A Rare Case of Extranodal Rosai-Dorfman Disease Involving the Entire Colon
Pravin R Suryawanshi, Neha D Borde, Sushil S Deshpande

TL;DR
A rare case of a non-cancerous histiocytic disease affecting the entire colon in a 47-year-old man is reported and successfully treated.
Contribution
This paper presents a rare extra-nodal variant of Rosai-Dorfman Disease involving the entire colon in an adult patient.
Findings
RDD was diagnosed in a 47-year-old male with chronic abdominal symptoms and colon involvement confirmed via imaging and histology.
The patient underwent total abdominal colectomy and has remained in remission for four years.
Histopathological analysis confirmed extra-nodal RDD with transmural involvement of the colon and mesentery.
Abstract
Previously known as sinus histiocytosis accompanied by massive lymphadenopathy, Rosai-Dorfman Disease (RDD) is an extremely uncommon idiopathic histiocytic condition that does not have a malignant cause. In young patients, RDD often manifests as a painless cervical lymphadenopathy. However, some cases present as the extra-nodal variant of the disease, which might show a mass in the skin, soft tissue, nasal cavity, eye, bone, or other sites. RDD's involvement in the gastrointestinal (GI) tract is exceedingly uncommon. We reported a case of extra-nodal RDD affecting the GI tract in a 47-year-old Indian male patient who presented with chronic lower abdominal pain and constipation. On computed tomography, there was circumferential thickening of the ascending, transverse, and descending colon and recto-sigmoid junction with luminal narrowing and pericolic enlarged lymph nodes. Similar short…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
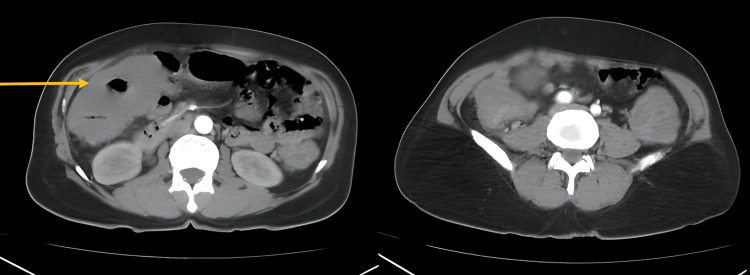 Figure 1
Figure 1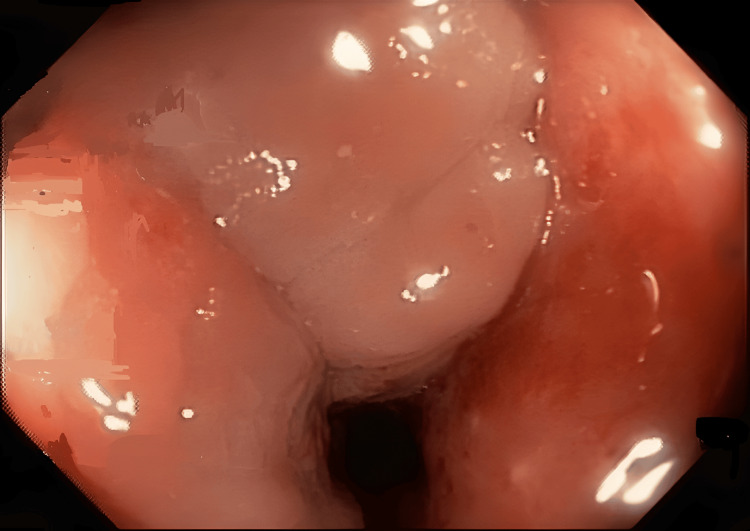 Figure 2
Figure 2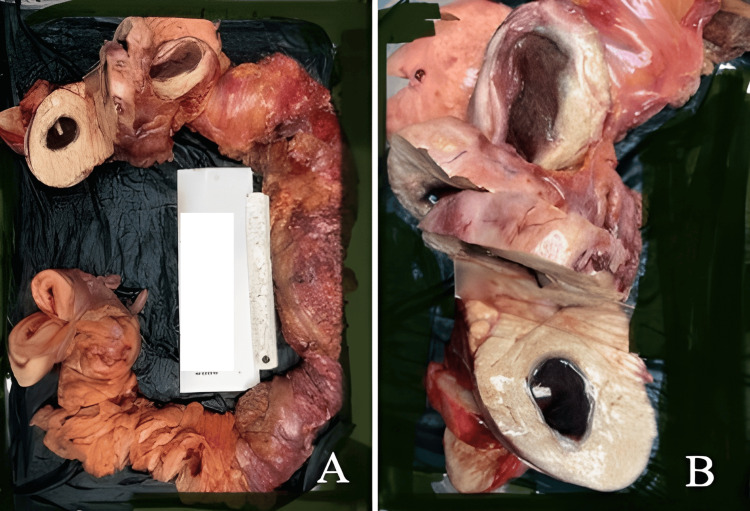 Figure 3
Figure 3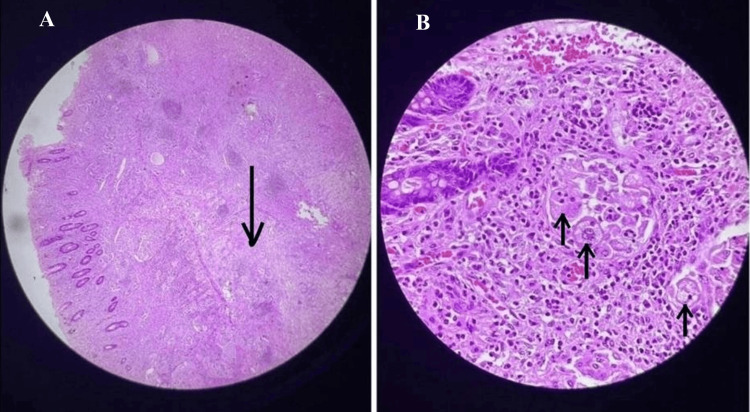 Figure 4
Figure 4|
| References | Age (years) | Sex | GI Site Involved | Other Extranodal Sites | Diagnosis Done on | Treatment Given | Outcome |
| 1 | Anders et al., 2003 [ | 51 | Female | Sigmoid colon | Lymph nodes | Post-surgery specimen | Low anterior colon resection | AWD, 15 months |
| 2 | Lauwers et al., 2000 [ | 56 | Female | Rectum | None | Colonoscopy | NA | NA |
| 3 | Lauwers et al., 2000 [ | 13 | Male | Jejunum | Bone | Autopsy | NA | DOD |
| 4 | Lauwers et al., 2000 [ | 7 | Female | Appendix | Eye (cornea) | Post-surgery specimen | Appendectomy | AWD, 11 years |
| 5 | Lauwers et al., 2000 [ | 4 | Male | Appendix | None | Colonoscopy | Segmental bowel resection | AWD, 12 years |
| 6 | Delacrétaz et al., 1991 [ | 60 | Female | Rectum | sigmoid mesocolon, abdominal wall | Post-surgery specimen | Transrectal excision of the mass | AWD, 4.5 years |
| 7 | Long et al., 2007 [ | 79 | Male | Ascending & descending colon | LNs, multiple relapse | Colonoscopy | Left Hemicolectomy | DOD |
| 8 | Nathwani et al., 2008 [ | 50 | Female | Rectum | None | Snare biopsy | NA | NA |
| 9 | Ide et al., 2010 [ | 62 | Female | Descending colon | None | Colonoscopic polypectomy | NA | NA |
| 10 | Osborne et al., 1981 [ | 53 | Female | Colon | Peritoneum | Post-surgery specimen | Right hemicolectomy | AWD, 17 months |
| 11 | Shukla et al., 2003 [ | 55 | Female | Caecum | None | Post-surgery specimen | Local resection | NA |
| 12 | Current case | 47 | Male | Whole Colon with duodenum | Lymph nodes | Post-surgery specimen | Total colectomy with ileo-anal anastomosis with Gastrojejunostomy | R, 4 years |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHistiocytic Disorders and Treatments · Tuberous Sclerosis Complex Research · Cardiac tumors and thrombi
Introduction
A non-malignant proliferation of characteristic histiocytic cells within lymph node sinuses and lymphatics at extranodal locations is a hallmark of Rosai-Dorfman Disease (RDD), a rare condition known as sinus histiocytosis with extensive lymphadenopathy [1]. In 1969, Rosai and Dorfman demonstrated it as an entirely distinct clinicopathologic entity [2]. It occurs worldwide and is primarily a disease of childhood and young adults.
Among others, axillary, para-aortic, inguinal, and mediastinal lymph nodes are commonly affected. Extranodal disease is documented in less than half of patients, with or without associated lymphadenopathy, which possibly develops later during the course of the disease. Practically, every organ system can be affected, but the most commonly affected extranodal sites include the central nervous system, skin and soft tissues, retina, the upper respiratory tract, and the skeletal system, followed by the genitourinary and lower respiratory tracts and the oral cavity. The gastrointestinal (GI) tract is the least commonly involved site [3]. This report describes a rare presentation of RDD affecting the GI tract.
Case presentation
A 47-year-old male patient presented with lower abdominal pain and chronic constipation. He was in good health till a year prior to presentation. There was no weight loss, nausea, vomiting, diarrhoea, melena, or jaundice. There was no evidence of any clinical lymphadenopathy. The patient had a known history of hypertension with well-controlled blood pressure on medication.
The patient had been undergoing treatment for the same at various institutes under the assumption of various different diagnoses, including ulcerative colitis, without any relief, and was later diagnosed with infective colitis with a component of melanosis coli and received antibiotics and laxatives, which provided symptomatic relief for a few days, but the symptoms recurred. Multiple colonoscopies were done over the year, which showed the progressive nature of the disease and lymphoplasmacytic and macrophage infiltration on biopsy, but no specific pathology. The patient had multiple episodes of subacute obstruction, which caused severe dehydration and led to acute kidney injury due to acute tubular necrosis, and was under intensive care for the same. With proper hydration and dialysis, the patient completely recovered from acute kidney injury (AKI).
The patient underwent contrast-enhanced computed tomography at our institute, which showed long-segment polypoidal circumferential thickening in the ascending, transverse, and descending colon, and rectosigmoid junction with skip areas in between, producing luminal narrowing and loss of mural stratification with enlarged pericolic lymph nodes. Similar morphology with short segment circumferential thickening of D1 and D2 was noted (Figure 1).
CT image showed short segment circumferential thickening of D1 and D2 was noted.
Colonoscopy was done, which showed luminal narrowing of the sigmoid colon with inflammatory changes in the mucosa with minimal pigmentation beyond which the scope could not be negotiated (Figure 2).
Colonoscopy image showed luminal narrowing of sigmoid colon with inflammatory changes in mucosa with minimal pigmentation beyond which scope could not be negotiated.
Since the mucosa was not showing any pathology but had significant thickening, a core needle biopsy was done, which was reported as colonic xanthomatosis. In view of significant luminal narrowing with repeated episodes of subacute obstruction and core needle biopsy of colonic xanthomatosis, the patient was planned for surgical intervention. Intra-operatively, there was evidence of bosselation along the length of the entire colon with tumor-like circumferential hypertrophy at the ceacum and proximal ascending colon, hepatic flexure, distal descending colon, and recto-sigmoid (Figure 3).
(A) Evidence of bosselation along the length of the entire colon with tumor-like circumferential hypertrophy at the ceacum and proximal ascending colon, hepatic flexure, distal descending colon and recto-sigmoid. (B) Cut surface of colon reveals firm thickened yellowish wall
Total abdominal colectomy with ileoanal anastomosis using a circular stapler and a gastro-jejunostomy. The specimen was sent for histopathological examination. The patient tolerated the procedure well. The gross histopathological examination showed irregular, yellowish, homogenous wall thickening extending from the mucosa to the serosa with no evidence of any haemorrhage or necrosis. Focal areas of infarction were noted. Microscopy revealed histiocytic disease involving the entire colon (transmurally), mesentery, and regional lymph nodes. The lesion was composed of sheets of large histiocytes with abundant foamy cytoplasm and vesicular nuclei. Numerous histiocytes also showed emperipolesis (Figure 4).
Microscopy image showing histiocytic disease involving the entire colon (transmurally), mesentery and regional lymph nodes.(A) Colon (H&E stained, 100 x magnification): submucosa is infiltrated by histiocytes (arrow); (B) (H&E stained: 400x magnification): histiocytes showing emperipolesis
Abundant lymphoplasmacytic infiltration with extensive areas of fibrosis was seen with no mitotic activity. Immunohistochemistry revealed that histiocytes were positive for S100 and CD68 but negative for c-kit. This confirmed the diagnosis of extranodal colonic RDD. The patient suffered no postoperative complications, and he was subsequently discharged. He continues to do well four years after the operation with no evidence of disease.
Discussion
Rosai and Dorfman first established sinus histiocytosis with massive lymphadenopathy (SHML or RDD) as a separate clinicopathological entity in 1969 [1]. It is primarily a disease of childhood and young adults and is characterised by insidious, slow progressive, painless lymphadenopathy, which is self-limiting [2]. Multisystem involvement is generally associated with poor prognosis. The Histiocyte Society's writing group recently updated the classification of RDD [4]. RDD has been divided into the following subtypes: extranodal, neoplasia-associated, familial, classical, and immunological disease-associated. Extranodal RDD is seen in less than 25% of cases. Every organ system can be affected by RDD, but the most commonly affected organs in the extranodal subtype include skin and soft tissues, the upper respiratory tract, and the skeletal system, followed by the genitourinary and lower respiratory tracts and the oral cavity. The GI tract is the least commonly involved site [3].
Table 1 shows the summary of 12 reported cases of extranodal RDD involving the GI system reported in English-language journals. These comprised four male and eight female patients. Two were paediatric, eight were middle-aged adults, and only two were elderly patients (over 60 years). Six cases were symptomatic with abdominal pain, abdominal mass, hematochezia, or chronic constipation. Four cases had extranodal involvement. The distal GI tract was most commonly affected. Out of 12 cases, eight underwent endoscopic evaluation, and three were diagnosed as RDD. Endoscopic procedures carried out were polypectomy, snare biopsy, and colonoscopy [5-7]. Surgical procedures carried out were right hemicolectomy, left hemicolectomy, segmental bowel resection, low anterior resection, appendecectomy, local resection, and total colectomy with gastrojejunostomy. A 4 cm transrectal mass was locally excised in one case. One case was diagnosed at autopsy. The GI sites involved were: isolated small bowel (n=1), isolated proximal colon (n=3), isolated distal colon (n=5), entire colon (n=2), colon with duodenum (n=1) [8-11].
The diagnosis of RDD is faced with great difficulty because its morphological and immunophenotypic features are somewhat similar to reactive and neoplastic diseases. The differentials include Hodgkin’s lymphoma, metastasis from various neoplasms and melanomas, malignant histiocytic neoplasm, and other inflammatory diseases. Definite diagnosis of extranodal RDD can be made by appreciating the presence of inflammatory cells and histiocytes that show emperipolesis and immunohistochemistry positive for S-100 and CD68.
The cause of RDD has been hypothesised as immune dysfunction, but it still remains unclear. The RDD histiocytes exhibit an extensive array of markers, including the S-100 protein, pan-macrophage antigens, and phagocytosis-related antigens. Nguyen et al. demonstrated that histiocytes in RDD express CD163, an acute phase-regulated transmembrane protein and hemoglobin scavenger receptor present on tissue macrophages and monocytes [12]. This finding supports the assumption that the dominant cell in RDD is activated by macrophages and is distinct from Langerhans’ cells and dendritic cells. But the definite mechanism of RDD is yet to be proven. In addition, parvovirus B19 and human herpes virus-6 have been hypothesized as contributing factors to the pathophysiology of RDD [13-15].
The closest differentials of RDD are GI xanthoma and Langerhans’ cell histiocytosis. Xanthoma presents histologically as foamy histiocytes that express CD68. As per a study by Nakasono et al. of 25 cases of rectosigmoid xanthomata [15], the histiocytosis was restricted to the lamina propria, unlike in RDD, and did not extend into the submucosa. Most of the histiocytes contained neither cell debris nor pigments in cytoplasm, and mild lymphoplasmacytic infiltration was present, which is in contrast to RDD. Langerhans’ cell histiocytosis can be differentiated from RDD by testing immunoreactivity to S-100 and CD1a; while Langerhans’ cell histiocytosis is reactive to both S-100 and CD41a, RDD is only reactive to S-100.
Treatment for RDD is not well-defined. In most patients, the disease is self-limiting. In asymptomatic patients or in patients who don’t present with involvement or compression of any major organs, no active intervention is done, and patients are asked to follow up for observation. Surgical resection is helpful in symptomatic cases with involvement of major organs.
Studies by Antonius et al. [16] and Ocheni et al. [17] suggest the use of oral corticosteroids for RDD, which has not been proven. In our case, surgical resection of the affected organ, i.e., the colon, provided symptomatic relief with no evidence of any further progression or relapse of the disease on follow-up of four years.
Conclusions
Extranodal RDD, which affects the entire colon, is an extremely rare clinical entity that presents substantial diagnostic limitations due to its inconsistent presentation and histological overlap with other inflammatory and neoplastic disorders. Histopathology and immunohistochemistry must be used for early detection in order to prevent misdiagnosis and guide subsequent necessary surgical intervention. The present case emphasizes the need to include RDD in the differential diagnosis of diffuse colonic lesions and contributes to the limited literature on this unusual manifestation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rosai-Dorfman disease presenting in the gastrointestinal tract Arch Pathol Lab Med Anders RA Keith JN Hart J 05127200310.5858/2003-127-e 74-RDDPIT 12562257 · doi ↗ · pubmed ↗
- 2The digestive system manifestations of Rosai-Dorfman disease (sinus histiocytosis with massive lymphadenopathy): review of 11 cases Hum Pathol Lauwers G Perez-Atayde A Dorfman R Rosai J 3803853120001074668310.1016/s 0046-8177(00)80254-3 · doi ↗ · pubmed ↗
- 3Sinus histiocytosis with massive lymphadenopathy (Rosai Dorfman disease) in an HIV-positive patient Virchows Arch A Pathol Anat Histopathol Delacrétaz F Meugé-Moraw C Anwar D Borisch B Chave JP 2512544191991192676710.1007/BF 01626356 · doi ↗ · pubmed ↗
- 4Revised classification of histiocytoses and neoplasms of the macrophage-dendritic cell lineages Blood Emile JF Abla O Fraitag S 2672268112720162696608910.1182/blood-2016-01-690636 PMC 5161007 · doi ↗ · pubmed ↗
- 5Intestinal occlusion caused by Rosai-Dorfman disease mimicking colonic diverticulitis Pathol Res Pract Long E Lassalle S Cheikh-Rouhou R Hofman V Lacour JP Hofman P 23323720320071740039910.1016/j.prp.2007.01.008 · doi ↗ · pubmed ↗
- 6Rosai-Dorfman disease of the colon Gastrointest Endosc Nathwani RA Kenyon L Kowalski T 1941966820081829139710.1016/j.gie.2007.11.007 · doi ↗ · pubmed ↗
- 7Rosai-Dorfman disease of the colon presented as small solitary polypoid lesion Rare Tumors Ide M Asao T Yoshida T 02201010.4081/rt.2010.e 2PMC 299448921139947 · doi ↗ · pubmed ↗
- 8Extranodal gastrointestinal sinus histiocytosis with massive lymphadenopathy. Clinically presenting as a malignant tumor Am J Surg Pathol Osborne BM Hagemeister FB Butler JJ 60361151981732527710.1097/00000478-198109000-00010 · doi ↗ · pubmed ↗