Knowledge, Attitudes, and Practices Regarding Dengue, Vector Control, and Vaccine Acceptance Among the Mexican Population
Fortino Solorzano-Santos, Miguel Betancourt-Cravioto, Gisel Escobedo, Jorge F Mendez-Galvan, Jose G Martinez-Nuñez, Abiel H Mascareñas de los Santos, Jesus F Gonzalez-Roldan, Sarbelio Moreno-Espinosa, Jose Ramos-Castañeda

TL;DR
This study explores how much the Mexican population knows about dengue, their attitudes toward prevention, and their willingness to get vaccinated.
Contribution
The study provides insights into dengue-related knowledge, attitudes, and vaccine acceptance in Mexico using a large survey.
Findings
Most participants knew dengue could be fatal, but few understood virus types or co-infection risks.
High confidence in vaccination was reported, but concerns about safety and effectiveness were common.
Most participants would take the dengue vaccine if recommended by a doctor, but cost was a barrier for some.
Abstract
Introduction Dengue is a growing public health problem. Prevention strategies need to consider the population’s attitudes, practices, and knowledge about the disease, including its transmission and preventive measures. This study aims to analyze the results of the cross-sectional GEMKAP (Growth & Emerging Markets, Knowledge, Attitudes, and Practices) survey among the Mexican population and make recommendations for improvement. Methods A subset study of the GEMKAP survey was carried out, considering only Mexican participants. A total of 600 participants aged between 18 and 60 years were included. A web-based survey was administered from September to October 2022, with descriptive statistics applied for analysis. Results Six hundred people were evaluated; 55% were women, 39% were young adults, and 71% had at least a high school education. The scores obtained were: knowledge 48%,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
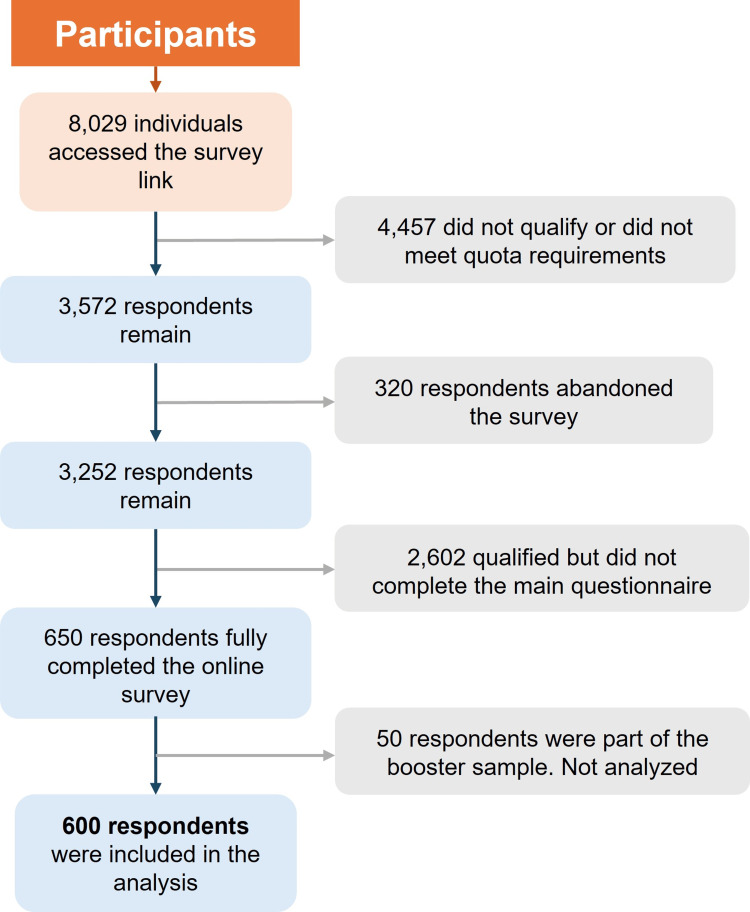 Figure 1
Figure 1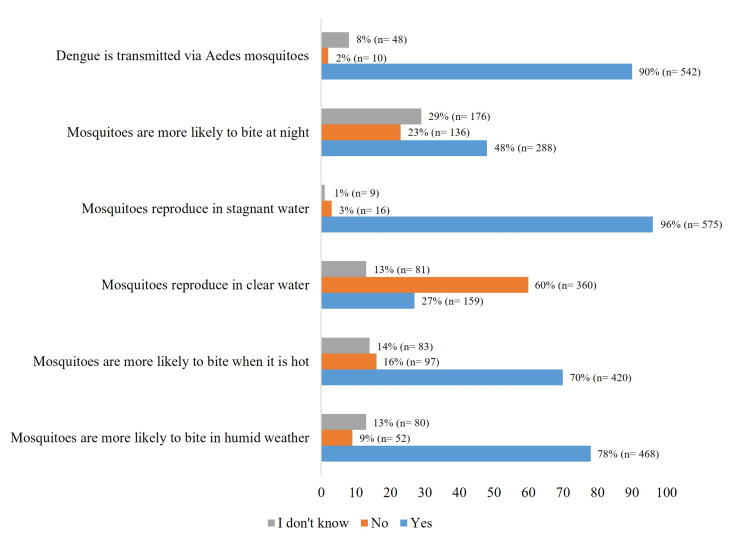 Figure 2
Figure 2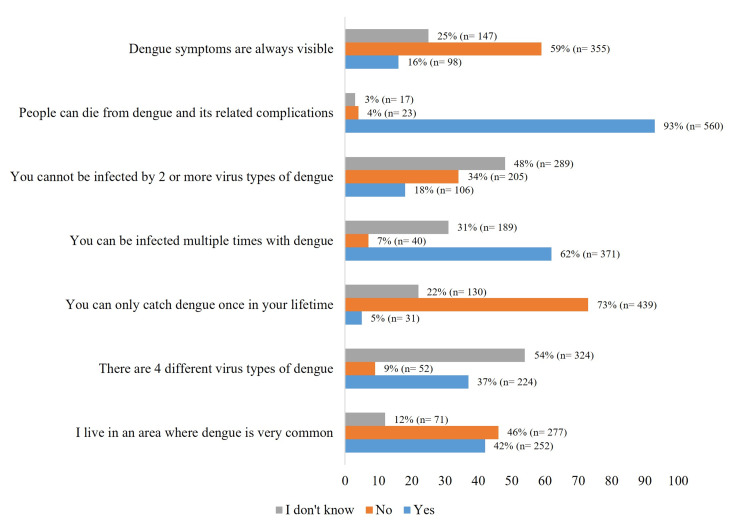 Figure 3
Figure 3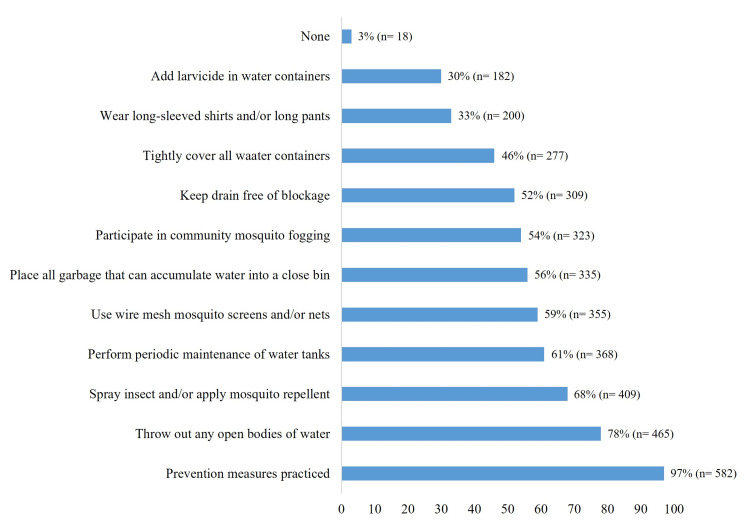 Figure 4
Figure 4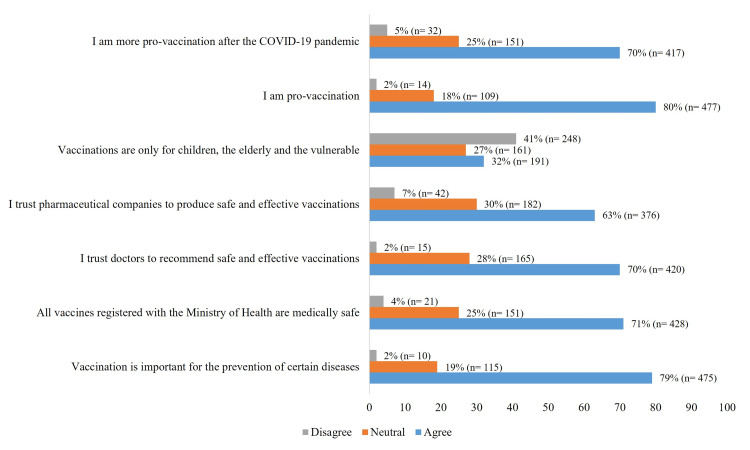 Figure 5
Figure 5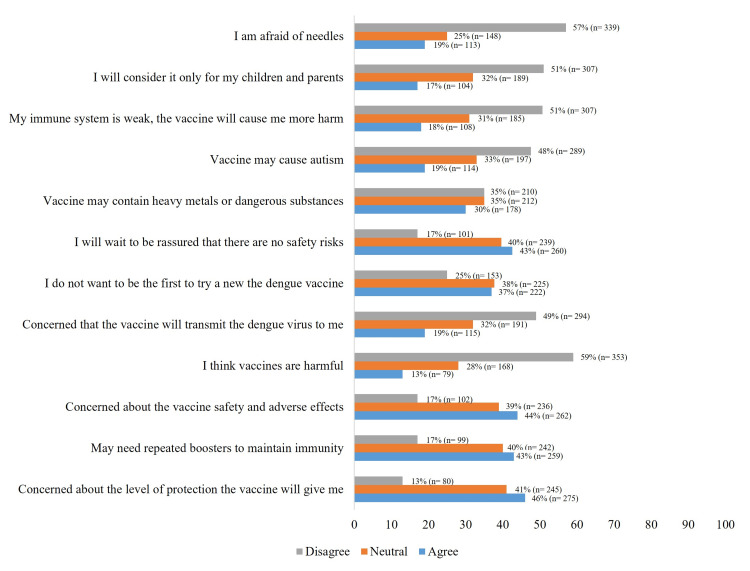 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMosquito-borne diseases and control · Viral Infections and Outbreaks Research · COVID-19 and Mental Health
Introduction
Dengue is a disease transmitted mainly by Aedes aegypti and Aedes albopictus and is a growing global public health problem [1,2]. Despite efforts to control the vector and the transmission of the virus, dengue is endemic approximately between latitude 30°N and 30°S worldwide, in what is known as the dengue belt, with recurrent outbreaks affecting millions of people each year [1,3-5]. The complexity of this disease lies not only in its biological mechanism of transmission but also in the interaction between social, economic, and environmental factors that impact the vulnerability of communities [4]. Therefore, effective strategies to prevent dengue must go beyond simple mosquito control and require modifying people’s attitudes, practices, and knowledge about the disease, including its transmission and preventive measures [1,3-5].
The scientific literature has extensively explored the relationship between knowledge, attitudes, and practices in preventing vector-borne diseases, including dengue [1,5]. PAHO issued guidelines for preventing and controlling dengue in the region, putting forward the Integrated Management Strategy for Dengue Prevention and Control (IMS-Dengue) [6]. This management model strengthens national programs aimed at reducing morbidity and mortality and the social and economic burden caused by dengue outbreaks and epidemics [6]. The model focuses on modifying individual and community behavior to diminish risk factors for transmission through coordinated measures inside and outside the health sector [6]. Previous studies have shown that a lack of information regarding the transmission of dengue and misconceptions surrounding the disease can make it difficult to implement effective preventive measures [1-3]. For example, it has been demonstrated that the exclusive use of larvicides as a vector control method is insufficient [7]. Furthermore, the perceived risk of contracting dengue, the public’s confidence in health authorities, and the availability of resources for prevention also influence the measures people take in their homes and communities [2-4].
In Mexico, an increasing trend in dengue incidence has been observed, with a notable growth in 2024. States such as Colima, Guerrero, and Tabasco have the highest rates of confirmed cases, with Colima ranking first at 140.11 cases per 100,000 inhabitants, followed by Tabasco (104.35) and Guerrero (101.83) [5,8]. In the latter, a significant increase in confirmed and estimated cases was documented, which is also reflected in the rising number of hospitalizations and severe cases reported across various states [9].
Furthermore, in Mexico, the transmission of dengue is highly variable across regions, from very low (<0.01) to incredibly high (>0.5) [10]. Notwithstanding, Mexico invests nearly half of its dengue budget in vector control strategies [11].
The Ministry of Health has confirmed that all four serotypes of the virus are currently circulating in the country, with a predominance of serotype 3 increasing the risk of severe and potentially fatal cases [9].
This increase in incidence highlights the need for preventive measures, including controlling the dengue-transmitting mosquito, raising public awareness about warning signs, and encouraging early medical attention.
This article explores the key roles of knowledge, attitudes, and practices of the Mexican population regarding dengue prevention. To this end, we conducted a sub-analysis of the data from the previously published GEMKAP (Growth & Emerging Markets, Knowledge, Attitudes, and Practices) study [12].
The aim of the study was to analyze the results of the GEMKAP survey among the Mexican population and to make recommendations for improvement.
Materials and methods
The study GEMKAP was a multi-center (Argentina, Brazil, Colombia, Mexico, Indonesia, Malaysia, and Singapore), international, cross-sectional, and observational (quantitative electronic survey) study conducted in dengue-endemic countries [12].
The GEMKAP study used the Knowledge, Attitudes, and Practices (KAP) framework to assess the level of individuals’ knowledge living in endemic areas. It explored their education about dengue and its prevention, their attitudes toward the risk of contracting dengue, the effectiveness of vector control methods, and their attitudes and practices towards community-based dengue vector control, personal prevention, and prevention through vaccination [12-15]. The study applied the Capability, Opportunity, and Motivation for Behavior Change (COM-B) framework to identify the factors correlated with accepting the dengue vaccine(s) [12,15].
Only the responses of 600 Mexican participants from all areas of Mexico, 31 out of Mexico's 32 states, were considered in this subset study during the period September to October 2022 (see Appendices 1-5). Details of the design and methodology can be found in the article by Shaffie et al. [12].
Participants
Inclusion Criteria
Potential respondents were individuals of both genders, ranging between 18 years old (legal age) and 60 years of age. The age limit was set at 60 to minimize differences in digital literacy among participants, thus reducing potential selection bias.
Exclusion Criteria
Additionally, individuals who had participated in other dengue-related surveys within the last three months were excluded, as were those who did not make decisions about their health or were not personally responsible for it.
A quota sampling procedure was applied, with strata based on gender, age, income, and regional distribution, to ensure the sample was representative of the country's gender, age, regional, and income distribution.
Most participants received an electronic invitation. To ensure adequate representation of older individuals and those living in remote areas without internet access in the total sample, respondents were recruited through local partner fieldwork agencies, inviting them to complete the survey at a partner center.
Instrument
A 35-item survey (binary answers (true/false), Likert scale, multiple-choice, and open-ended questions) previously published as material supplementary in Shaffie et al.'s study [12] was used. It took approximately 30 minutes to complete. The survey was designed in English and then translated into the native language of each country. The survey incorporated both frameworks: (i) KAP framework, aimed at identifying, understanding, and measuring misconceptions that could pose obstacles to activities or potential barriers to behavior change toward vaccination; (ii) COM-B framework, aimed at identifying factors that may influence individuals' capability, opportunity, and motivation, which can drive behavioral change for successful vaccine adoption [12].
Overall K, A, and P composite scores were also derived and standardized to a scale of 0-100%. For K, A, and P scores, 80-100% was considered a “high” score, 50-80% a “moderate” score, and 50% or below a “low” score. For attitude scores, a higher score indicated a more positive attitude [12].
The primary outcome sought was the respondents' willingness to receive the dengue vaccine. The study's secondary outcome was the general knowledge, attitudes, and practices regarding dengue infection and symptoms, dengue prevention methods, and dengue vaccines. For this report, four sections were considered: knowledge about dengue, general dengue prevention, prevention of diseases through vaccination, and prevention of dengue through vaccination.
Statistical analysis
Sociodemographic variables, other baseline characteristics, and primary and secondary outcome variables were reported descriptively using simple frequencies and percentages for categorical variables and the mean for continuous variables.
Ethics and data confidentiality
This subset study adhered to the scope detailed in the informed consent form signed by participants; therefore, it does not require Institutional Review Board (IRB) approval. Nonetheless, the primary project received approval from the Pearl Institutional Review Board (IN, USA; study number 22-VIST-101). Participants who completed the full survey received an incentive in the form of points that could be exchanged for a small prize.
Results
Sociodemographic characteristics of the participants
Out of 8,029 individuals who accessed the survey link from them 4,457 did not qualify or did not meet quota requirements; 320 respondents abandoned the survey during the screening test or main questionnaire; 2,602 qualified but did not complete the main questionnaire because the quota had already been filled; 600 respondents fully completed the online survey and were included in the analysis; and 50 respondents formed a booster sample but were excluded from the analysis (Figure 1). Among the 600 analyzed participants, 55% were women, 39% were young adults, 71% had at least a high school education, and 83% reported low (less than 9,000 Mexican pesos per month) to middle-income levels (from 9,000 to 39,000 Mexican pesos per month).
Participant flow diagram.
Regarding vaccination history, 94% reported having been vaccinated against COVID-19, and 76% had received the influenza vaccine. Questions about vaccination for dengue prevention and yellow fever prevention were not included. Additionally, 156 (26%) of respondents reported having previously contracted dengue.
Knowledge about dengue
Knowledge regarding the dengue vector was inconsistent. While most respondents were aware of the mosquito, fewer understood that it breeds in clear water, and less than 50% knew that the mosquito bites primarily during the afternoon and evening (Figure 2).
Dengue transmission statements.The data have been represented as percentage (n=number of participants).
Regarding the dengue virus, only 37% knew that there are four types of dengue virus; 34% were aware that co-infection with two or more types of the virus was possible; 62% knew that a person could be infected with the virus multiple times; and 93% knew that dengue could be fatal (Figure 3).
Dengue infection statements.The data have been represented as percentage (n=number of participants).
Most (71%) considered dengue a severe illness, and almost half of the respondents (44%) believed anyone could get infected. The population demonstrated a moderate level of knowledge about diagnostic methods. Sixty-nine percent correctly identified blood tests as the diagnostic method for dengue.
In terms of clinical presentation, the three most recognized symptoms of dengue were fever (90%), headaches (79%), and generalized pain (76%).
The most recognized consequences of dengue were potential medical visits (59%), potential hospitalization (57%), absenteeism (51%), and unexpected medical expenses (46%). The questionnaire did not ask whether death was a perceived consequence of dengue. However, awareness of secondary consequences was low. Only 11% recognized the impact on quality of life, 20% acknowledged a higher risk of reinfection, and 21% understood the potential severity of reinfection.
General dengue prevention
The majority (97%) of respondents reported practicing the 10 dengue preventive measures recommended by the Centers for Disease Control and Prevention (CDC) [16-20]. The most commonly implemented actions included eliminating standing water (78%), using insecticides or mosquito repellents (68%), regularly maintaining water tanks (61%), and installing mosquito screens or nets (59%) (Figure 4).
Frequency of prevention measures practices.The data have been represented as percentage (n=number of participants).
Prevention of diseases through vaccination
Overall, confidence in vaccination as a preventive measure against diseases was high (79%). Trust in the Ministry of Health and clinicians is similarly strong, at 70%. Confidence in the pharmaceutical industry as a producer of safe and effective vaccines is lower (63%); 32% of respondents believe that vaccination was primarily for children, older adults, and vulnerable populations (Figure 5).
Impression of vaccines (general vaccines).The data have been represented as percentage (n=number of participants).
Seventy-seven percent ensure their children are up to date with their vaccination schedules, 68% proactively ask their clinicians about vaccines, and, in turn, clinicians recommend vaccinations for various conditions (64%).
The respondents' views on government vaccination measures were as follows: 61% agree that the government facilitates access to vaccines by providing convenient vaccination sites; 59% feel the government’s promotion of vaccination is low; and 51% believe that the government promotes the importance of vaccination. The decision to get vaccinated against influenza was primarily influenced by the vaccine being free (79%) and by awareness of the potential risks associated with not getting vaccinated (65%). In contrast, the factors that least influenced the decision to get vaccinated were material incentives (3%) and knowing someone who had an adverse reaction to the influenza vaccine (14%).
The primary reasons for not getting the influenza vaccine were fear of side effects (28%), difficulty in scheduling an appointment (15%), and the cost of the vaccine (13%).
Dengue prevention through vaccination
Key concerns about the dengue vaccine included its effectiveness (46%), safety (44%), the need for booster doses (43%), and the assurance of no adverse reactions (43%) (Figure 6).
Impression of vaccines (dengue vaccine).The data have been represented as percentage (n=number of participants).
The majority (80%) believe that the vaccine should be available to the entire population, and 59% trust that health institutions and clinicians can manage both the administration of the vaccine and any adverse reactions to it. Nearly a quarter of the population (24%) would not get the vaccine if they had to pay for it.
Sixty-five percent of respondents would get vaccinated to prevent dengue if their clinician recommended it.
Most of the population (70%) believes that an education campaign should accompany the dengue vaccination program, and 32% also feel that it should be paired with a vector control program.
The reasons the population gave for getting vaccinated against dengue were to prevent it (31%), to protect their health and well-being (25%), and to protect their family (18%).
Conversely, the reasons reported for not getting vaccinated were adverse events (19%), lack of scientific evidence (7%), and lack of efficacy (5%).
The preferred channels for obtaining health information were search engines (81%), social networks (59%), and television (41%).
The survey question results for the Mexican population can be found in Appendices 1-5.
Discussion
The global scores for each component of the KAP and COM-B frameworks in the GEMKAP study among the Mexican population were moderate (for interpretation, see reference [12]): knowledge 48%, attitudes 68%, practices 42%, capability 55%, opportunity 61%, and motivation 58%. These results underscore the need for population-level education on dengue and its prevention [12]. Considering the complexity of the elements involved in calculating these scores, analyzing the responses of the Mexican population could help identify areas for improvement.
The surveyed population had knowledge gaps regarding the transmission and symptoms of dengue, including certain misconceptions. This observation is consistent with the findings of Chuc et al., who reported that in Morelos, a region in central Mexico, individuals frequently confuse dengue with other infectious diseases, both in terms of its transmission and clinical presentation [4].
Vargas Navarro et al., in their systematic literature review on the general aspects of dengue and the challenges associated with technical and community participation in its eradication, identified the absence of self-directed community engagement in official prevention programs as the primary barrier to effective vector control [21]. They point out that in Mexico, vector control has historically followed a vertical preventive model, where technical government personnel are deployed to communities to inspect homes, yards, and surrounding areas to determine where larvicides (elimination) and insecticides (fogging) should be applied. Additionally, informational materials are disseminated through various media, bypassing active and self-directed participation from the communities [21]. The results of this study show that a low proportion of respondents cited community participation and self-management as useful tools for dengue control.
The Ministry of Health, through the National Center of Preventive Programs and Disease Control (CENAPRECE), published a guide based on the national by-law NOM-032-SSA2-2014, which recommends using community-based promotion as a key element for preventing and controlling dengue, and it outlines procedures to achieve these goals [22]. This guide is used by the health authorities, and they have mainly engaged communities during epidemics through large-scale "de-cluttering" campaigns, widespread distribution of printed materials, and radio and television campaigns to share information about the vector, its breeding grounds, and the disease itself. Public health efforts have traditionally focused on informing the population about the disease and its vector; however, existing public knowledge on the subject is rarely assessed [21]. As evidenced, community participation is not considered a significant and active element in the management of dengue. Therefore, it is necessary to determine the population's position on this issue (knowledge, attitudes, practices, and perception of preventive measures) to design better strategies for dengue control.
According to Vargas Navarro et al., only 33% of the reviewed literature reported on the lack of citizen participation in dengue control, citing minimal community involvement in vector elimination activities, a failure to assess public knowledge about disease prevention, and widespread reliance on routine larvicide and insecticide use as the main control strategy [21]. In contrast, the results of this study showed more participation of the community in the dengue control to prevent dengue, although, as mentioned previously, the fact that they carry them out does not mean that they trust them, as is the case with the application of larvicides. However, it is important to reinforce the community outreach, the meeting with social groups, and supervision and evaluation as mentioned in the guide to community participation in the prevention and control of vector-borne diseases [22].
The perception of dengue as a potentially severe disease, as observed in this study, contrasts with the findings of Menchaca-Armenta et al., who reported that in the general population of Hidalgo (a state with low dengue incidence), 93.1% of participants perceived the risk as low to moderate [5].
The Mongua-Rodríguez et al. study on knowledge, attitudes, and perceptions regarding the COVID-19 vaccine provides indirect information about the factors associated with vaccine hesitancy, including fear of adverse events and distrust of medical recommendations [23]. In the present study, the population showed greater confidence in vaccination, governmental health services, and the pharmaceutical industry.
Within this research, respondents showed moderate levels (50-80%) of satisfaction and confidence in the government’s ability to manage dengue. Likewise, they practiced a few prevention measures for dengue and did so infrequently. In general, studies conducted in Mexico support the following observation: Even when there is a high awareness of the severity of dengue and a high perceived risk of contracting it, the Mexican population tends to view disease control as the government's responsibility [24]. To the best of the authors' knowledge, although there has been a vaccine registry for several years, and it was available for purchase, no mass communication campaigns were carried out in the community, which could be related to this finding.
Although respondents reported greater trust in information provided by clinicians (92%) and only 25% trusted information provided by the government, it is worth noting that most of the population receives care from the public health system, and it is very likely that they were referring to institutional clinicians.
The findings of this study suggest that raising public awareness about the disease (recognition of its severity), as well as the effectiveness, safety, and benefits of the vaccine, could improve public health by increasing dengue protection, which could lead to higher vaccination rates and a reduced risk of severe dengue, hospitalizations, complications, quality-of-life impacts, and mortality. However, social media, the internet, and other media strongly influence the population, affecting the acceptance of a dengue vaccine [25].
At the same time, addressing misconceptions is essential, as many pose risks to public health - particularly two: the false sense of security that insecticide used alone interrupts dengue transmission and the mistaken belief that vaccination replaces integrated control measures when, in fact, it is just one additional tool to help prevent severe disease and deaths from dengue [26,27].
Strengths
This report is derived from the first multinational study conducted to understand knowledge, attitudes, and practices regarding dengue and its prevention. The study was designed to increase the generalizability and statistical power of the results. Online respondents underwent industry-standard quality controls, ensuring that the data collected came from reliable participants.
Limitations
The study has five potential biases.
Sampling Bias
While the sample is geographically representative, it may not accurately reflect the distribution of disease transmission or the proportion of participants from each state. For instance, the classification between endemic and non-endemic areas was not precise, as they were not further categorized into endemic, hyperendemic, and non-endemic regions.
Selection Bias
A high proportion of participants were vaccinated against dengue. The study's objectives were deliberately excluded from the participant screening questions to reduce selection bias.
Recall Bias
Due to the self-administered nature of the survey, the high percentage of people vaccinated against dengue, and the fact that different areas have different epidemic curves for the disease, recall bias may have influenced responses.
Temporal Bias
The epidemiological context in which the survey was conducted (post-COVID-19 period) might have influenced respondents' willingness to vaccinate.
Availability Bias
The population may perceive more risk during or after an outbreak, as outbreaks occur at different times in different populations.
Recommendations
In light of the results on public perceptions of dengue and its prevention and control strategies, the following recommendations are proposed.
Stronger Communication
Despite the longstanding implementation of structured information campaigns, their impact has been limited. Consequently, designing new messages and finding more effective information channels that directly address persistent misinformation and resonate with prevailing attitudes and perceptions is essential.
Policy Refinements
New health policies can formulate adjustments to dengue prevention and management strategies, addressing the identified gaps.
Building Public Trust
Fostering greater public trust in health authorities is essential to improving the impact of health messages. At the same time, the concept of shared responsibility in developing and maintaining healthy environments should be actively promoted and strengthened.
Vaccine Integration
Emphasizing the existence and potential usefulness of a safe and effective vaccine as an additional element in a multi-faceted strategy for preventing and controlling dengue.
Conclusions
Considering that this study is exploratory, it shows that the population's knowledge of the vector and the virus was inconsistent. The population had limited knowledge about the mosquito's breeding sites and feeding habits, and a lack of awareness of the existence of four virus types and the possibility of co-infection. Although the majority of respondents claimed to follow the ten recommended vector control measures, actual adherence rates were below 70% for nine of them. Regarding attitudes towards vaccination in general, the population is pro-vaccination and trusts health authorities for its implementation. Regarding the vaccine to prevent dengue, there are concerns about its level of protection, the need for boosters, and its overall safety.
This study provides a comprehensive overview of the national population’s attitudes toward dengue and its prevention, offering areas of opportunity for community education and care. Dengue control requires addressing the problem from multiple perspectives: educational, community-based, governmental, medical, and pharmaceutical.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Determining perceived self-efficacy for preventing dengue fever in two climatically diverse Mexican states: a cross-sectional study Behav Sci (Basel) Annan E Angulo-Molina A Yaacob WF Kline N Lopez-Lemus UA Haque U 12202210.3390/bs 12040094 PMC 903145535447666 · doi ↗ · pubmed ↗
- 2Cost-effectiveness of the strategies to reduce the incidence of dengue in Colima, México Int J Environ Res Public Health Mendoza-Cano O Hernandez-Suarez CM Trujillo X 14201710.3390/ijerph 14080890 PMC 558059428786919 · doi ↗ · pubmed ↗
- 3Knowledge and beliefs about dengue transmission and their relationship with prevention practices in Hermosillo, Sonora Front Public Health Arellano C Castro L Díaz-Caravantes RE Ernst KC Hayden M Reyes-Castro P 142320152609035710.3389/fpubh.2015.00142 PMC 4453268 · doi ↗ · pubmed ↗
- 4Local conditions of vulnerability associated with dengue in two communities of Morelos [Article in Spanish]Salud Publica Mex Chuc S Hurtado-Díaz M Schilmann A Riojas-Rodríguez H Rangel H González-Fernández MI 1701785520132354640810.1590/s 0036-36342013000200008 · doi ↗ · pubmed ↗
- 5Risk perception and level of knowledge of diseases transmitted by Aedes aegypti Rev Inst Med Trop Sao Paulo Menchaca-Armenta I Ocampo-Torres M Hernández-Gómez A Zamora-Cerritos K 060201810.1590/S 1678-9946201860010 PMC 596208629538507 · doi ↗ · pubmed ↗
- 6Integrated management strategy for dengue prevention and control 1 2025 Pan American Health Organization Integrated Management Strategy for Dengue Prevention and Control 2018 https://iris.paho.org/handle/10665.2/34860
- 7The influence of gender and temephos exposure on community participation in dengue prevention: a compartmental mathematical model BMC Infect Dis Alvarado-Castro VM Vargas-De-León C Paredes-Solis S 4632420243869834510.1186/s 12879-024-09341-w PMC 11067291 · doi ↗ · pubmed ↗
- 8Knowledge, attitudes, and practices regarding vector-borne diseases in central Mexico J Ethnobiol Ethnomed Nava-Doctor JE Sandoval-Ruiz CA Fernández-Crispín A 451720213428986110.1186/s 13002-021-00471-y PMC 8296709 · doi ↗ · pubmed ↗