New challenges in diagnosis and treatment of chest pain in the patient with hyperuricemia
Yubing Zhang, Dongming Han, Yuhua He, Xiaoyao Chang, Ping Lu, Tao Zhang, Yanlong Jia, Hongqin Zhuang, Zichun Hua

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
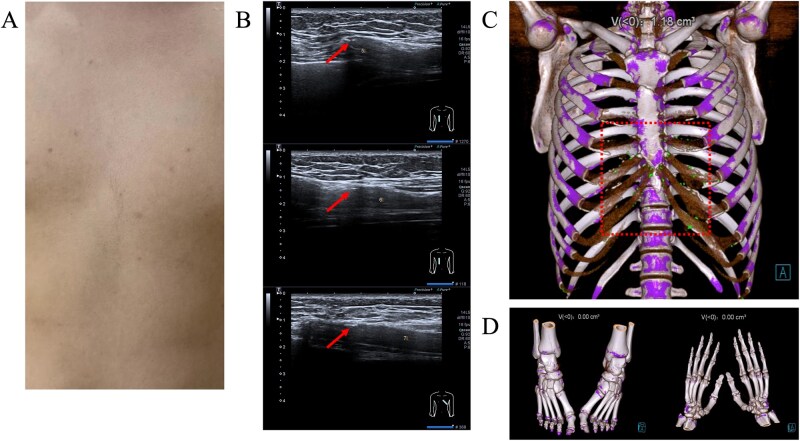 Figure 1
Figure 1- —Chinese National Natural Sciences Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGout, Hyperuricemia, Uric Acid · Trauma Management and Diagnosis · Pericarditis and Cardiac Tamponade
A 27-year-old man presented to our outpatient department with a 3-day history of acute anterior chest pain. He had a history of gout and was first diagnosed with hyperuricemia (serum uric acid level 518 μmol/l) at the age of 24. In the days leading up to this visit, he experienced daily chest pain that progressively worsened from morning to night. The pain was sharp and localized over the costal cartilage, especially on palpation.
Physical examination revealed no significant abnormalities in the lungs or heart and no visible redness or swelling was observed over the chest wall (Fig. 1A). Laboratory tests showed a mildly elevated C-reactive protein level (1.76 mg/l). Musculoskeletal ultrasound revealed dot-like echogenic foci on the costal cartilage (Fig. 1B). Dual-energy computed tomography (DECT) of the chest wall demonstrated green colorization along the costochondral cartilage, indicating the presence of monosodium urate crystals (Fig. 1C). However, DECT of the hands and feet showed no crystal deposition (Fig. 1D).
The patient was treated with etoricoxib (120 mg/day) and benzbromarone (100 mg/day), resulting in rapid pain relief within 2 days. Compared with allopurinol and febuxostat, benzbromarone demonstrates a faster absorption efficiency and a higher rate of uric acid reduction. Furthermore, there are fewer reports of adverse effects related to benzbromarone in Asian populations. Based on the evidence, we chose benzbromarone for treatment of this patient. Further documentation of similar clinical presentations and outcomes may help improve our understanding of the diagnosis and management of costochondral gout in patients. Detailed diagnosis and treatment records are presented in the supplementary materials, available at Rheumatology Advances in Practice online.
Supplementary Material
rkaf134_Supplementary_Data