Recurrent Stroke Due to Pulmonary Arteriovenous Malformation: Diagnostic Challenges and Management
Rui Pedro Ribeiro, Carolina Guimarães, Helena Hipólito Reis, Ana Aires, Ana Pastor, Luísa Fonseca

TL;DR
A rare lung condition called PAVM can cause strokes by allowing blood clots to bypass the lungs, and it was successfully treated in a patient with a special plug.
Contribution
Highlights the importance of diagnosing PAVMs as a cause of cryptogenic stroke and demonstrates effective embolization treatment.
Findings
Recurrent stroke in a patient was linked to a PAVM identified via transcranial Doppler and CT angiography.
Embolization using an Amplatzer Vascular Plug effectively treated the PAVM and resolved the right-to-left shunt.
Comprehensive investigation of RLS is essential when stroke etiology remains undetermined.
Abstract
Pulmonary arteriovenous malformations (PAVMs) are rare vascular anomalies that establish a direct right-to-left shunt (RLS). Although uncommon, they may cause paradoxical embolism leading to stroke, cryptogenic stroke, or hemorrhage. Despite their potential severity, PAVMs remain an unrecognized entity. We report a case of a 57-year-old woman with cardiovascular risk factors and a previous recurrent stroke of undetermined origin, admitted with acute right-sided weakness, dysarthria, and facial droop. Computed tomography (CT) confirmed acute infarcts in the left frontal and temporal cortices. During the diagnostic workup, transcranial Doppler with bubble contrast revealed RLS, and transesophageal echocardiography excluded an intracardiac defect. Pulmonary CT angiography identified a right lower lobe PAVM that was embolized with an Amplatzer Vascular Plug 4 (St. Paul, MN: Abbott).…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
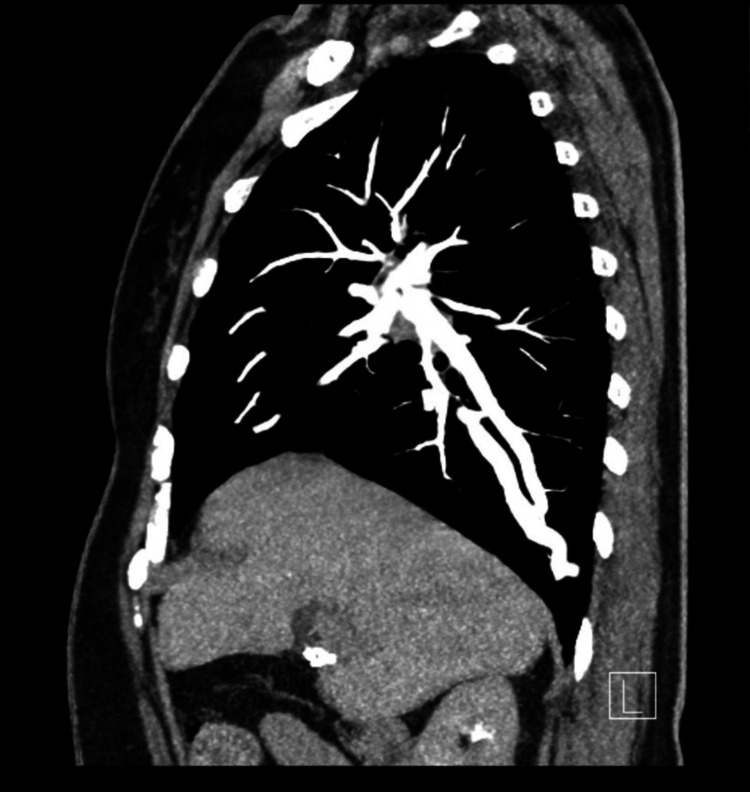 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Anomalies and Treatments · Tracheal and airway disorders · Congenital Diaphragmatic Hernia Studies
Introduction
Pulmonary arteriovenous malformation (PAVM) is characterized by the presence of abnormal pulmonary blood vessels in which there is a direct connection between arterial and venous vessels. This bypass of the capillary bed can create a low-resistance and high-flow continuous intrapulmonary right-to-left shunts (RLS), which can lead to a broad spectrum of clinical manifestations, including life-threatening hemorrhage or complications from paradoxical embolization (e.g., ischemic stroke or brain abscess) [1,2]. In patients with no clear cardioembolic source but with evidence of an RLS, paradoxical embolism should be considered. While a patent foramen ovale is a common cause, PAVMs remain an underrecognized entity, with retrospective studies showing an incidence of PAVMs in approximately 0.02% of patients with ischemic stroke [3]. Early diagnosis and management are essential to prevent recurrent cerebral ischemic events. This case emphasizes the relevance of investigating pulmonary sources of embolism when standard stroke workup is unrevealing.
Case presentation
A 57-year-old right-handed woman presented to the emergency department two hours after the sudden onset of right-sided limb weakness, trouble speaking, and facial droop. She was a smoker (more than 20 cigarettes daily for over 40 years), and had a history of arterial hypertension, dyslipidemia, previous hepatitis C virus infection, and a past of cocaine and heroin use. She had experienced several strokes in multiple territories of undetermined etiology (at that date, transthoracic echocardiogram, 24 h ambulatory electrocardiography, and transcranial Doppler ultrasound had revealed no obvious abnormality) and, since then, had been on antiplatelet therapy.
A physical examination revealed normal vital signs and glycemia, but weakness in her right upper and lower limbs (graded 4/5 according to the Medical Research Council scale), partial right facial paralysis, and severe dysarthria. Her National Institutes of Health Stroke Scale (NIHSS) score was 6, and her modified Rankin Scale (mRS) was 1. A non-contrast head computed tomography scan revealed no acute lesions, and the patient was infused with a standard dose of intravenous recombinant tissue plasminogen activator.
Subsequent vascular studies were performed and excluded the presence of luminal filling abnormalities on carotid and vertebral vessels. Brain magnetic resonance imaging revealed three ischemic acute lesions in the cortical areas of the left frontal and temporal regions. The chest X-ray showed no abnormal cardiopulmonary findings.
As part of the etiologic workup, transcranial Doppler with bubble study found significant right-to-left shunting, classified as severe (grade 4/4). Transesophageal echocardiography excluded an intracardiac shunt; however, microbubbles were observed entering the left atrium via the pulmonary veins, raising suspicion of an intrapulmonary shunt. Pulmonary CT angiography revealed a right lower lobe PAVM measuring 24×18 mm (transverse×anteroposterior) as follows: the feeding artery, originating from the right pulmonary artery, had a maximum upstream diameter of 6 mm, while the draining pulmonary vein measured 7 mm (Figure 1).
CT angiography revealed a right lower lobe PAVM.PAVM: pulmonary arteriovenous malformations
Pulmonary angiography confirmed a high-flow PAVM. Superselective catheterization of the right lower lobar pulmonary artery and basal segmental branch demonstrated a feeding artery with a distal diameter of 5 mm and a mid-segment diameter of 6 mm with no other vascular malformations identified (Figure 2).
Pulmonary angiography confirmed a high-flow PAVM.PAVM: pulmonary arteriovenous malformations
Selective catheterization of the right pulmonary artery and the feeding artery of the right posterior basal PAVM was performed. An Amplatzer Vascular Plug 4 (St. Paul, MN: Abbott) (8×13.5 mm) was deployed, and control angiography confirmed successful endovascular exclusion of the PAVM (Figure 3).
Control angiography confirmed successful endovascular exclusion of the PAVM.PAVM: pulmonary arteriovenous malformations
Some causes of acquired malformations were excluded, namely cirrhosis (no parenchymal abnormalities on ultrasound and hepatic elastography of 4 kPa), pulmonary tuberculosis or other infections (CT scan showing no parenchymal disease or other abnormalities), and no prior history of trauma or surgery. Venous Doppler of the lower limbs was negative for deep vein thrombosis. Atrial fibrillation was not detected on telemetry during her hospital stay. Laboratory investigations ruled out hematological abnormalities or hypercoagulable states. Given the absence of a family history of hereditary hemorrhagic telangiectasia (HHT) and the lack of previous symptoms reported (such as nasal or other bleeding), HHT was considered unlikely, and genetic testing was not pursued.
The patient showed improvement in neurological deficits, with only slight residual weakness in the lower limb. She has maintained follow-up and underwent repeat CT angiography, which demonstrated persistent occlusion of the PAVM. To date, no new embolic events have occurred, and the patient remains on antiplatelet therapy.
Discussion
This case demonstrates a rare but significant cause of paradoxical embolism due to a pulmonary arteriovenous malformation. Most cases are associated with HHT, but isolated lesions, as in this patient, may occur [4].
According to several studies, transcranial Doppler with bubble contrast has greater sensitivity for detecting RLS than echocardiography and should be the preferred screening method [5,6]. Transesophageal echocardiography is important to distinguish between intracardiac and intrapulmonary shunt [7]. The identification of microbubbles entering the left atrium through pulmonary veins strongly supports an intrapulmonary shunt. In patients with cryptogenic stroke, particularly those with recurrent events or involving multiple arterial territories, investigation for right-to-left shunt is critical.
When a PAVM is suspected, CT angiography is the modality of choice for its diagnosis, as it allows us to characterize the lesion, identify the feeding artery, and plan a possible therapeutic intervention. Although angiography is the gold standard, it should be used only in patients at the time of endovascular treatment [8].
Treatment of PAVMs, according to several studies, is indicated when feeding arteries exceed 3 mm, regardless of the presence or absence of symptoms. Endovascular embolization is the standard of care, with excellent efficacy in preventing further neurologic events [9-12]. According to some studies, the long-term success rate of embolization is over 80% [11].
Although approximately 80% of PAVMs are congenital and therefore associated with conditions, such as HHT, when this does not appear to be the most likely underlying cause, other etiologies should be excluded, including trauma, liver cirrhosis, infections (such as fungal infections or tuberculosis), or a history of previous surgery [13]. The absence of typical HHT signs (e.g., epistaxis, mucocutaneous telangiectasia, family history) supported a non-HHT etiology in this patient. With no other embolic sources identified, the likely mechanism of stroke was paradoxical embolism through the PAVM.
Conclusions
This case highlights the importance of comprehensive evaluation of patients with cryptogenic strokes, especially when the initial investigation is inconclusive. Recognition and treatment of pulmonary shunts are crucial, as they require specific management and have significant prognostic value.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The pulmonary vascular complications of hereditary haemorrhagic telangiectasia Eur Respir J Faughnan ME Granton JT Young LH 118611943320091940705210.1183/09031936.00061308 · doi ↗ · pubmed ↗
- 2Pulmonary arteriovenous malformations associated with migraine with aura Eur Respir J Post MC van Gent MW Plokker HW 8828873420091932494810.1183/09031936.00179008 · doi ↗ · pubmed ↗
- 3Ischemic stroke in patients with pulmonary arteriovenous fistulas Stroke Topiwala KK Patel SD Pervez M Shovlin CL Alberts MJ 31131552202110.1161/STROKEAHA.120.03207334082575 · doi ↗ · pubmed ↗
- 4British Thoracic Society clinical statement on pulmonary arteriovenous malformations Thorax Shovlin CL Condliffe R Donaldson JW Kiely DG Wort SJ 115411637220172914189010.1136/thoraxjnl-2017-210764 · doi ↗ · pubmed ↗
- 5The diagnostic value of contrast-enhanced transcranial Doppler and contrast-enhanced transthoracic echocardiography for right to left shunt in patent foramen ovale: a systematic review and meta-analysis Front Neurol Zhang D Jiang L Chen YN Pan MF 15202410.3389/fneur.2024.1447964 PMC 1132703139157064 · doi ↗ · pubmed ↗
- 6Contrast-enhanced transcranial Doppler versus contrast transthoracic echocardiography for right-to-left shunt diagnosis J Clin Monit Comput Tian L Zhang M Nie H Zhang G Luo X Yuan H 114511513720233680859710.1007/s 10877-023-00979-6PMC 10520160 · doi ↗ · pubmed ↗
- 7Transcranial Doppler versus transthoracic echocardiography for the detection of patent foramen ovale in patients with cryptogenic cerebral ischemia: a systematic review and diagnostic test accuracy meta-analysis Ann Neurol Katsanos AH Psaltopoulou T Sergentanis TN 6256357920162683386410.1002/ana.24609 · doi ↗ · pubmed ↗
- 8Diagnosis and endovascular management of pulmonary arteriovenous malformations Br J Radiol Kramdhari H Valakkada J Ayyappan A 94202110.1259/bjr.20200695 PMC 824819934038182 · doi ↗ · pubmed ↗