The Influence of Health Literacy on the Control of Hypothyroidism in Patients Under Levothyroxine Treatment
Jessyka Krause Meneses, Daniella Araujo Muniz, Débora Moroto, João Roberto Maciel Martins, Carolina Castro Porto Silva Janovsky

TL;DR
This study shows that patients with lower health literacy have worse control of hypothyroidism, requiring higher doses of levothyroxine.
Contribution
Demonstrates health literacy as a modifiable factor affecting hypothyroidism treatment outcomes.
Findings
Lower health literacy was linked to higher TSH levels and greater levothyroxine dose requirements.
The association between health literacy and TSH remained significant in adjusted models.
No significant differences in comorbidities were found across literacy levels.
Abstract
To investigate the association between health literacy levels and biochemical control of hypothyroidism, measured by serum TSH and free thyroxine (FT4) levels, in patients receiving levothyroxine (L‐T4) therapy. We conducted a cross‐sectional study at the Thyroid Disorders Outpatient Clinic, Escola Paulista de Medicina, Universidade Federal de São Paulo (EPM/UNIFESP), between April and December 2024. The protocol was approved by the institutional ethics committee (CAAE: 76540423.5.0000.5505), and all participants provided written informed consent. Adult patients aged 18–65 years with primary hypothyroidism on levothyroxine (L‐T4) therapy were screened; 274 met eligibility criteria after exclusions. Health literacy was assessed using the Brazilian‐Portuguese Newest Vital Sign (NVS), administered face‐to‐face by trained staff. Demographic and clinical data, including comorbidities, L‐T4…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
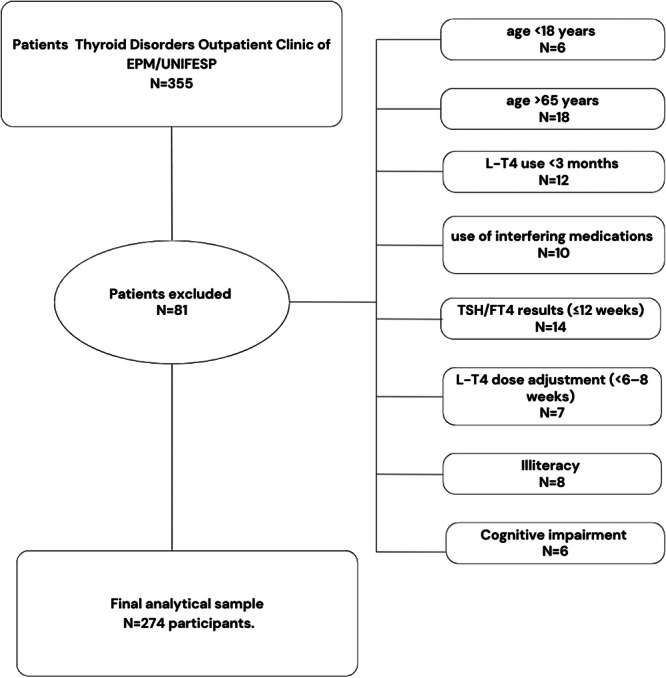 Figure 1
Figure 1 Figure 2
Figure 2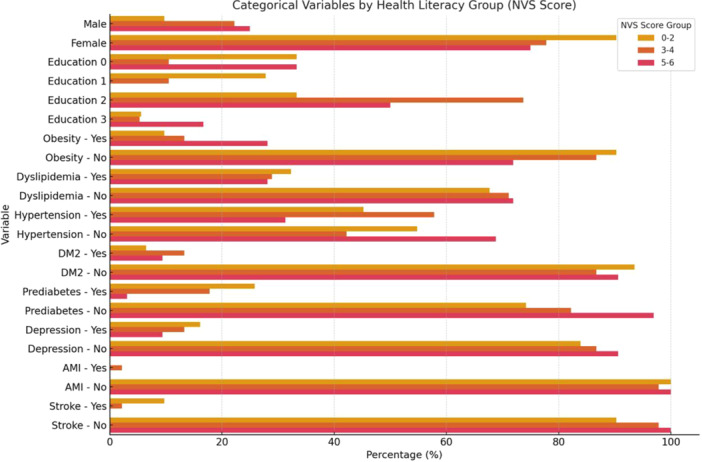 Figure 3
Figure 3| Total ( | The Newest Vital Sign Score |
| |||||||
|---|---|---|---|---|---|---|---|---|---|
| 0–2 ( | 3–4 ( | 5–6 ( | |||||||
| Age, in years (mean, SD) | 53.98 | 16.09 | 53.62a | 16.49 | 55.27a | 16.19 | 53.09a | 15.66 | 0.639 |
| TSH, in mIU/L (median, iQR) | 2.67 | 1.24–5.27 | 6.24a | 0.64–12.56 | 3.43b | 2.47–4.50 | 1.60c | 0.85–2.18 | < 0.001* |
| T4, in ng/dL (median, iQR) | 1.30 | 1.09–1.48 | 1.25a | 1.07–1.46 | 1.29a | 1.06–1.47 | 1.32a | 1.11–1.59 | 0.166* |
| Levothyroxine dosage, in µg/kg/day (median, iQR) | 1.30 | 1.09–1.48 | 1.38a | 1.06–1.81 | 1.20b | 0.91–1.51 | 1.27ab | 1.00–1.59 | 0.011* |
| Duration of diagnosis, in years (median, iQR) | 11.00 | 6.00–19.25 | 12.00a | 8.00–21.50 | 11.00a | 6.00–18.00 | 10.50a | 6.00–19.75 | 0.244 |
| N | % | N | % | N | % | N | % | ||
| Sex | 0.777 | ||||||||
| Male | 53 | 19.3% | 16 | 17.2% | 19 | 21.3% | 18 | 19.6% | |
| Female | 221 | 80.7% | 77 | 82.8% | 70 | 78.7% | 74 | 80.4% | |
| Level of Education | 0.668 | ||||||||
| Missing | 178 | 65.0% | 60 | 64.5% | 56 | 62.9% | 62 | 67.4% | |
| No schooling | 15 | 5.5% | 7 | 7.5% | 5 | 5.6% | 3 | 3.3% | |
| Elementary/Middle/High school | 66 | 24.1% | 21 | 22.6% | 25 | 28.1% | 20 | 21.7% | |
| Some college or higher | 15 | 5.5% | 5 | 5.4% | 3 | 3.4% | 7 | 7.6% | |
| Obesity | 0.647 | ||||||||
| No | 212 | 77.4% | 69 | 74.2% | 71 | 79.8% | 72 | 78.3% | |
| Yes | 62 | 22.6% | 24 | 25.8% | 18 | 20.2% | 20 | 21.7% | |
| Dyslipidaemia | 0.615 | ||||||||
| No | 180 | 65.7% | 60 | 64.5% | 56 | 62.9% | 64 | 69.6% | |
| Yes | 94 | 34.3% | 33 | 35.5% | 33 | 37.1% | 28 | 30.4% | |
| Hypertension | 0.234 | ||||||||
| No | 146 | 53.3% | 49 | 52.7% | 42 | 47.2% | 55 | 59.8% | |
| Yes | 128 | 46.7% | 44 | 47.3% | 47 | 52.8% | 37 | 40.2% | |
| DM2 | 0.657 | ||||||||
| No | 228 | 83.2% | 78 | 83.9% | 76 | 85.4% | 74 | 80.4% | |
| Yes | 46 | 16.8% | 15 | 16.1% | 13 | 14.6% | 18 | 19.6% | |
| Prediabetes | 0.216 | ||||||||
| No | 240 | 87.6% | 80 | 86.0% | 75 | 84.3% | 85 | 92.4% | |
| Yes | 34 | 12.4% | 13 | 14.0% | 14 | 15.7% | 7 | 7.6% | |
| Depression | 0.183 | ||||||||
| No | 234 | 85.4% | 75 | 80.6% | 76 | 85.4% | 83 | 90.2% | |
| Yes | 40 | 14.6% | 18 | 19.4% | 13 | 14.6% | 9 | 9.8% | |
| AMI | 0.695 | ||||||||
| No | 263 | 96.0% | 90 | 96.8% | 86 | 96.6% | 87 | 94.6% | |
| Yes | 11 | 4.0% | 3 | 3.2% | 3 | 3.4% | 5 | 5.4% | |
| History of Stroke | 0.231 | ||||||||
| No | 268 | 97.8% | 89 | 95.7% | 88 | 98.9% | 91 | 98.9% | |
| Yes | 6 | 2.2% | 4 | 4.3% | 1 | 1.1% | 1 | 1.1% | |
| Univariate | Adjusted model | |||||||
|---|---|---|---|---|---|---|---|---|
| lnTSH | B | 95% CI |
| B | 95% CI |
| ||
| Health Literacy | ||||||||
| 0–2 | Ref. | Ref. | ||||||
| 3–4 | −0.389 | −0.652 | −0.126 | 0.004 | −0.399 | −0.649 | −0.148 | 0.002 |
| 5–6 | −0.883 | −1.146 | −0.620 | < 0.001 | −0.897 | −1.153 | −0.641 | < 0.001 |
| lnT4 | ||||||||
| Health Literacy | ||||||||
| 0–2 | Ref. | Ref. | ||||||
| 3–4 | 0.064 | −0.01 | 0.139 | 0.091 | 0.071 | −0.004 | 0.145 | 0.063 |
| 5–6 | 0.053 | −0.008 | 0.115 | 0.089 | 0.061 | −0.001 | 0.122 | 0.053 |
| Levothyroxine Dose | ||||||||
| Health Literacy | ||||||||
| 0–2 | Ref. | Ref. | ||||||
| 3–4 | −0.094 | −0.161 | −0.028 | 0.006 | −0.083 | −0.144 | −0.022 | 0.008 |
| 5–6 | −0.067 | −0.131 | −0.004 | 0.038 | −0.064 | −0.124 | −0.004 | 0.038 |
- —This study was financed in part by a master's scholarship from the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil (CAPES) – Finance Code 001.
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealth Literacy and Information Accessibility · Patient-Provider Communication in Healthcare · Thyroid Disorders and Treatments
Introduction
1
Hypothyroidism is one of the most prevalent endocrine disorders worldwide, affecting ≈4.6% of the population [1, 2]. Women and older adults are disproportionately affected—a pattern also observed in Brazil [1, 2]. Characterised by insufficient thyroid‐hormone production, the condition commonly leads to fatigue, weight gain and depressive mood, all of which impair quality of life [3].
Levothyroxine (L‐T4) is the standard therapy, intended to restore metabolic homoeostasis by normalising serum thyroid‐stimulating hormone (TSH) and free thyroxine (FT4) levels [1]. Nevertheless, a considerable proportion of patients continue to report symptoms or display biochemical instability. Such difficulties may stem from impaired L‐T4 absorption, drug–drug interactions, inconsistent intake or miscommunication between patients and clinicians [3, 4, 5].
Health literacy—the capacity to obtain, process and apply health‐related information—plays a pivotal role in chronic‐disease management. It encompasses cognitive and social skills that shape how individuals interpret medical advice, navigate the healthcare system and engage in self‐care. Low health literacy has been consistently linked to reduced treatment adherence, higher healthcare utilisation and poorer clinical outcomes [2, 3, 4, 5, 6].
In hypothyroidism specifically, health literacy influences patients' understanding of correct L‐T4 use and the importance of regular TSH and FT4 monitoring [7, 8]. Individuals with limited health literacy often struggle to follow complex dosing schedules or grasp the implications of laboratory results, challenges that are aggravated by low educational attainment and restricted access to reliable information [9, 10, 11, 12]. Personalised educational interventions have shown promise in improving health literacy and, consequently, clinical outcomes—including in hypothyroidism [11, 12, 13].
Given the high prevalence of hypothyroidism and the central role of L‐T4 adherence in achieving biochemical control, clarifying the impact of health literacy is especially relevant in countries such as Brazil, where socioeconomic disparities and limited access to health information persist. Despite its clinical importance, this association remains underexplored in developing‐country settings and within public healthcare systems.
Therefore, this study aims to evaluate whether health literacy independently influences biochemical control of hypothyroidism—measured by TSH and FT4 levels—in patients receiving L‐T4 therapy within a real‐world, public healthcare setting in Brazil.
Methods
2
Study Design and Ethical Approval
2.1
A cross‐sectional study was conducted at the Thyroid Disorders Outpatient Clinic, Escola Paulista de Medicina, Universidade Federal de São Paulo (EPM/UNIFESP) from April to December 2024. The protocol was approved by the Institutional Ethics Committee (CAAE: 76540423.5.0000.5505) and complied with the Declaration of Helsinki. All participants provided written informed consent (Termo de Consentimento Livre e Esclarecido).
Participants and Sample Size
2.2
A single‐proportion formula for population‐based studies was used to calculate the sample size. To account for a 10% nonresponse rate, the final sample size was determined to be 355 patients. These adult patients with primary hypothyroidism receiving levothyroxine (L‐T4) were initially identified at the Thyroid Disorders Outpatient Clinic of EPM/UNIFESP. Of these, 81 were excluded based on predefined eligibility and data quality criteria (Figure 1). The final analytical sample therefore comprised 274 participants.
Flowchart of patient selection. Of 355 patients initially identified at the Thyroid Disorders Outpatient Clinic of EPM/UNIFESP, 81 were excluded due to predefined eligibility and data quality criteria: age < 18 years (n = 6), age > 65 years (n = 18), intermittent levothyroxine (L‐T4) use < 3 months (n = 12), use of interfering medications (n = 10), absence or out‐of‐window TSH/FT4 results ( ≤ 12 weeks) (n = 14), recent L‐T4 dose adjustment ( < 6–8 weeks) (n = 7), illiteracy (n = 8), and documented cognitive impairment (n = 6). The final analytical sample comprised 274 participants.
Inclusion Criteria
2.3
- Age 18–65 years.
- Primary hypothyroidism diagnosed ≥ 6 months earlier (clinical or subclinical).
- Continuous levothyroxine (L‐T4) therapy for ≥ 3 months.
- Recent TSH and free T4 (FT4) results ( ≤ 3 months old) available in the electronic record.
Exclusion Criteria
2.4
- Illiteracy or diagnosed cognitive disorder.
- Current use of agents that alter thyroid function or L‐T4 kinetics (e.g., amiodarone, biotin, carbamazepine, carbidopa, furosemide, haloperidol, heparin, levodopa, lithium, metoclopramide, phenytoin, propranolol, primidone, rifampin, systemic steroids, and valproic acid).
Data Collection
2.5
After consent, the Brazilian‐Portuguese Newest Vital Sign (NVS) questionnaire was administered by the same trained staff in face‐to‐face interviews. The NVS is a brief six‐item instrument that evaluates functional health literacy using a nutrition label as stimulus material. It requires participants to apply reading comprehension and numeracy skills to answer questions on serving size, calories, nutrient content, percentages, and allergy information. Each correct answer scores one point, yielding a total between 0 and 6. Scores of 0–2 indicate a high likelihood of limited health literacy, 3–4 suggest the possibility of limited literacy, and 5–6 almost always reflect adequate literacy. The instrument has been validated internationally and adapted for use in Brazilian Portuguese by Carthery‐Goulart et al. (2009), demonstrating good psychometric performance in outpatient populations. It typically requires 3–5 min to administer, making it feasible in routine clinical care. Although it provides a reliable measure of general health literacy, it does not directly capture disease‐specific behaviours related to levothyroxine therapy (e.g., fasting intake, timing of ingestion, or drug–nutrient interactions), which was considered in the interpretation of our findings. Demographic and clinical data—age, sex, education, treatment duration, comorbidities (obesity, dyslipidaemia, hypertension, type 2 diabetes, prior stroke or myocardial infarction)—were extracted from electronic records, along with the latest serum TSH and FT4 results (drawn ≤ 12 weeks earlier). L‐T4 dose (µg kg⁻¹ day⁻¹) was calculated from the current prescription and body weight.
Demographic and clinical data—age, sex, education, treatment duration, comorbidities (obesity, dyslipidaemia, hypertension, type 2 diabetes, prior stroke or myocardial infarction)—were extracted from electronic records, along with the latest serum TSH and FT4 results (drawn ≤ 12 weeks earlier). L‐T4 dose (µg kg⁻¹ day⁻¹) was calculated from the current prescription and body weight.
Laboratory Methods
2.6
Biochemical Measurements
2.6.1
Serum TSH and free thyroxine (FT4) concentrations were measured in the hospital's central laboratory using an electrochemiluminescence immunoassay (ECLIA) on a Cobas e601 analyser (Roche Diagnostics, Mannheim, Germany).
‐ TSH: Analytical sensitivity (Limit of Detection) of 0.005 mIU/L, with an inter‐assay coefficient of variation (CV) < 5%. Reference interval for euthyroid adults: 0.4–4.0 mIU/L.
‐ FT4: Analytical sensitivity (Limit of Detection) of 0.5 pmol/L, with a measuring range from 0.3 to 100 pmol/L (0.093–7.77 ng/dL). The inter‐assay CV ranged from 1.3% to 4.5%, depending on the concentration. The reference interval for euthyroid adults was 12–22 pmol/L (0.93–1.7 ng/dL), according to the manufacturer's specifications.
Quality control followed CLSI standards, and the laboratory participates in the national external‐proficiency programme. All blood samples were collected in the morning during routine outpatient visits to minimise the impact of TSH circadian variation.
Data Management
2.7
All questionnaire and laboratory data were double‐entered into REDCap® and verified for consistency.
Statistical Analysis
2.8
Continuous variables are reported as mean ± SD (when normally distributed) or median (IQR); categorical variables as counts (percentages). Normality was assessed by skewness and kurtosis (–2 to +2 acceptable). Age and treatment duration were normally distributed; TSH and FT4 were log‐transformed for analysis. Group differences across NVS strata were tested with one‐way ANOVA (continuous) or χ² (categorical).
Associations between health literacy (independent variable) and biochemical/therapeutic outcomes (TSH, FT4, and L‐T4 dose) were evaluated using generalised linear regression models. For TSH and FT4, models were adjusted sequentially for age, sex, duration of diagnosis, as well as comorbidities (dyslipidaemia, diabetes, hypertension). For the outcome L‐T4 dose per kg, obesity was not included as a covariate to avoid over‐adjustment. Univariate and fully adjusted multivariable models are reported. Model performance was assessed by Akaike (AIC) and Bayesian (BIC) information criteria and log‐likelihood statistics. All analyses were performed with IBM SPSS Statistics v30, and a two‐sided p < 0.05 was considered statistically significant.
Group differences across NVS strata were tested with one‐way ANOVA (continuous) or χ² (categorical). Associations between health literacy (independent variable) and biochemical/therapeutic outcomes (TSH, FT4, L‐T4 dose) were evaluated with generalised linear regression:
Model 1: adjusted for age, sex, and log‐diagnosis duration. Model 2: additionally adjusted for comorbidities, which were entered as categorical variables (yes/no) and included obesity, dyslipidaemia, hypertension, and type 2 diabetes. Stroke and myocardial infarction were described in the sample but not included in the multivariable model due to low prevalence.
Results
3
A total of 274 participants were included in the final analysis. The majority were female (80.7%), with a mean age of 53.98 years (SD = 16.09). Stratification by Newest Vital Sign (NVS) scores revealed that 33.9% of participants scored 0–2, 32.5% scored 3–4, and 33.6% scored 5–6 (Table 1, Figure 2).
(A) Distribution of serum TSH levels (mIU/L), (B) free T4 concentrations (ng/dL), and (C) levothyroxine dose (µg/kg/day) according to health literacy levels (Newest Vital Sign score categories: 0–2, 3–4, 5–6). Boxplots show medians, interquartile ranges, and outliers. Significant differences were observed for TSH (p < 0.001) and levothyroxine dose (p = 0.011), but not for FT4 (p = 0.166).
When comparing biochemical parameters across health literacy strata, median TSH values were significantly higher in the lowest literacy group (0–2) compared with those scoring 3–4 (p = 0.004) and 5–6 (p < 0.001). Patients who scored 3–4 had higher TSH values than those in the highest group (5–6) (p < 0.001). Patients in the lowest literacy group presented higher levothyroxine dose per kg than their counterparts in the middle group (p = 0.011), whereas FT4 did not differ significantly between groups (Table 1, Figure 2). With respect to comorbidities, clinical variables—including dyslipidaemia, hypertension, obesity, depression, prediabetes, DM2, previous myocardial infarction, and history of stroke—showed no statistically significant differences between literacy levels (all p > 0.05, Figure 3).
Distribution of categorical clinical variables across health literacy levels according to Newest Vital Sign (NVS) scores. Values are presented as percentages. AMI = acute myocardial infarction, DM2 = type 2 diabetes mellitus, NVS = Newest Vital Sign, TSH = thyroid‐stimulating hormone, T4 = thyroxine.
In multivariable regression analyses, higher health literacy was independently associated with lower serum TSH concentrations (3–4 group: β = −0.399, 95% CI −0.649; −0.148, p = 0.002; 5–6 group: β = −0.897, 95% CI −1.153; −0.641, p < 0.001) after adjustment for age, sex, duration of diagnosis, obesity, and comorbidities (dyslipidaemia, diabetes, hypertension). The association of health literacy with FT4 was marginal, showing a trend for a positive association in the fully adjusted model (β = 0.071, p = 0.063 and β = 0.061, p = 0.053 for 3–4 and 5–6 groups, respectively). A negative and significant association was observed between NVS score and levothyroxine dose per kg (3–4 group: β = −0.083, 95% CI −0.144; −0.022, p = 0.008; 5–6 group: β = −0.064, 95% CI −0.124; −0.004, p = 0.038). Results are summarised in Table 2.
Discussion
4
In this study, we found a clear and consistent relationship between health literacy and biochemical control in patients with primary hypothyroidism. Individuals with higher Newest Vital Sign (NVS) scores had lower serum TSH concentrations, and this association remained significant even after adjusting for age, sex, disease duration, and major comorbidities. Each step up in literacy appeared to move patients closer to guideline‐recommended TSH targets, highlighting how functional literacy plays a direct role in treatment success [14, 15].
This effect cannot be explained simply by years of schooling. Although education and health literacy are related, they capture different abilities. The NVS evaluates skills such as reading comprehension and numeracy, which are essential for applying medical instructions in daily life and are not always reflected by formal education. In countries like Brazil, where educational quality is uneven, this distinction becomes especially important. Our findings suggest that patient evaluation should consider functional literacy, not only reported schooling [6, 7].
We also observed that literacy levels were not associated with differences in age, sex, formal education, or the prevalence of obesity, dyslipidaemia, hypertension, diabetes, or cardiovascular disease. This strengthens the interpretation that the relationship between literacy and TSH control reflects literacy‐specific mechanisms rather than baseline clinical profile [8, 16].
Adherence to levothyroxine is the most likely explanation for the association we found. The medication requires strict routines: fasting intake, avoiding interactions with food or other drugs, and taking it at the same time each day. Patients with limited literacy may struggle with these requirements, which can lead to TSH fluctuations. We did not measure adherence directly, but prior studies show that understanding instructions, managing missed doses, and recognising interactions strongly relate to literacy levels. Adherence is probably a key mediator, though other elements—such as communication with health professionals or general self‐care skills—may also play a role [14, 16, 17].
Another relevant finding was that patients with lower literacy required higher doses of levothyroxine per kilogram. This supports the idea that irregular intake or absorption issues could contribute to biochemical instability. On the other hand, associations with FT4 were weaker and lost significance after adjustment, although a marginal trend remained. This may be explained by the greater biological variability of FT4 compared with TSH, as well as transient influences such as dietary iodine, gastrointestinal absorption, acute illness, or the use of supplements like calcium or iron. Some patients may also take levothyroxine right before blood collection, which can artificially increase FT4 levels [18].
From a clinical point of view, these findings create opportunities for simple and low‐cost strategies to improve treatment outcomes. At our clinic, we are developing educational materials in plain language to help patients understand levothyroxine use, focusing on key issues such as fasting, missed doses, and timing. These actions align with the principles of the Brazilian public health system (SUS), which values equity, access, and patient empowerment [18, 19].
This study has limitations. First, its cross‐sectional design does not allow us to establish causality. Second, health literacy was assessed using the NVS, which, although validated, measures general literacy skills rather than thyroid‐specific self‐care behaviours [20]. Third, we did not evaluate medication adherence directly, which limits our ability to confirm its mediating role. Fourth, although all blood samples for TSH were collected in the morning to reduce circadian effects, some residual variability is possible. Finally, although 355 patients were initially identified, 81 were excluded according to predefined criteria, leaving 274 in the final analysis. Even with a smaller‐than‐expected sample, the associations remained consistent and biologically plausible.
Digital tools may offer additional ways to support patients with low literacy, including voice reminders, simplified mobile apps, and pictorial instructions. Future studies should test whether tailoring these interventions to patients' literacy levels can improve adherence and biochemical control [12, 19, 21].
Addressing health literacy is a practical and cost‐effective approach to strengthening endocrine care, particularly in settings with limited resources.
Conclusion
5
In summary, limited health literacy, as measured by lower NVS scores, was independently associated with higher serum TSH in patients with primary hypothyroidism. Individuals with greater literacy not only achieved better biochemical control but also required lower doses of levothyroxine per kilogram, suggesting more efficient treatment management. By contrast, associations with FT4 were weaker and did not remain significant after adjustment. These findings position health literacy as a modifiable determinant of treatment success. Simple strategies such as plain‐language counselling, teach‐back techniques, and visual aids could help patients achieve more stable thyroid control, with potential benefits in long‐term morbidity and quality of life. Future research should explore how literacy‐sensitive approaches can be integrated into routine thyroid care at scale.
Author Contributions
Jessyka Krause Meneses: conceptualisation (lead), data curation (lead), writing – original draft (lead). Daniella Araujo Muniz: writing – review and editing (equal). Débora Moroto: writing – review and editing (equal). João Roberto Maciel Martins: writing – review and editing (equal). Carolina Castro Porto Silva Janovsky: conceptualisation (lead), supervision (lead), Project administration (lead), writing – review and editing (lead).
Conflicts of Interest
Jessyka Krause Meneses is currently employed by Merck. However, this employment commenced after the study was designed, conducted, and completed. The other authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1M. P. J. Vanderpump , “The Epidemiology of Thyroid Disease,” British Medical Bulletin 99 (2011): 39–51.21893493 10.1093/bmb/ldr 030 · doi ↗ · pubmed ↗
- 2Ministério da Saúde (BR). Prevalência de doenças da tireoide . Bol Epidemiol. Brasília (DF): Ministério da Saúde; 2020.
- 3V. Fatourechi , “Subclinical Hypothyroidism: An Update for Primary Care Physicians,” Mayo Clinic Proceedings 84, no. 1 (2009): 65–71.19121255 10.4065/84.1.65PMC 2664572 · doi ↗ · pubmed ↗
- 4J. Jonklaas , A. C. Bianco , A. J. Bauer , et al., “Guidelines for the Treatment of Hypothyroidism: Prepared by the American,” Thyroid 24, no. 12 (2014): 1670–1751.25266247 10.1089/thy.2014.0028 PMC 4267409 · doi ↗ · pubmed ↗
- 5W. M. Wiersinga , “Paradigm Shifts in Thyroid Hormone Replacement Therapies for Hypothyroidism,” Nature Reviews Endocrinology 10, no. 3 (2014): 164–174.10.1038/nrendo.2013.25824419358 · doi ↗ · pubmed ↗
- 6D. Nutbeam , “Health Literacy as a Public Health Goal: A Challenge for Contemporary Health Education and Communication Strategies,” Health Promotion International 15, no. 3 (2000): 259–267.
- 7K. Sørensen , S. Van den Broucke , J. Fullam , et al., “Health Literacy and Public Health: A Systematic Review and Integration of Definitions and Models,” BMC Public Health 12 (2012): 80.22276600 10.1186/1471-2458-12-80PMC 3292515 · doi ↗ · pubmed ↗
- 8N. D. Berkman , S. L. Sheridan , K. E. Donahue , D. J. Halpern , and K. Crotty , “Low Health Literacy and Health Outcomes: An Updated Systematic Review,” Annals of Internal Medicine 155, no. 2 (2011): 97–107.21768583 10.7326/0003-4819-155-2-201107190-00005 · doi ↗ · pubmed ↗