Prognostic Tools for Predicting Mortality in Older Adults With Hip Fracture: A Systematic Review
Gemma Badosa-Collell, Estel Call-Alsina, Jordi Amblàs-Novellas, Joan Carles Trullàs

TL;DR
This paper reviews tools used to predict mortality in older adults with hip fractures, finding that multidimensional assessments offer the best predictions.
Contribution
The study systematically evaluates and compares the predictive accuracy of various prognostic tools for mortality in older hip fracture patients.
Findings
The ASAgeCoGeCC score and Almelo Hip Fracture Score both showed strong 30-day mortality prediction (AUC = 0.82).
A nomogram including age and lab values predicted six-month mortality with AUC = 0.83.
The Frail-VIG index had the highest one-year mortality prediction accuracy (AUC = 0.90).
Abstract
Hip fracture (HF) is highly prevalent in older adults and is associated with functional impairment, disability, institutionalisation, increased use of healthcare resources, and mortality. Knowing the prognostic tools and identifying a gold standard to unify criteria would allow for more personalised clinical decision-making. The aim of this study is to conduct a systematic review of prognostic tools and their ability to predict mortality in patients over 65 years of age with HF. A search was conducted in the PubMed, Scopus, and Web of Science databases for studies published up to June 2022. The eligibility criteria were single-centre or multicentre studies published in English or Spanish that assessed the predictive ability of a prognostic tool for long-term mortality in patients over 65 years of age with HF. We identified 24 eligible publications. Most were single-centre observational…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
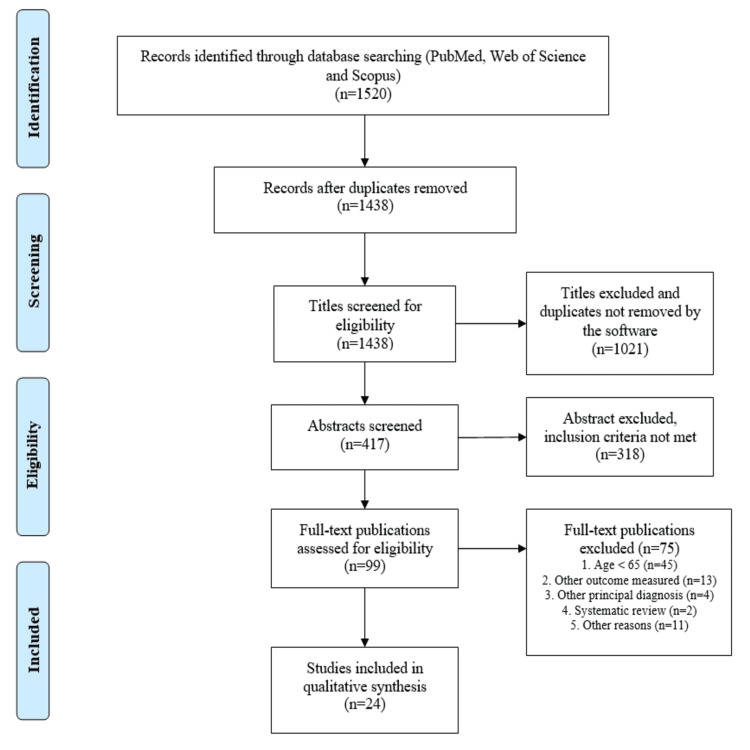 Figure 1
Figure 1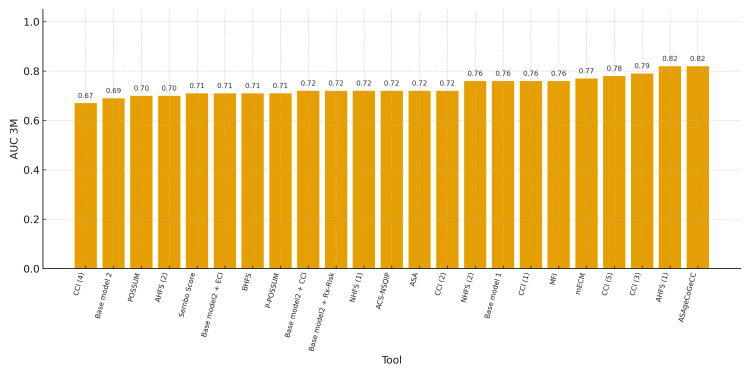 Figure 2
Figure 2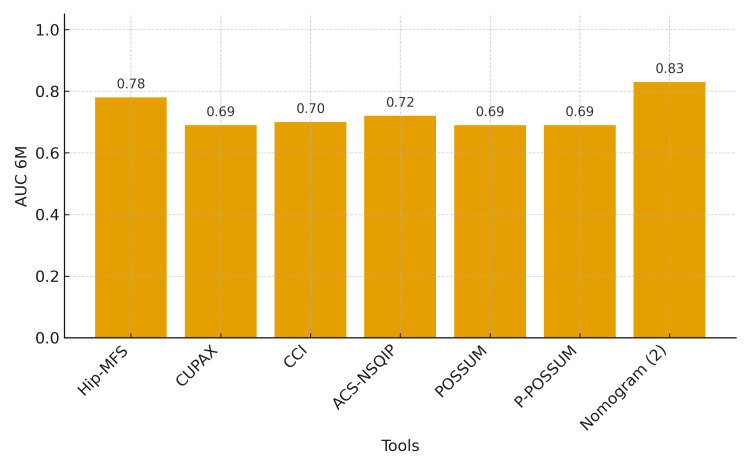 Figure 3
Figure 3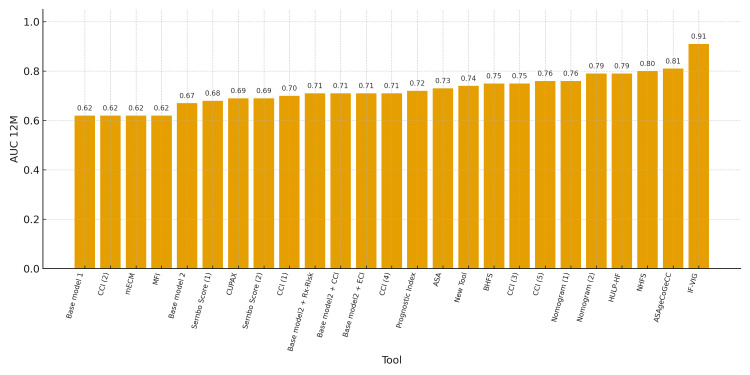 Figure 4
Figure 4| Characteristics of the publication | Number (Percentage) |
| Year of publication | |
| 2013-2015 | 3 (12%) |
| 2016-2018 | 5 (21%) |
| 2019-2022 | 16 (67%) |
| Continent/countriesᵃ | |
| Europe | 14 (58.3%) |
| Asia | 6 (25%) |
| Americas | 3 (12.5%) |
| Oceania | 1 (4%) |
| Africa | 0 (0%) |
| Study design | |
| Retrospective cohort studies | 17 (71%) |
| Prospective cohort studies | 7 (29%) |
| Sample size | |
| Median (range) | 7,421 (75-55,716) |
| <500 patients | 11 (46%) |
| 501-999 patients | 6 (25%) |
| >1000 patients | 7 (29%) |
| Main outcomes | |
| 30-day mortality | 11 (46%) |
| 6-month mortality | 5 (21%) |
| 12-month mortality | 7 (29%) |
| Secondary outcomes | |
| 6-month mortality | 2 (8%) |
| 12-month mortality | 11 (46%) |
| Author (Year, Country) [Ref] | Sample size / mean age / female | Cohort design | Prognostic tool(s) | 30-day mortality* | 6-month mortality* | 12-month mortality* | Conclusions, limitations, risk of bias |
| Badosa-Collell G et al. (2021, Spain) [ | N=103; 87 years; F: 76% | Retrospective | IF-VIG | AUC = 0.91 | IF-VIG has good predictive capacity for mortality in older adults with FF. Limitation: only patients ≥85 years. Risk of bias: moderate. | ||
| Azevedo PS et al. (2017, Brazil) [ | N=75; 80 years; F: 65% | Prospective | Goldman, Detsky, Lee | Goldman: OR 3.025 (1.022-8.953), p=0.046; Detsky: OR 2.328 (0.422-12.835), p=0.332; Lee: OR 1.262 (0.649-2.454), p=0.494 | Only the Goldman score was associated with six-month mortality. Limitations: single-centre, small sample. Risk of bias: moderate. | ||
| Cenzer IS et al. (2016, USA) [ | N=857; 84 years; F: 76% | Retrospective | Prognostic index | AUC = 0.72 | The index differentiates low- vs high-risk one-year mortality after FF. Limitation: data collected within two years before FF, not immediately pre-event. Risk of bias: serious. | ||
| Choi JY et al. (2021, South Korea) [ | N=242; 82 years; F: 73% | Retrospective | HGS, Hip-MFS, ASA | HGS: OR 1.101 (0.985-1.231), p=NS; Hip-MFS: OR 1.403 (1.027-1.917), p<0.005; ASA: OR 3.066 (1.106-8.503), p<0.005 | Hip-MFS and ASA, but not HGS, predicted 6-month mortality. Limitations: single-centre, retrospective; postoperative complications were the main outcome. Risk of bias: serious. | ||
| Choi JY et al. (2017, South Korea) [ | N=481; 80 years; F: 71% | Retrospective | Hip-MFS | AUC = 0.78; OR 1.419 (1.239-1.626), p<0.001 | Hip-MFS predicts six-month mortality after FF. Limitation: single-centre, retrospective. Risk of bias: moderate. | ||
| Crespo-Fresno A et al. (2022, Spain) [ | N=206; 87 years; F: 80% | Prospective | CUPAX | AUC = 0.69 | AUC = 0.69 | CUPAX is useful in older adults with FF. Limitation: single-centre. Risk of bias: moderate. | |
| Dawe EJ et al. (2013, UK) [ | N=259; 85 years; F: 78% | Prospective | Sernbo score | AUC = 0.71 | AUC = 0.68 | Simple tool for routine assessment to identify high-risk older adults pre-op. Limitation: only intracapsular FF. Risk of bias: low. | |
| Fu G et al. (2020, China) [ | N=702; 77 years; F: 77% | Retrospective | Nomogram | AUC = 0.76 | Nomogram predicts one-year mortality and walking ability pre-op in FF slated for arthroplasty. Limitations: single-centre, retrospective. Risk of bias: serious. | ||
| Garabano G et al. (2021, Argentina) [ | N=135; 87 years; NA | Retrospective | CCI | AUC = 0.70 | CCI suitable for one-year mortality. Limitations: small sample; retrospective; valid only for ≥75 years with unstable intertrochanteric FF. Risk of bias: moderate. | ||
| Guo J et al. (2021, China) [ | N=2,241; 79 years; F: 68% | Retrospective | Base model vs CCI, mECM, MFI | AUC = 0.76 / 0.76 / 0.77 / 0.76 | AUC = 0.62 for all scores | Base model showed good discrimination for all-cause mortality. Limitations: single-centre, retrospective; largest AUC below “fair” threshold. Risk of bias: moderate. | |
| Haugan K et al. (2021, Norway) [ | N=3,651; 84 years; F: 70% | Retrospective | CCI vs ASA | AUC = 0.72 / 0.72 | AUC = 0.75 / 0.73 | CCI and ASA similar predictive capacity; ASA easier to use. Limitations: single-centre, retrospective. Risk of bias: low. | |
| Hjelholt T et al. (2022, Denmark) [ | N=28,791; 82 years; F: 70% | Retrospective | New tool | AUC = 0.74 | Model is useful with information available at admission. Limitations: no cognitive assessment; retrospective. Risk of bias: low. | ||
| Lau TW et al. (2016, China) [ | N=759; 84 years; F: 72% | Retrospective | CCI | AUC = 0.79 | AUC = 0.71 | CCI correlated well with mortality. Limitations: non-operated FF excluded; single-centre, retrospective. Risk of bias: serious. | |
| Mellner C et al. (2021, Sweden) [ | N=55,716; 83 years; F: 69% | Retrospective | Sernbo score | AUC = 0.69 | Sernbo is easy to use and identifies high one-year mortality risk. Limitation: 30% missing data on cognitive impairment; retrospective. Risk of bias: moderate. | ||
| Menéndez-Colino R et al. (2020, Spain) [ | N=509; 85 years; F: 79% | Prospective | HULP-HF | AUC = 0.79 | HULP-HF slightly higher predictive capacity for one-year mortality vs prior studies. Limitation: no external validation. Risk of bias: low. | ||
| Nia A et al. (2021, Austria) [ | N=1,101; 84 years; F: 70% | Retrospective | ACS-NSQIP vs POSSUM, P-POSSUM, CCI | AUC = 0.72 / 0.70 / 0.71 / 0.67 | AUC = 0.72 / 0.69 / 0.69 / 0.70 | ACS-NSQIP best of the four. Limitations: single-centre, retrospective. Risk of bias: moderate. | |
| Nijmeijer WS et al. (2016, Netherlands) [ | N=850; 83 years; F: 74% | Prospective | Almelo Hip Fracture Score vs NHFS | AUC = 0.82 / 0.72 | AHFS more useful than NHFS for identifying frail older adults at high early-mortality risk after FF. Limitation: single-centre. Risk of bias: moderate. | ||
| Pan L et al. (2022, China) [ | N=454; 82 years; F: 73% | Retrospective | Nomogram | AUC = 0.83 | AUC = 0.79 | New nomogram shows good accuracy/usefulness post-FF. Limitations: no external validation; single-centre, retrospective. Risk of bias: moderate. | |
| Toson B et al. (2015, Australia) [ | N=47,698; NA; F: 73% | Prospective | CCI | AUC = 0.72-0.75 | AUC = 0.69-0.75 | CCI predicts 30-day and one-year mortality after FF. Limitation: data from administrative database (retrospective in nature). Risk of bias: moderate. | |
| Trevisan C et al. (2021, Italy) [ | N=323; 84 years; F: 78% | Retrospective | ASAgeCoGeCC vs CCI, NHFS | AUC = 0.82 / 0.78 / 0.76 | AUC = 0.81 / 0.76 / 0.80 | ASAgeCoGeCC showed good calibration and excellent discrimination up to 4 years after FF. Limitations: single-centre, retrospective; needs external validation. Risk of bias: moderate. | |
| van de Ree CL et al. (2019, Netherlands) [ | N=993; 82 years; F: 70% | Retrospective | Brabant Hip Fracture Score | AUC = 0.71 | AUC = 0.75 | BHFS showed acceptable discrimination and adequate calibration for 30-day and one-year mortality. Limitation: retrospective. Risk of bias: moderate. | |
| Vesterager JD et al. (2022, Denmark) [ | N=31,443; NA; F: 69% | Prospective | Base model, CCI, ECI, Rx-Risk, combinations | AUC = 0.69 / 0.72 / 0.71 / 0.72 | AUC = 0.67 / 0.71 / 0.71 / 0.71 | Highest discrimination at 30 days and one year by combining CCI and Rx-Risk with age and gender. Risk of bias: moderate. | |
| Vitale E et al. (2014, Italy) [ | N=95; 84 years; NA | Retrospective | Ortho-MPI | OR 1.05 (1.004-1.11) | Ortho-MPI could predict outcomes in older adults with FF. Limitations: small sample; single-centre; very high 6-month mortality (75%). Risk of bias: serious. | ||
| Wesdorp MA et al. (2021, Netherlands) [ | N=422; 84 years; F: 75% | Retrospective | Almelo Hip Fracture Score | AUC = 0.70 | AHFS useful and easy to use for predicting 30-day mortality after FF surgery. Limitations: single-centre; some variables collected retrospectively. Risk of bias: moderate. |
| Prognostic toolref. | Age | Gender | Comorbidities | Geriatric syndromes | Cognitive and/or emotional variables | Functional status | Analytical parameters | Other variables |
| IF-VIG [ | √ | √ | √ | √ | Socioeconomic data | |||
| Goldman score [ | √ | √ | ECG | |||||
| Detsky score [ | √ | √ | ||||||
| Lee score [ | √ | √ | ||||||
| Prognostic Index [ | √ | √ | √ | √ | √ | Socioeconomic data | ||
| Hip-MFS [ | √ | √ | √ | √ | √ | Serum albumin | ||
| Handgrip Strength [ | ||||||||
| CUPAX [ | √ | |||||||
| Sernbo score [ | √ | √ | √ | Socioeconomic data | ||||
| Nomogram [ | √ | √ | √ | √ | Serum albumin | ECG and chest X-ray | ||
| CCI [ | √ | √ | ||||||
| Base model [ | √ | √ | √ | Haemoglobin | Type of fracture | |||
| Multidimensional frailty [ | √ | √ | √ | √ | Serum albumin | |||
| ASA [ | √ | |||||||
| New tool [ | √ | √ | √ | √ | Institutionalisation; type of fracture | |||
| HULP-HF [ | √ | √ | √ | √ | √ | D vitamin and haemoglobin | ||
| ACS-NSQIP [ | √ | √ | √ | √ | ||||
| POSSUM [ | √ | √ | √ | Blood count and biochemistry | Type of fracture; ECG and chest X-ray | |||
| p-POSSUM [ | √ | √ | √ | √ | Blood count and biochemistry | Type of fracture; ECG and chest X-ray | ||
| NHFS [ | √ | √ | √ | √ | Haemoglobin | Institutionalisation | ||
| Almelo Hip Fracture Score [ | √ | √ | √ | √ | √ | Haemoglobin | Institutionalisation | |
| Nomogram [ | √ | √ | Serum albumin, Na+ and haemoglobin | |||||
| ASAgeCoGeCC [ | √ | √ | √ | √ | ||||
| Brabant Hip Fracture Score [ | √ | √ | √ | √ | Haemoglobin | Institutionalisation | ||
| Base model [ | √ | √ | ||||||
| Rx-Risk [ | √ | √ | √ | √ | ||||
| mECM and ECI [ | √ | √ | Haemoglobin | |||||
| Ortho-MPI [ | √ | √ | √ | √ | √ | √ | Haemoglobin |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHip and Femur Fractures · Bone health and osteoporosis research · Statistical Methods in Epidemiology
Introduction and background
Hip fracture (HF) is the main complication of osteoporosis and has a very high incidence in the older adult population [1]. It is associated with increased mortality, loss of function, decline in quality of life, and greater use of healthcare resources after discharge. The prevalence of HF is increasing due to population ageing, making it a matter of concern [1,2].
It is important to identify tools that can help differentiate between patients with a better or worse prognosis for survival at 12 months after an HF so as to improve outcomes. These tools are called predictive models or predictive tools. Early surgery has been shown to reduce the risk of mortality and postoperative complications. Furthermore, the preoperative assessment also presents an opportunity to stabilise patients, who often have multiple comorbidities. This can further prevent postoperative complications [3,4]. Reliable prognostic tools can be useful for effective preoperative preparation, which can subsequently reduce the risk of postoperative complications. These tools could also aid in determining the most suitable surgical and/or anaesthetic approach for each patient, thus optimising resources and improving the quality of patient care [4].
Numerous tools have been proposed in the literature to measure or predict mortality risk in order to improve the safety and well-being of older adult patients admitted with HF during the preoperative period. This study aims to conduct a systematic review of the literature to evaluate prognostic tools for mortality in patients over 65 years of age who present with an HF. It would be interesting to know if there is any tool that stands out above the others to serve as a gold standard.
Review
Methods
A systematic review was conducted of published studies investigating prognostic tools and their ability to predict mortality in patients over 65 years of age with HF. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [5] were followed during the conduct of this study, and the study protocol was registered in the PROSPERO international database of prospectively registered systematic reviews (registry number CRD42022340054) on 26 June 2022.
The inclusion criteria were: (1) single- or multicentre studies; (2) studies that evaluated a prognostic tool in patients with (any type of) HF; (3) studies that included patients older than 65 years; and (4) studies that evaluated short- or long-term mortality (one, six, and 12 months) as primary or secondary outcomes. The exclusion criteria were: (1) studies that did not provide primary data (i.e., review articles); (2) studies that included patients younger than 65 years; and (3) studies that only evaluated in-hospital mortality.
Studies were identified through a literature search in the PubMed, Scopus, and Web of Science (WOS) databases through 29 July 2022. The search terms “Hip fractures” and “Mortality” or “Survival” and “ROC curve” or “Predictive tool” or “Predictive model” were used. Only articles published in English or Spanish were included. The bibliographies of pertinent articles were also reviewed to identify additional studies.
Citations were uploaded to the Mendeley Desktop (version 1.19.8) reference manager software for title and abstract screening and data characterisation. Documents were reviewed based on title and abstract by two independent reviewers (GBC and ECA). Potentially eligible works were subsequently retrieved, and the full text was scrutinised for inclusion. A third investigator or “tiebreaker” (JCT) intervened in the event of disagreement. The data extracted included the first author’s name, year of publication, country (or countries) where the study was performed, number of patients included, mean age, gender, study design, name and description of the prognostic tool, and outcomes evaluated. An overview of the characteristics of eligible studies is shown in Table 1, and more details are provided in Table 2.
With regard to ethics, this study complies with the Declaration of Helsinki. Ethical approval and consent to participate were not applicable due to this study’s nature as a systematic literature review.
Results
Study Identification
A total of 1,520 potentially relevant publications were initially identified in the three databases (PubMed, Scopus, and WOS), as shown in the PRISMA flow diagram in Figure 1. After the initial screening, 1,339 articles were excluded based on title and abstract. The remaining 99 potentially relevant publications were identified for further review and, after examining these articles in greater detail, 24 were ultimately included in the systematic review.
PRISMA flow diagram showing the stages of the review and the numbers of records identified, screened, excluded, and included.PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study Characteristics
The main characteristics of the 24 studies selected are overviewed in Table 1 and detailed in Table 2. The studies were published between 2013 and 2022, and all were observational cohort studies (only seven were prospective and the remaining 17 were retrospective). They were mainly conducted in Europe. The sample sizes ranged from 75 to 55,716 patients. Overall, the mean age of the patients included in the studies was 83 years, and there was greater representation of females (70% on average). The outcome most frequently evaluated was 30-day mortality (11 studies), followed by 12- and 6-month mortality (seven and five studies, respectively). Since the results obtained in the studies are very heterogeneous, they do not allow us to conduct an in-depth subgroup meta-analysis.
Risk of Bias Assessment of Included Studies
All studies included in this review are cohort studies; therefore, we evaluated the risk of bias using the ROBINS-I scale. The seven domains of bias assessed were: confounding, patient selection, classification of interventions, deviations from intended interventions, missing data, measurement of outcomes, and selection of reported results. Overall, most studies presented a moderate risk of bias, as detailed in Table 2, particularly in the domains of patient selection (especially retrospective studies) and missing data. According to the GRADE system, the overall risk of bias was considered moderate.
Prognostic Tools for Mortality
The 24 studies included in this systematic review assessed the prognostic value of 28 prognostic tools. The characteristics and variables or domains they include are shown in Table 3. Briefly, the prognostic tools are very heterogeneous but usually share some common variables or domains [4,6-27]. Almost all the prognostic tools evaluate age and comorbidities (in 20 and 24 cases, respectively), followed by cognitive or emotional status in 15 cases, gender and analytical parameters in 13 cases, and functional status in 12. Lastly, seven prognostic tools also included an evaluation of geriatric syndromes [4,6-27].
Results for the 30-Day Mortality Outcome
Eleven studies evaluated 30-day mortality as the main outcome. As shown in Tables 2-3, the prognostic tools used to predict 30-day mortality were very heterogeneous but frequently entail evaluation of the following variables or domains: age, gender, comorbidities, cognitive and/or emotional variables, and functional status. The prognostic tools with better predictive capacity (measured by area under the curve (AUC)) for 30-day mortality were the ASAgeCoGeCC score (including the ASA score, age, gender, cognitive status, and Charlson Comorbidity Index (CCI)) [24] and the Almelo Hip Fracture Score (including age, gender, comorbidities, cognitive and functional status, haemoglobin values, and institutionalisation) [21], both with an AUC of 0.82. Figure 2 describes the predictive capacity of all the 30-day mortality prognostic tools.
3-month mortality prognostic tools.AHFS: Almelo Hip Fracture Score; ACS-NSQIP: American College of Surgeons National Surgical Quality Improvement Program; ASA: American Society of Anesthesiologists physical status classification; AUC: area under the curve; BHFS: Brabant Hip Fracture Score; CCI: Charlson Comorbidity Index; ECI: Elixhauser Comorbidity Index; mECM: modified Elixhauser Comorbidity Measure; NHFS: Nottingham Hip Fracture Score; POSSUM: Physiological and Operative Severity Score for the Enumeration of Mortality and Morbidity.Base model 1 corresponds to the tool described in reference [14], and Base model 2 corresponds to the tool described in reference [26].Three tools have been assessed and compared in more than one study, showing different AUC values: CCI1 [14], CCI2 [15], CCI3 [17], CCI4 [20], CCI5 [24]; AHFS1 [21], AHFS2 [28]; NHFS1 [21], NHFS2 [24].
Results for the Six-Month Mortality Outcome
Six-month mortality was evaluated as the main outcome in five studies and as a secondary outcome in two studies. The prognostic tools used to evaluate six-month mortality were also heterogeneous and are detailed in Tables 2-3. The tool that showed the best predictive capacity was a nomogram that included age, comorbidities, and analytical parameters (including haemoglobin, sodium, and albumin), with an AUC of 0.83 [22]. Figure 3 describes the predictive capacity of all the 6-month mortality prognostic tools.
6-month mortality prognostic tools.ACS-NSQIP: American College of Surgeons National Surgical Quality Improvement Program; AUC: area under the curve; CCI: Charlson Comorbidity Index; CUPAX: Universal Questionnaire of Previous Extraordinary Activity; Hip-MFS: Hip Multidimensional Frailty Score; POSSUM: Physiological and Operative Severity Score for the Enumeration of Mortality and Morbidity.Nomogram 2 corresponds to reference [22].
Results for the 12-Month Mortality Outcome
Lastly, eighteen studies evaluated 12-month mortality: seven as the primary outcome and eleven as a secondary outcome. As with the other outcomes, the tools used to evaluate 12-month mortality are heterogeneous but share common variables or dimensions (Tables 2-3). The Frail-VIG index [4] (which includes 22 variables from five domains: clinical, nutritional, functional, cognitive, and social) had the highest predictive capacity for one-year mortality, with an AUC of 0.91. Figure 4 describes the predictive capacity of all the 12-month mortality prognostic tools.
12-month mortality prognostic tools.ASA: American Society of Anesthesiologists physical status classification; AUC: area under the curve; BHFS: Brabant Hip Fracture Score; CCI: Charlson Comorbidity Index; CUPAX: Universal Questionnaire of Previous Extraordinary Activity; ECI: Elixhauser Comorbidity Index; Hip-MFS: Hip Multidimensional Frailty Score; HULP-HF: Hospital Universitario La Paz-Hip Fracture Score; IF-VIG: Frail-VIG index; mECM: modified Elixhauser Comorbidity Measure; NHFS: Nottingham Hip Fracture Score; POSSUM: Physiological and Operative Severity Score for the Enumeration of Mortality and Morbidity.Base model 1 corresponds to reference [14]; Base model 2 corresponds to reference [26]; Nomogram 1 corresponds to reference [12]; Nomogram 2 corresponds to reference [22].Two tools have been assessed and compared in more than one study, showing different AUC values: Sernbo score 1 [11], Sernbo score 2 [18]; CCI1 [13], CCI2 [14], CCI3 [15], CCI4 [17], CCI5 [24].
Discussion
The results of this systematic review show great variability in the prognostic tools used to predict mortality after an HF. Despite this heterogeneity, most prognostic tools evaluate similar variables or domains, the most common being age, comorbidities, cognitive and/or emotional status, and functional status. It should be noted that most of these studies have been carried out in Europe, possibly because there is a large older adult population and femur fracture is prevalent [29,30].
Most studies evaluated short-term mortality (at 30 days), with predictive capacity (according to the AUC) ranging from 0.64 to 0.82. The tools with the highest predictive capacity (AUC of 0.82) were the Almelo Hip Fracture Score and ASAgeCoGeCC, both of which include variables and domains that are easy to collect in clinical practice (age, gender, comorbidities, and cognitive/emotional status) [21,24]. It should be noted that there are two studies in our review that validate the Almelo tool. The Wesdorp MA et al. study shows an AUC of 0.70. Comparing the two studies, both have substantial sample sizes, although the sample in the Wesdorp MA et al. study is smaller. Additionally, in the original Almelo population [21], the high-risk group is more institutionalised and presents greater cognitive impairment than the high-risk population in the Wesdorp MA et al. study [28].
Fewer studies assessed six-month mortality using the area under the curve. A nomogram developed by Pan L et al. showed the highest predictive capacity for six-month mortality, with an AUC of 0.83. Again, this nomogram evaluates age and comorbidities as well as analytical parameters that are easy to measure in clinical practice [22].
Finally, regarding one-year mortality, the Frail-VIG index was the prognostic tool that demonstrated the highest predictive capacity, with an AUC of 0.91. The Frail-VIG index includes 22 variables from five domains (clinical, nutritional, functional, cognitive, and social) that are also easy to obtain in clinical practice [4,31].
It is striking that the Nottingham Hip Fracture Score (NHFS), a well-known and widely used score to predict mortality in patients with HF in different European countries, was not included in this systematic review [32,33]. The NHFS was not included because the studies conducted for its development and validation were carried out in patients under 65 years of age, which was an exclusion criterion for this systematic review [32,33]. However, we believe it is a useful tool. In fact, our group has published a study, after carrying out this review, demonstrating its utility in the geriatric population with hip fracture [34].
There are some limitations to this study that should be considered. First, this review included 24 articles out of the 1,520 initially identified. Despite efforts to be as comprehensive as possible, some articles may have been missed. To avoid this, the reference lists of the eligible articles were also reviewed to detect possible publications not found in the initial search. Second, this systematic review has the inherent limitations of the studies included: most studies were single-centre, retrospective cohort studies, and the prospective studies usually had small sample sizes. To increase the level of evidence of these prognostic tools, they should be tested in randomised controlled trials. Also, only published studies were included; thus, publication bias may have affected the results. Finally, most of the studies were carried out in Europe and Asia, so the results cannot be extrapolated to other continents.
In summary, this systematic review found that different tools have been tested to predict mortality after an HF. Most evaluate similar domains that are easy to obtain in clinical practice, and they usually show good predictive capacity. Despite this, it is necessary to conduct more prospective studies to assess the predictive capacity of these tools in larger populations.
Conclusions
There is a considerable number of studies evaluating mortality prediction in patients with hip fracture; however, most are retrospective and have small sample sizes. Despite this, we observed considerable variability in tools for predicting mortality in older adults with hip fracture. Those with greater predictive capacity are multidimensional assessments that take into account age, comorbidities, and cognitive and functional status.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Registro Nacional de Fracturas de Cadera (RNFC). Informe Anual 2018 Spain López PS González Montalvo JI Thies CO Campelo PG Madrid RNFC/Idi PAZ 112018 https://rnfc.es/wp-content/uploads/2023/02/Informe-RNFC-2021.pdf
- 2Epidemiology and social costs of hip fracture Injury Veronese N Maggi S 145814604920182969973110.1016/j.injury.2018.04.015 · doi ↗ · pubmed ↗
- 3Application of POSSUM and P-POSSUM scores in the risk assessment of elderly hip fracture surgery: systematic review and meta-analysis J Orthop Surg Res Wanjiang F Xiaobo Z Xin W Ye M Lihua H Jianlong W 2551720223552601510.1186/s 13018-022-03134-0PMC 9077349 · doi ↗ · pubmed ↗
- 4[Predictive capacity for mortality of the Frail-VIG index (IF-VIG) in old patients with hip fracture]Rev Esp Geriatr Gerontol Badosa-Collell G Latorre-Vallbona N Martori JC Oller R Trullàs JC Amblàs-Novellas J 2202235720223566026210.1016/j.regg.2022.05.002 · doi ↗ · pubmed ↗
- 5The PRISMA 2020 statement: an updated guideline for reporting systematic reviews BMJ Page MJ Mc Kenzie JE Bossuyt PM 0372202110.1186/s 13643-021-01626-4PMC 800853933781348 · doi ↗ · pubmed ↗
- 6Goldman score, but not Detsky or Lee indices, predicts mortality 6 months after hip fracture BMC Musculoskelet Disord Azevedo PS Gumieiro DN Polegato BF 1341820172837259310.1186/s 12891-017-1480-x PMC 5379496 · doi ↗ · pubmed ↗
- 7One-year mortality after hip fracture: development and validation of a prognostic index J Am Geriatr Soc Cenzer IS Tang V Boscardin WJ 186318686420162729557810.1111/jgs.14237 PMC 5026872 · doi ↗ · pubmed ↗
- 8How does the multidimensional frailty score compare with grip strength for predicting outcomes after hip fracture surgery in older patients? A retrospective cohort study BMC Geriatr Choi JY Kim JK Kim KI Lee YK Koo KH Kim CH 2342120213382744410.1186/s 12877-021-02150-9PMC 8028224 · doi ↗ · pubmed ↗