysis, we focused on a subset of 1260 ASPREE participants with complete baseline data on hearing ability, depressive symptoms, and relevant covariates.36
Measures and operational definitions
Hearing ability was measured at baseline, 18 months, and 36 months and was assessed using World Health Organisation (WHO) standards for pure-tone audiometry.37^,^38 Average tone sound detection thresholds for tones at 0.5, 1, 2, and 4 kHz test frequencies in the better ear were calculated, and ears were categorized as “normal” hearing (≤25 dBHL), “mild” HL (26-40 dBHL), or “moderate to severe” HL (≥41 dBHL). We additionally classified hearing aid use as present if participants reported wearing a hearing aid in at least 1 ear, or absent if otherwise. We further assessed hearing aid use as frequent (≥6 h hearing aid use per day) or infrequent (<6 h hearing aid use per day). Incident depression was defined as a Center for Epidemiologic Studies Depression Scale 10-item (CES-D-10) score of ≥8 during the follow-up period. A cut-score of 8 was chosen to improve sensitivity in detecting depression.39 The CES-D-10 has been shown to have reliability and validity with respect to a diagnosis of depression among older adults.39 Depressive symptoms were assessed annually, and participants were followed up for a median time of 7.3 years (IQR 0.21 years).
Statistical analysis
Cox proportional hazards regression models were employed to evaluate the association between time-updating hearing ability (normal, mild, moderate/severe) and risk of developing depression (CES-D-10 ≥ 8). Hearing ability and hearing aid use were both treated as time-varying exposures, allowing participants to transition between hearing status categories or update hearing aid use across baseline, 18-month, and 3-year visits. Depression was analyzed as a recurrent event, meaning individuals who recovered (ie, had a CES-D-10 score below the threshold at subsequent visits) re-entered the risk pool, allowing additional depressive episodes to be analyzed. Start–stop intervals were created to capture these transitions over time in Cox models. In contrast, the Kaplan–Meier curves focused on time to the first depressive episode only, censoring participants at the earliest occurrence of depression onset, last known study contact, withdrawal, or death. For first-onset incidence models, the event was the first assessment with CES-D-10 ≥ 8 after baseline among those non-depressed at baseline (excluding those with CES-D-10 ≥ 8 or reporting antidepressant use at baseline). In recurrent-event models, we did not exclude those with baseline CES-D-10 ≥ 8. Covariates included in adjusted models were selected based on published evidence linking them to both HL and depression.40 These consisted of age, sex, living arrangement, educational attainment, smoking history, alcohol use, cognitive performance (modified Mini-Mental State score), body mass index, diabetes, and chronic kidney disease. These covariates were chosen based on a review of the literature, and further details on their measurement can be found in McNeil et al.34 The proportional hazards assumption was tested by examining Schoenfeld residuals, revealing no significant violations. Hazard ratios (HRs) with 95% CIs are presented, providing the time-averaged risk over the entire follow-up period, with normal hearing as the reference category. Missingness was low, with 90.5% of participants having complete data, and missingness was primarily driven by 1 variable. Missing data were handled using a complete-case approach, with participants with missing values on any exposure, outcome, or covariate excluded. All statistical analyses were conducted in R version 4.2.0.41
Subgroup analysis
In addition to the main models, we performed a subgroup analysis restricted to participants who were classified as having moderate/severe hearing impairment at any time point. Among participants classified as having moderate/severe HL at any time point, we conducted 2 pre-specified comparisons with time-updated exposures: (1) any hearing-aid use versus no use (reference = no use); and (2) among hearing-aid users, ≥6 h/day versus <6 h/day (reference ≤6 h/day). The ≥6-h threshold was defined to approximate “most-of-day” use.
Results
Baseline characteristics
The baseline characteristics of the study participants, stratified by hearing category (normal, mild, and moderate/severe HL), are presented in Table 1. Participants with moderate/severe HL at baseline were more likely to be older and living alone. Hearing aid use was reported in 2.2% of those with no pure tone audiometry impairment, 21.5% of those categorized as having mild HL, and 73.5% of those with moderate to severe HL. Baseline HHIE-S, with higher scores indicating a greater perceived hearing handicap,42 was correlated with baseline audiometry-assessed HL (Pearson’s r = 0.62 [95% CI, 0.61-0.64, P < .01]).
Depression-free survival
The Kaplan–Meier curve demonstrated depression-free survival over time, stratified by hearing impairment categories (Figure 1). It highlighted differences in survival trajectories, with individuals with moderate/severe HL exhibiting lower probabilities of remaining depression-free compared to those with mild or normal hearing (χ^2^(2) = 8.8, P = .013). In Cox proportional hazards models, moderate to severe HL was associated with an increased risk of incident depression over the follow-up period. In the fully adjusted model (Table 2), there was an adjusted HR (aHR) of 1.24 (95% CI, 1.08-1.43, P < .01). Mild HL was not significantly associated with depression risk in unadjusted or adjusted models. Complete case analysis was utilized; however, the impact of missing data was evaluated using multiple imputation, and there were no differences in the findings.
Kaplan–Meier curve of baseline hearing category and depression incidence.
In a subgroup analysis restricted to the moderate to severe HL subgroup, any self-reported use versus no use of hearing aids was not associated with incident depression (aHR = 1.03, 95% CI, 0.80-1.32) (Table 3). However, among hearing aid users, more than 6 h of self-reported use per day was associated with lower risk compared with less than 6 h of use per day (aHR = 0.65, 95% CI, 0.49-0.87) (Table 4). Modeling hours of use per day continuously showed a dose–response (aHR per hour = 0.98; 95% CI, 0.97-0.99).
Table 4.: Cox proportional hazards model for ≥ 6 versus < 6 hours of hearing aid use in subgroup with moderate to severe hearing loss.
Discussion
This prospective cohort study of 1260 older adults found that moderate to severe HL, measured using pure tone audiometry, was associated with an increased risk of incident depression after adjusting for a range of potential confounders. In the fully adjusted model, moderate/severe HL was associated with a 1.24-fold increase in depression risk over a period averaging 7.3 years. In contrast, mild HL was not significantly associated with depression risk. Notably, hearing aid use for more than 6 h per day exerted a protective effect, suggesting that consistent use of auditory amplification may mitigate the psychological consequences of HL.
This study adds to the growing body of evidence linking HL to depression in older adults. Importantly, our study is one of the few to use robust audiometric measures of hearing ability in a longitudinal cohort. These measures psychophysically determine sound detection levels, and as such, are less prone to biases associated with self-reported data.43 Previous studies, reported in recent meta-analyses,6^,^40^,^44 have largely relied on self-reported HL, which may underestimate the true prevalence of HL and its impact on mental health and may be affected by the presence of depression. By using pure tone audiometry in a longitudinal study design, our study provides the most reliable assessment of HL severity and its relationship with subsequent depression.
Our findings are consistent with prior research showing a modest association between HL and depression. Notably, the effect found in our study, which was longitudinal in nature and accounted for a range of potential confounders, was lower than previous meta-analytic estimates.6 This may relate to the sample, which was older adults eligible for a primary prevention trial. Nonetheless, our results align with research that identifies a stronger association with depression for more severe degrees of HL. For example, the findings of Powell et al.7 in the Health ABC Study, which similarly showed that older adults with moderate or greater HL had an approximately 25% higher risk of developing clinically significant depressive symptoms compared to those with normal hearing. Like Powell et al., we observed that mild HL was not consistently linked to depression risk, underscoring that the greatest vulnerability may lie among those with more pronounced impairment.
There have been mixed findings about the effects of hearing aid use on depression risk. Our study is unique in measuring the effect of self-reporting hours of hearing aid use, rather than self-reported hearing aid use as a binary outcome. Consistent with previous studies,7^,^8^,^12^,^18 our study found that self-reported hearing aid use as a yes/no response was not associated with a reduced risk of depression. However, when measured as self-reported hearing aid use for more than 6 h per day, hearing aid use was found to be protective (HR = 0.65, P = .003) in individuals with moderate to severe HL. Our finding is supported by Tsimpida et al.9 who examined longitudinal data from the English Longitudinal Study of Ageing (ELSA) and found that older adults with hearing impairment who used hearing aids experienced fewer depressive symptoms than non-users, suggesting a moderating effect of hearing aid use on the relationship between HL and depression. These benefits were more pronounced among participants with greater social or economic vulnerabilities, indicating that consistent hearing aid use may be especially protective in groups at higher risk for late-life depression. Adherence to hearing aid use is generally suboptimal, with 55.4% of people prescribed a hearing aid using them daily and only 27.3% using them >6 h a day, in 1 study.45
The beneficial effects of hearing aid use are also supported by trial evidence. Choi et al.46 found that use of a hearing aid was associated with a significant decrease in depressive symptoms at 6 months but not at 12 months, and that the most substantial improvements in depressive scores were seen in individuals who had the highest depressive symptoms at baseline. Our study suggests that the benefits of hearing aid use may extend beyond 12 months for mood symptoms. Recent randomized trial evidence further supports this, with significantly reduced depressive symptoms after 6 months in older adults offered over-the-counter hearing aids.47 Ongoing clinical trials are required to identify which groups may benefit most from hearing remediation.48
This study had several strengths and limitations. Limitations include bias due to attrition and nonresponse, a population that was free of dementia, independence-limiting physical disability, and known cardiovascular disease, which may limit generalizability. Furthermore, we classified depression using a screening tool (CES-D-10) rather than a clinician-established diagnosis. This scale assesses symptoms over the preceding week. Consequently, some cases may reflect transient affective states or context-appropriate distress rather than depressive disorder.49 Such misclassification is likely nondifferential with respect to hearing status and would bias associations toward the null, although differential reporting cannot be fully excluded. In addition, antidepressant treatment during follow-up may have influenced observed symptom trajectories. To reduce inclusion of prevalent treated depression, our first-onset analyses excluded participants with baseline CES-D-10 ≥ 8 and those using antidepressants at baseline. We did not adjust for post-baseline antidepressant use in Cox models because initiation typically follows depressive symptom emergence and thus functions as a time-varying mediator. Conditioning on this mediator would bias estimates of the total association between time-updated hearing status and incident depression.
There were several notable strengths, including the large sample size, use of audiometric measures, use of time-updating measures, modeling depression as a recurrent event, and extended follow-up period. The results provide valuable longitudinal evidence that moderate or severe HL is associated with an increased risk of depression among older adults, and notably, that hearing aid adherence may protect against this risk. By differentiating between minimal and extensive hearing aid use, our findings suggest that sporadic hearing aid use may not yield the same mental health benefit as consistent daily use of 6 h or more.
Still, questions remain about the precise mechanisms through which hearing aids may alleviate depressive symptoms, whether through improved social engagement, greater self-efficacy, or impacting biological mechanisms. Hearing loss may heighten cognitive load and alter auditory-limbic connectivity, leading to structural brain changes that impair mood regulation.50 Alternatively, shared neurodegenerative or vascular processes may contribute to both hearing decline and depression.3
Future research, including larger randomized trials in diverse populations, is necessary to pinpoint how best to optimize hearing aid use, explore barriers to consistent wear, and evaluate targeted interventions for older adults at heightened risk of depression. Ultimately, our findings underscore the importance of assessing and addressing hearing impairment as part of comprehensive geriatric care, with the potential to bolster not just communication abilities but also emotional well-being and overall quality of life in later years. Future research should investigate whether the relationship between HL and late-life depression is bidirectional, as depression may also affect adherence and response to HL treatment.
Conclusion
Moderate-severity hearing impairment is a significant risk factor for depression in older adults. Hearing aid use may reduce the incidence of late-life depression. This has important clinical implications and should lead to targeted interventions and prevention strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organisation. Deafness and hearing loss. Internet. WHO. Accessed November 26, 2024. 2024. https://www.who.int/health-topics/hearing-loss
- 2Kiely KM , Anstey KJ, Luszcz MA. Dual sensory loss and depressive symptoms: the importance of hearing, daily functioning, and activity engagement. Front Hum Neurosci. 2013;7:837. 10.3389/fnhum.2013.0083724379769 PMC 3864127 · doi ↗ · pubmed ↗
- 3Rutherford BR , Brewster K, Golub JS, Kim AH, Roose SP. Sensation and psychiatry: linking age-related hearing loss to late-life depression and cognitive decline. Am J Psychiatry. 2018;175:215-224. 10.1176/appi.ajp.2017.1704042329202654 PMC 5849471 · doi ↗ · pubmed ↗
- 4Andrade C , Pereira CR, Silva P. The silent impact of hearing loss: using longitudinal data to explore the effects on depression and social activity restriction among older people. Ageing Soc. 2017;38:2468-2489. 10.1017/S 0144686 X 17000708 · doi ↗
- 5Amieva H , Ouvrard C, Meillon C, Rullier L, Dartigues JF. Death, depression, disability, and dementia associated with self-reported hearing problems: a 25-year study. J Gerontol A Biol Sci Med Sci. 2018;73:1383-1389. 10.1093/gerona/glx 25029304204 · doi ↗ · pubmed ↗
- 6Lawrence BJ , Jayakody DMP, Bennett RJ, Eikelboom RH, Gasson N, Friedland PL. Hearing Loss and depression in older adults: a systematic review and meta-analysis. Gerontologist. 2020;60:e 137-e 154. 10.1093/geront/gnz 00930835787 · doi ↗ · pubmed ↗
- 7Powell DS , Betz JF, Yaffe K, et al Hearing loss and risk of depressive symptoms in older adults in the Health ABC study. Front Epidemiol. 2022;2:980476. 10.3389/fepid.2022.98047638455326 PMC 10910912 · doi ↗ · pubmed ↗
- 8Han JH , Lee HJ, Jung J, Park EC. Effects of self-reported hearing or vision impairment on depressive symptoms: a population-based longitudinal study. Epidemiol Psychiatr Sci. 2019;28:343-355. 10.1017/S 204579601800004529415786 PMC 6998913 · doi ↗ · pubmed ↗